29 March 2022: Articles 
Portal and Mesenteric Vein Thrombosis Associated with Decompression Sickness in a 48-Year-Old Deep Sea Self-Contained Underwater Breathing Apparatus (SCUBA) Diver
Unusual clinical course, Challenging differential diagnosis
Emily V. Kassar1BDEF*, Jessica R. BassDOI: 10.12659/AJCR.935473
Am J Case Rep 2022; 23:e935473






Abstract
BACKGROUND: Deep sea diving can cause decompression illness which comprises both decompression sickness and arterial gas embolism. Decompression sickness is a clinical diagnosis with symptoms including dizziness, joint pain, rash, and myalgias and is due to nitrogen bubbles that form in tissues during ascent. These gas bubbles can be clinically silent even in the absence of decompression sickness and can rarely predispose a patient to venous thrombus, for which the role of hyperbaric oxygen (HBO) is undefined. The following case describes a male diver who developed portal and mesenteric venous thrombosis secondary to silent nitrogen venous bubbles.
CASE REPORT: A 48-year-old man developed abdominal pain 1 day after diving to a maximum depth of 13.7 m, without clinical symptoms of decompression sickness after surfacing. He presented to the Emergency Department 10 days later, and magnetic resonance angiogram revealed a diagnosis of gas containing superior mesenteric and portal vein thrombus. Due to the lack of guidelines of HBO with the presence of a thrombus and timing since onset, HBO therapy was not pursued. Oral anticoagulation was initiated, and symptoms resolved.
CONCLUSIONS: This patient developed gastrointestinal illness 1 day after diving that was later found to be due to thrombosis. Other etiologies were ruled out, making silent nitrogen bubbles within the venous system the most likely etiology. Vascular thrombosis is a rare complication of diving and lacks guidelines for treatment. While HBO is a known treatment for decompression sickness, there are no clinical guidelines for diving-associated thrombi, representing an area for further research.
Keywords: Decompression Sickness, Hyperbaric Oxygenation, Venous Thrombosis, Diving, Humans, Male, mesenteric ischemia, Mesenteric Veins, Thrombosis
Background
Decompression sickness (DS) is a clinical syndrome caused by the formation of nitrogen gas bubbles in blood and tissues that occurs secondary to the rapid decrease from high to low pressures [1]. It can cause a wide variety of symptoms, including fatigue, joint pain, myalgias, and ataxia [1–3]. While most notably a disease of deep sea divers, DS can also occur when flying in unpressurized aircraft and emerging from a caisson, or in astronauts who leave their spacecraft [3]. The mainstay of treatment is recompression using hyperbaric oxygen (HBO) therapy [4]. Even in the absence of DS, clinically silent nitrogen gas bubbles can form in the venous system and rarely lead to thrombosis, for which the role of HBO is not defined [2,5]. This is a case of a 48-year-old previously healthy male diver without clinical DS who developed gastrointestinal symptoms 1 day after diving and was later found to have a gas-containing portal and superior mesenteric venous thrombosis.
Case Report
A 48-year-old man presented to the Emergency Department (ED) with diffuse abdominal pain, bloating, nausea, and inability to tolerate oral intake 10 days after diving in the Bahamas on the second day of a 5-day diving trip. He was a professional deep sea diver with over 1000 prior diving events without major complications. He reported diving 4 times to a depth of 13.7 m for 1 h per dive the day prior to symptom onset. The surface interval between dives was between 45 min and 1 h. His ascent rate was roughly 1.2 m per min, and he performed a 3-min safety stop when between 4.6 and 6 m from the surface. He used a computer-based dive log to record the data regarding each dive.
