22 April 2022: Articles 
A 15-Year Change of an Adrenal Endothelial Cyst
Challenging differential diagnosis, Rare disease
Min-Jui Wu1ABCDEF, Meng-Hung Shih12ADE, Chin-Li Chen1BF, En Meng1ACF*DOI: 10.12659/AJCR.935053
Am J Case Rep 2022; 23:e935053






Abstract
BACKGROUND: Adrenal gland cysts are rare and often occur without any symptoms. Even with advanced imaging modalities, it is still difficult to differentiate a benign adrenal neoplasm from a malignant one. Therefore, it is difficult to arrive at a definitive diagnosis and provide treatment.
CASE REPORT: We describe a patient with asymptomatic adrenal incidentaloma. The patient was lost to follow-up until 7 years later. On resuming follow-up, an enlarged suprarenal tumor was noted on ultrasound imaging. Magnetic resonance imaging revealed a 6×4 cm tumor mass, and the peripheral part expressed progressive enhancement on dynamic contrast-enhanced images. Laboratory data showed slight hypokalemia, and a complete endocrine assessment was performed, which showed no abnormality. Because malignancy of the adrenal gland remained suspected, a laparoscopic adenectomy was performed. The pathological result showed an adrenal endothelial (vascular) cyst with the formation of thrombi and calcification, without any evidence of malignancy.
CONCLUSIONS: Adrenal cystic lesions can change with time. Routine imaging studies during follow-up are recommended, and endocrine evaluations should be performed as an initial adrenal tumor work-up. Surgery is the treatment of choice when the cyst is >6 cm in size, malignancy is suspected, or abnormal endocrine activity is present.
Keywords: Adrenal Gland Diseases, Adrenal Gland Neoplasms, Adrenocortical Adenoma, Adrenalectomy, Adrenal Glands, Cysts, Humans, Magnetic Resonance Imaging, Ultrasonography
Background
Adrenal gland cysts are rare and often do not present any symptoms. However, nonspecific symptoms, such as abdominal or flank pain, can occur when the tumors become large enough to compress adjacent organs [1]. Even with advanced imaging modalities, it is still difficult to differentiate a benign adrenal neoplasm from a malignant neoplasm. Hence, determining a definitive diagnosis and providing treatment is difficult. We present a case of a 76-year-old man who was incidentally found to have a suspected cystic neoplasm of the adrenal gland and underwent adrenalectomy after a 15-year follow-up period.
Case Report
A 76-year-old man presented to our outpatient department for asymptomatic adrenal incidentaloma (size, 6×4 cm). According to the patient history, he was diagnosed with a left adrenal lesion 15 years ago. Physical examination revealed no apparent abnormalities, including cushingoid symptoms. The initial abdominal sonography indicated a hypoechoic nodule in the left suprarenal region. Abdominal computed tomography (CT) (Figure 1A) showed a lesion over the left adrenal gland with a Hounsfield unit value of 40 and ring enhancement; malignancy was suspected. An abdominopelvic magnetic resonance image (MRI) (Figure 1B) revealed a well-defined, round nodular lesion, measuring 3.84 cm, over the left suprarenal region with 2 different signals. The central part had a relatively high signal but no significant contrast medium enhancement; however, the peripheral section showed moderate contrast medium enhancement. The whole nodule did not decrease signal intensity on the out-phase images when compared with that on the in-phase images. During regular follow-up evaluations, every 6 months for 8 years, abdominal ultrasound images showed no noticeable changes in the nodule.
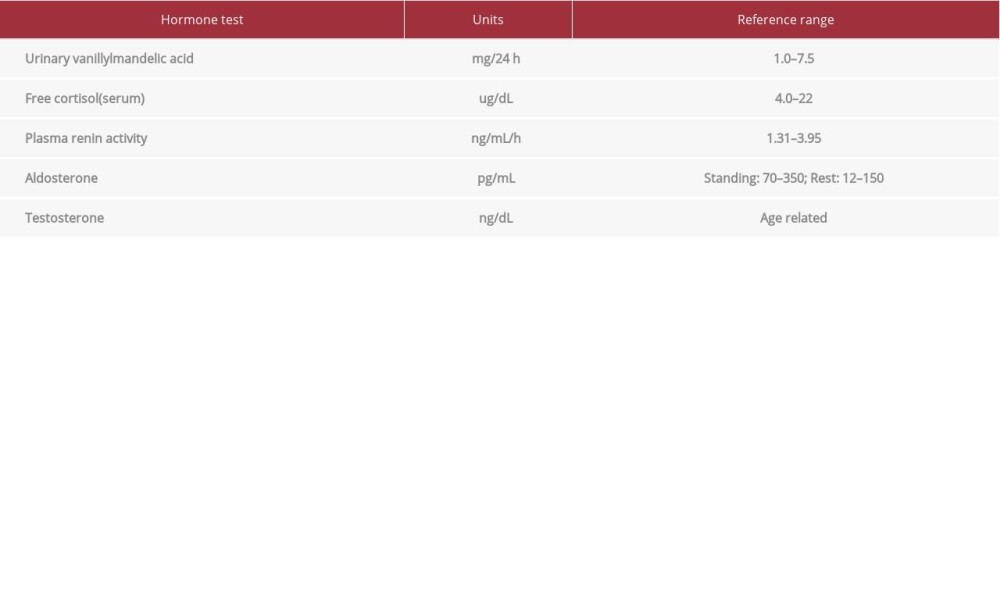
The patient was lost to follow-up until 7 years later. No abdominal pain, other discomforts, or palpable masses were present on the flank or abdominal wall. Laboratory data showed slight hypokalemia (2.9 mmol/L), while the results of the remaining blood tests and urinalysis were all within the reference ranges. No specific medication was administered to the patient. A complete endocrine assessment was performed, including the estimation of urinary vanillylmandelic acid (3.5 mg/24 h), serum cortisol (8.39 ug/dL), plasma renin activity (0.56 ng/mL/h), aldosterone (133.9 pg/mL), and testosterone (201 ng/dL). The normal test ranges are presented in Table 1. These tests showed no hormonal hypersecretion. Upon the patient resuming follow-up, an enlarged suprarenal tumor was noted on ultrasound imaging. MRI revealed a tumor mass measuring 6×4 cm (Figure 2A). The central part of the tumor resembled a hematoma, and progressive enhancement on the peripheral part was observed with dynamic contrast-enhanced images (Figure 2B). As malignancy of the adrenal gland was suspected, a laparoscopic adenectomy was performed.