He reported lightheadedness about 1 h after surfacing from his final dive of the day. He was initially given intravenous (i.v.) fluids and supplemental oxygen via nasal cannula; the patient was unaware of the exact oxygen pressure used or the i.v. fluid rate or content. A dive medicine–trained physician’s assistant on the boat assessed him and reviewed his computer-based dive logs. His calculated residual nitrogen and his compliance with safety stops made DS unlikely. He did not have dizziness, joint pain, myalgias, rashes, balance or gait disturbance, weakness, paralysis, or any other clinical symptoms characteristic of DS, and given the high outdoor temperature with decreased fluid intake, his symptoms were attributed to dehydration. Supplemental oxygen was discontinued after 15 min and recompression using US Navy Table 6 was not performed since clinical DS was ruled out.
His symptoms improved after i.v. fluid resuscitation. The following morning, he awoke with diffuse mild to moderate abdominal cramping with nausea and spasms that were exacerbated by any oral intake; however, he was able to continue diving for an additional 3 days despite this. He mitigated his symptoms by limiting himself to small and infrequent meals. His symptoms continued to progress and increased to a 7–8/10 in intensity upon return from his trip.
During his trip, he described eating mostly chicken and pasta dishes and denied consumption of any raw or undercooked food, fish, or shellfish. He denied any recent use of alcohol. Those traveling with him did not experience similar symptoms. He denied fever, chills, night sweats, vomiting, and diarrhea. He was obese, with a body mass index (BMI) of 31, but was however without any other comorbidities or significant past medical history. He had never had any surgeries and prior to his recent clinic visit, he took no daily medications. He worked as an environmental consultant where he regularly scuba dived to obtain water samples. He endorsed rare social alcohol use and denied tobacco or illicit drug use.
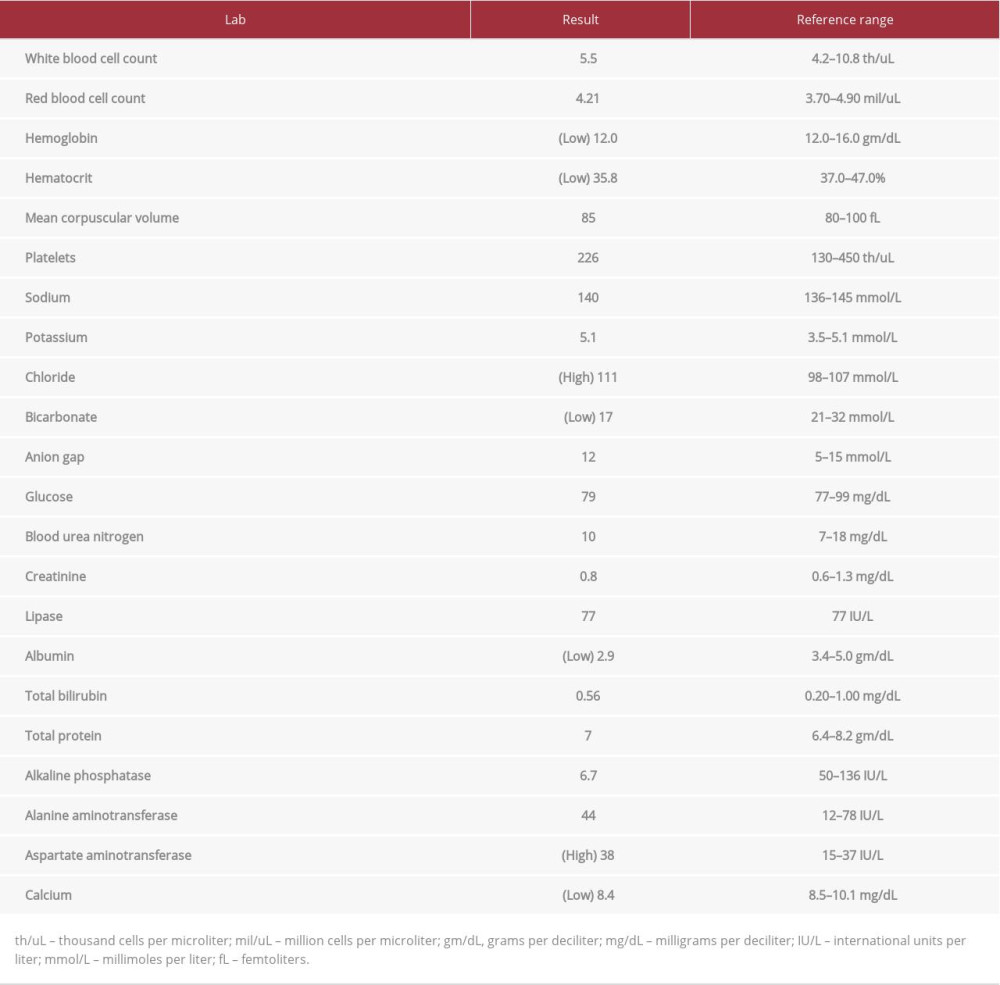
Upon return from his trip, he initially sought treatment at an outpatient clinic, where he was prescribed omeprazole and glucosamine and chondroitin for presumed gastritis without relief. He later presented to the ED 10 days after initial onset of gastrointestinal symptoms. His vital signs on presentation were all within normal limits. The physical examination was significant for a soft, yet diffusely tender and moderately distended abdomen with voluntary guarding but was otherwise unremarkable. The laboratory analysis was significant for mild normocytic anemia, non-anion gap metabolic acidosis, minimal elevation in alanine aminotransferase (ALT), and hypoalbuminemia. Interestingly, his lactic acid level was normal (Table 1).
A chest X-ray was unremarkable. An abdominal ultrasound showed a heterogeneous echotexture within the liver, with fatty infiltration medial to the left hepatic vein. A computed tomography (CT) scan of the abdomen and pelvis with i.v. contrast showed a low density within the portal vein, suggestive of a thrombus. A CT scan of the chest was not performed. A gastroenterologist was consulted and recommended a magnetic resonance angiogram (MRA) of the abdomen, which showed a gas-containing thrombus in the main portal vein and superior mesenteric vein (Figures 1, 2). A diagnosis of portal and mesenteric gas-containing venous thrombus was made. An outside facility with HBO capabilities was consulted; however, HBO therapy was not pursued because of timing since there was the onset and presence of thrombus. He was started on an i.v. heparin drip and transitioned to rivaroxaban, which was continued after hospital discharge.
He returned to his baseline level of functioning after about 1 month. Two months after discharge, a repeat CT of the abdomen and pelvis was performed, which showed a chronic thrombus of the portal, splenic, and superior mesenteric veins, with decreased vessel caliber and extensive venous collateral circulation throughout the abdomen despite compliance with rivaroxaban (Figures 3, 4). On review of his follow-up abdominal CT, questionable fatty replacement of the ileum was seen, which was concerning for Crohn disease. Given the risk of var-ices with chronic portal vein thrombus, and the association of Crohn disease with hypercoagulability, an esophagogastroduodenoscopy (EGD) and colonoscopy with biopsies were performed. These studies showed an incidental small gastric erosion and 3 small polyps, but no varices or tissue changes consistent with inflammatory bowel disease. He followed up with a hematologist who performed an extensive workup for genetic and autoimmune causes of hypercoagulability, which was unremarkable. The normocytic anemia previously seen in the ED had improved to a hemoglobin level of 13.5 on outpatient laboratory tests after hospital discharge. Unfortunately, a full anemia workup, including an iron panel, peripheral smear, and vitamin studies, was not performed and was believed to not be clinically significant, especially given a normal mean corpuscular volume, mean corpuscular hemoglobin concentration, and red blood cell distribution width. The fatty changes seen in his terminal ileum and heterogeneous fatty changes in the liver were also unable to be explained based on his further workup.