Gross examination of the surgical specimen revealed a brown-red tumor mass with a few blood clots on the surface, measuring 6.4×4.7×3.9 cm (Figure 3A). Histopathological analysis showed an adrenal endothelial (vascular) cyst with the formation of thrombi and calcification; the adrenal parenchyma was normal without any evidence of malignancy (Figure 3B).
Discussion
Adrenal cystic lesions are uncommon and show various histo-logical changes ranging from pseudocysts to malignant cystic tumors. With cases being rarely reported and a broad range of differential diagnoses, the optimal management of adrenal cysts remains controversial.
Radiographic findings may help determine the appropriate management strategy. A cystic image with fluid content and an attenuation coefficient similar to water-containing calcifications (occurring in up to 15% of cases) may suggest an adrenal cyst [2]. Although the cystic nature of these lesions can be demonstrated on ultrasonography, CT, and MRI scans, their histologic type cannot be predicted. Moreover, a small series of cystic neoplasms have been reported. Patients with these cystic lesions may present with inimical clinical features associated with a malignant neoplasm; however, the lesions radiologically mimic benign lesions [1].
When radiological features suggest a benign, non-secreting cyst <4 cm in size, regular monitoring is recommended to detect changes in the nature or size of the lesion. Indications for surgery include a tumor size >6 cm, suspected malignancy, progressive growth, or endocrine activity of the cyst. Although cystic adrenocortical carcinoma and functional cystic tumors are extremely rare, it is important for a pathologist to make a diagnosis when malignancy is present [3]. An additional role of surgery has been purported to eliminate the potential risk of hemorrhage or local pressure effects of the tumor [4]. However, the therapeutic approach to masses ranging from 4 to 6 cm is unclear [5].
When an adrenal cystic lesion is discovered, a comprehensive study investigating its endocrine activity is warranted. However, the lesion might be associated with unknown endocrine disorders or potential malignancies, similar to solid tumors. The potassium level has been defined as an unreliable screening test for a functional lesion. Further endocrine tests of plasma aldosterone and plasma renin activity could help identify aldosterone-producing tumors. [6]. A few adrenal cysts have also been reported in cases of pheochromocytoma and adrenal cortical adenomas [3]. However, we should not overlook the coexistence of benign adrenal cysts and functional neoplasms or a newly developed malignancy.
For years, there has been no definite follow-up period for initially benign lesions. In our case, the patient underwent an 8-year follow-up with ultrasound imaging, which did not show any significant change in the adrenal cyst. However, after being lost to follow-up for 7 years, the images showed malignant-like change. Despite a benign pathological diagnosis, an adrenal cyst can progress after a long time. A longer period of routine follow-up should be considered, as there is a possibility of malignancy. As we suggested, an annual follow-up should include an imaging assessment. When the possibility of a cystic neoplasm diagnosis increases, monitoring of endocrine activity should be included as an initial adrenal tumor evaluation. Surgical intervention remains the appropriate management for a definite diagnosis. Although they are not the most common etiology of incidental adrenal masses, these cysts should be considered in the differential diagnosis.
Conclusions
Adrenal cystic lesions are uncommon and can range from benign cysts to cystic primary adrenal malignancy. Although it is challenging to differentiate an adrenal cyst from other adrenal neoplasms, imaging studies, including CT and MRI, are essential for defining an adrenal cystic lesion. Routine imaging during follow-up examinations is recommended because adrenal cysts can progress after a long period. Endocrine evaluations should be performed as an initial adrenal tumor evaluation. The coexistence of functional neoplasms or functional cystic lesions should be considered. Surgery is the initial treatment of choice when the cyst is >6 cm in size, malignancy is highly suspected, or abnormal endocrine activity is present.
Figures
References:
1.. Goel D, Enny L, Rana C, A report of five cases: Cancer Rep (Hoboken), 2021; 4; e1314
2.. Khan MR, Ajmal S, Saleem T, Giant adrenal endothelial cyst associated with acute and. chronic morbidity in a young female: A case report: Cases J, 2009; 2; 8841
3.. Bellantone R, Ferrante A, Raffaelli M, Adrenal cystic lesions: report of 12 surgically treated cases and review of the literature: J Endocrinol Invest, 1998; 21; 109-14
4.. Pradeep PV, Mishra AK, Aggarwal V, An institutional experience: World J Surg, 2006; 30; 1817-20
5.. Young WF, Clinical practice. The incidentally discovered adrenal mass: N Engl J Med, 2007; 356; 601-10
6.. Cavallaro G, Crocetti D, Paliotta A, Clinical and surgical management. The experience of a referral centre: Int J Surg, 2015; 13; 23-26
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133