Discussion
This case demonstrates that silent nitrogen gas bubbles can predispose a patient to thrombosis, even in the absence of clinical decompression illness (DI). DI comprises 2 distinct pathologies: DS and air embolism [2]. DS is a clinical diagnosis that is made based on the presence of characteristic signs and symptoms [3]. It results from nitrogen bubbles that form within body compartments when the pressure of dissolved gasses exceeds local absolute pressure [3]. Divers inhale a mixture of nitrogen and oxygen, which occupy smaller volumes at increasing pressures during descent [2]. Unlike oxygen, the compressed nitrogen is not utilized by tissues [2]. Supersaturation occurs during ascent when pressures decrease faster than the rate of nitrogen gas washout from tissues [2]. It takes 12 to 24 h to fully clear excess nitrogen after a dive, which is why divers are advised to perform safety stops at depths greater than 18 m, and why repeat dives during the same day place divers at greater risk of DS [1,6].
An air embolism occurs secondary to inhalation of large volumes of air during diving [2]. This results in pulmonary baro-trauma, which pushes alveolar gas into the arterial circulation [2]. While the intra- and extravascular bubbles of DS are composed of nitrogen, those of an air embolism are composed of only air [2]. An arterial gas embolism typically causes neurological consequences as gas emboli enter the brain but it can uncommonly affect other organs within the body [2]. Given that gas was radiologically visualized within the venous system and not the arterial system of this patient, the portal and mesenteric vein thrombosis was not compatible with an arterial gas embolism but was related to venous nitrogen gas bubbles.
Symptoms of DS are secondary to nitrogen gas bubbles within tissues, namely the spinal cord, muscles, and joints [3]. They often include dizziness, myalgias, joint pain, rashes, and difficulty walking, making DS classically referred to as “the bends” [1,3]. Even in the absence of clinical DS, however, venous gas bubbles are common in diving and usually asymptomatic [2]. Our patient’s immediate symptoms on the boat were more likely secondary to dehydration, especially given that they resolved with i.v. fluids and did not require recompression treatment using US Navy Dive Table 6. Hemoconcentration due to plasma blood shifts is common in diving [2]. Increased temperature in warm tropical climates can further increase dehydration, which increases bubble formation [2]. While our patient did not have clinical evidence of DS upon surfacing, his dehydrated state likely further increased the formation of nitrogen bubbles.
Small venous gas bubbles independent of DS are more likely the cause of his portal and mesenteric venous thrombosis. Venous thrombosis secondary to diving is rarely reported, but a proposed mechanism is that bubbles within the vasculature may cause endothelial damage, induce a pro-inflammatory and pro-thrombotic state, and predispose a patient to clot formation [1,3]. Given the recent diving and lack of other predisposing factors for clotting, DS, coupled with dehydration, was the only reasonable explanation for portal vein and superior mesenteric vein thrombosis in our patient.
The etiology of portal venous thrombosis is often multifactorial, and includes hepatobiliary inflammation, malignancy, underlying inflammatory state, infection, cirrhosis, and hereditary or autoimmune causes of thrombophilia [7]. Potential etiologies of mesenteric venous thrombosis are similar [8]. Our patient was without stigmata of cirrhosis and had no coagulopathy or jaundice. He denied signs or symptoms of malignancy, and imaging was negative for any mass lesions. Pancreatitis is an uncommon cause of portal vein thrombus [9]; however, our patient had a normal lipase level and his abdominal pain was diffuse rather than epigastric. Inflammatory bowel disease was ruled out by EGD and colonoscopy. His serologic thrombophilia workup was unremarkable.
The superior mesenteric vein drains the small intestine, including the terminal ileum [10]. It is possible that the patient’s chronic mesenteric thrombus resulted in disrupted venous drainage and venous congestion, causing the questionable fatty changes seen on the CT scan around the terminal ileum. It is also possible that this was an incidental imaging finding without any true clinical significance. Workup including EGD and colonoscopy showed no bowel process, including inflammatory bowel disease or malignancy, that could have caused this imaging finding. It is therefore unlikely that this imaging finding was solely responsible for his portal or mesenteric vein thrombosis.
Portal venous gas can be related to other intra-abdominal pathology, including infection, bowel ischemia, peritonitis, bowel obstruction, sepsis, gastrointestinal cancers, and appendicitis [11]. Our patient developed gastrointestinal symptoms several hours after his initial symptoms of DS. Given that this occurred during travel and lasted for 1 week, his illness initially seemed most compatible with infection. His lack of vomiting, diarrhea, and fevers pointed away from an infectious source. Looking back at his description of symptoms, they appeared consistent with those seen in mesenteric thrombosis [12].
In a similar case, a deep sea diver in Japan presented with sudden abdominal pain after diving [12]. CT of the abdomen revealed gas in the portal, super mesenteric, inferior mesenteric, and femoral veins [12]. He urgently received HBO therapy; however, his pain worsened afterwards [12]. A repeat CT scan showed pneumatosis cystoides intestinalis, and he was urgently taken for exploratory laparotomy, which revealed a dark red and ischemic colon and mesentery [12]. He underwent resection, and pathology of the surgical specimen revealed venous thrombus [12]. This case of a Japanese diver mirrors the case of our patient who dived in the Bahamas in that the abdominal pain was secondary to mesenteric thrombosis. What is interesting is that our patient’s pain occurred many hours after diving, as opposed to immediately after in the case from Japan. In the case of our patient, it is unclear what his immediate scan would have shown, as it is equally unclear what the Japanese divers initial scan would have shown had he presented 1 week later. This begs the following question: Was HBO therapy actually harmful in the Japanese diver by further expanding the thrombus?
Other similar cases of venous thrombosis after scuba diving have been reported. In a case reported in 1984, a 27-year-old man developed periumbilical pain 12 h after diving [13]. He presented to the hospital 2 days later and was treated with recompression and i.v. fluids; however, his pain worsened [13]. He underwent exploratory laparotomy with bowel resection, and pathology of the resected specimen revealed thrombi within the mesenteric veins [13]. A serum thrombophilia workup was negative [13]. It is worth noting that while this patient was treated with recompression, his symptoms did not resolve, likely because they were related to the thrombus rather than venous gas alone.
A case reported in 2010 describes a 49-year-old male diver who reported severe abdominal pain and a pruritic rash immediately after surfacing [14]. Given the presence of a visible rash consistent with what is known as “skin bends”, a clinical diagnosis of DS was made [14]. He was recompressed in a hyperbaric chamber as per US Navy Table 5 [14]. His symptoms initially resolved; however, epigastric pain developed shortly thereafter [14]. An initial CT scan revealed minor portal and gastric venous bubbles; a subsequent scan 10 days later revealed portal venous thrombus [14]. Just like the patient in the present case, he was treated with anticoagulation, and his symptoms resolved [14]. A hypercoagulable workup and colonoscopy were negative, similar to the patient described in the present case [14].
The standard of care for DI is HBO, which encourages diffusion of nitrogen from gas bubbles into tissues [5]. HBO also enhances oxygen absorption, thereby increasing tissue perfusion [6]. What is not well known is the success of HBO when embolism is largely composed of a thrombus, and there is unfortunately no guideline-directed therapy for thrombosis related to diving. In recent literature, there are many applications for HBO aside from DS, including burns, carbon monoxide poisoning, retinal artery occlusion, and radiation injury; however, thrombosis is not one of them. [5]. Additionally, our patient presented 1 week after the initial insult, and HBO therapy for DS works best within a few hours after symptom onset [4]. For these reasons, HBO was not pursued.
This case was discussed with the vice president of the Diver’s Alert Network, an internationally recognized dive safety organization, who confirmed that the correct on site and hospital-based management was performed. The presence of light-headedness alone did not represent clinical DS, so there was no indication to perform recompression in the Bahamas. While thrombus is a known complication of decompression stress-related platelet aggregation and complement activation, recognized treatment is anticoagulation rather than HBO.
This case demonstrates that we must suspect a venous thrombus when approaching a patient with delayed onset gastrointestinal illness after diving. While treatment for DI is HBO, there is no guideline-directed treatment for thrombi related to asymptomatic gas bubbles common to divers. It is important to recognize that while a diver may not carry a clinical diagnosis of DS, these so-called “silent” bubbles can predispose to endothelial injury, venous stasis, and ultimately thrombosis. It is not known whether HBO is helpful in these situations, which poses a clinical question and area for further research.
Conclusions
DI comprises 2 clinical entities: DS and air embolism. DS is a clinical diagnosis caused by nitrogen gas bubbles that form within blood and tissues when an individual abruptly transitions from low- to high-pressure environments. Even in the absence of clinical DS, divers form asymptomatic bubbles. What is less well known is that these gas bubbles can predispose a patient to thrombosis when present in the venous system. Guideline-directed treatment of a bubble-induced thrombus that includes the utility of HBO and choice of anticoagulation unfortunately does not exist. This case demonstrates the importance of recognizing venous thrombosis in a patient presenting with gastrointestinal illness after diving, even when evidence of clinical DS is absent.
Figures
References:
1.. Merlin M, Ondeyka A, Marques-Batista A, Decompression illness in scuba divers: Emerg Med, 2009; 18(22); 48
2.. Vann RD, Butler FK, Mitchell S J, Moon R E, Decompression illness: Lancet, 2019; 377; 153-64
3.. Cooper JS, Hanson KC, Decompression sickness: National Center for Biotechnology Information, 2021, U.S. National Library of Medicine [serial online] [cited 2022 Feb 15]. Available from: URL: https://www.ncbi.nlm.nih.gov/books/NBK537264/?report=printable
4.. Antonelli C, Franchi F, Della Marta ME, Guiding principles in choosing a therapeutic table for DCI hyperbaric therapy: Minerva Anestesiol, 2009; 75; 151-61
5.. Ortega MA, Fraile-Martinez O, García-Montero C, A general overview on the hyperbaric oxygen therapy: Applications, mechanisms and translational opportunities: Medicina, 2021; 57(9); 864
6.. Moon RE, Decompression sickness – injuries; poisoning. Merck Manuals Professional Edition. Merck Manuals, 2021, Jun [cited 2022 Feb 15]. Available from: URL: https://www.merckmanuals.com/professional/injuries-poisoning/injury-during-diving-or-work-in-compressed-air/decompression-sickness
7.. Trebicka J, Strassburg CP, Etiology and complications of portal vein thrombosis: Viszeralmedizin, 2014; 30; 375-80
8.. Russell CE, Wadhera RK, Piazza G, Mesenteric venous thrombosis: Circulation, 2015; 131(18); 1599-603
9.. Gonzelez HJ, Sahay SJ, Samadi B, Splanchnic vein thrombosis in severe acute pancreatitis: a 2-year, single-institution experience: HPB (Oxford), 2011; 13(12); 860-64
10.. Broussard A, Wehrle CJ, Samra NS: Anatomy, abdomen and pelvis, superior mesenteric vein Aug, 2021, StatPearls [serial online]
11.. Hussain A, Mahmood H, El-Hasani S, Portal vein gas in emergency surgery: World J Emerg Surg, 2008; 3; 21
12.. Toyota S, Nagata S, Yoshino S, Mesenteric venous thrombosis as a rare complication of decompression sickness: Surg Case Rep, 2020; 6(1); 24
13.. Gertler S, Stein J, Simon T, Miyai K, Mesenteric venous thrombosis as sole complication of decompression sickness: Dig Dis Sci, 1984; 29; 91-95
14.. Righini M, Gueddi S, Maurel B, Coulange M, SCUBA diving and portal vein thrombosis: A case report: Clin J Sport Med, 2010; 20; 497-99
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133