09 April 2022: Articles 
Life-Threatening Cardiac Tamponade Secondary to COVID-19 Treated with Uniportal Video-Assisted Thoracoscopic Surgery: A Case Report
Unusual clinical course, Challenging differential diagnosis, Management of emergency care, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Rawand Abdulrahman Essa123ABCDEFG, Sirwan Khalid Ahmed123ABCDEFG*DOI: 10.12659/AJCR.935839
Am J Case Rep 2022; 23:e935839






Abstract
BACKGROUND: The COVID-19 outbreak emerged in December 2019 in Wuhan, China. COVID-19 is caused by the SARS-CoV-2 coronavirus and mostly affects the respiratory system but can also affect other organs, including the cardiovascular system. Furthermore, the most common cardiac complications include severe left ventricular dysfunction, acute myocardial injury, and arrhythmias. Life-threatening cardiac tamponade and large pericardial effusion are exceedingly rare complications in patients recovered from COVID-19. Previously, this condition was treated with pericardiocentesis, colchicine, and corticosteroids.
CASE REPORT: We present the case of a 54-year-old man who recovered from a SARS-CoV-2 infection 7 days before presentation and describe a complicated pericardial effusion with life-threatening cardiac tamponade. To the best of our knowledge, this is the first case of pericardial effusion with cardiac tamponade that was successfully treated with single port or uniportal video-assisted thoracoscopic surgery with an excellent outcome.
CONCLUSIONS: Life-threatening cardiac tamponade with pericardial effusion is an exceedingly rare complication in patients recovered from COVID-19. Generally, patients diagnosed with pericardial effusion undergo a pericardiocentesis procedure. Although there are multiple treatment options for draining pericardial effusion, the recurrence rate with surgical pericardial window formation is the lowest. However, our patient underwent surgery using a uniportal video-assisted thoracoscopic surgery with an excellent outcome.
Keywords: Cardiac Tamponade, COVID-19, Minimally Invasive Surgical Procedures, Pericardial Effusion, Thoracic Surgery, Video-Assisted, Video-Assisted Surgery, SARS-CoV-2, severe acute respiratory syndrome coronavirus 2, Pericardial Window Techniques, COVID-19, Humans, Male, Pericardiocentesis
Background
The current COVID-19 outbreak emerged in December 2019 in Wuhan, China. It is caused by the SARS-CoV-2 coronavirus and mostly affects the respiratory system; however, it can also affect other organs, including the cardiovascular system. Severe left ventricular dysfunction, acute myocardial injury, and arrhythmias are the most prevalent cardiac consequences [1].
The most commonly documented cardiovascular symptoms of COVID-19 include acute coronary syndrome, cardiac arrhythmias, thrombosis, and myocarditis. Although pericardial involvement has been reported in patients with COVID-19, the exact prevalence is unknown [2]. In a comprehensive evaluation of 34 individuals from 33 studies who presented with pericarditis, it was shown that 35% had cardiac tamponade, nearly half had myopericarditis, and 76% had pericardial effusion [3]. Conversely, reports of life-threatening cardiac tamponade and large pericardial effusion are rare [4]. Previously, this condition was treated with pericardiocentesis, colchicine, and corticosteroids.
Here we present the case of a 54-year-old man who recovered from SARS-CoV-2 infection and developed complicated pericardial effusion with cardiac tamponade, which was life-threatening. To the best of our knowledge, this is the first case of pericardial effusion with cardiac tamponade that was successfully treated using a single port or uniportal video-assisted thoracoscopic surgery (u-VATS) approach with an excellent outcome.
Case Report
A 54-year-old man presented with a severe cough of a 2-month duration. His general medical history was not significant. The patient had been diagnosed with COVID-19 65 days before presentation and recovered 7 days before arrival to hospital, as confirmed by real-time polymerase chain reaction (RTPCR) testing.
Regarding the treatment of COVID-19, the patient had received 1 mg ceftriaxone injection every 12 h for 6 days, vitamin D supplement for 10 days, and dextromethorphan 30 mg syrup every 8 h for 9 days, followed by paracetamol and oxygen therapy.
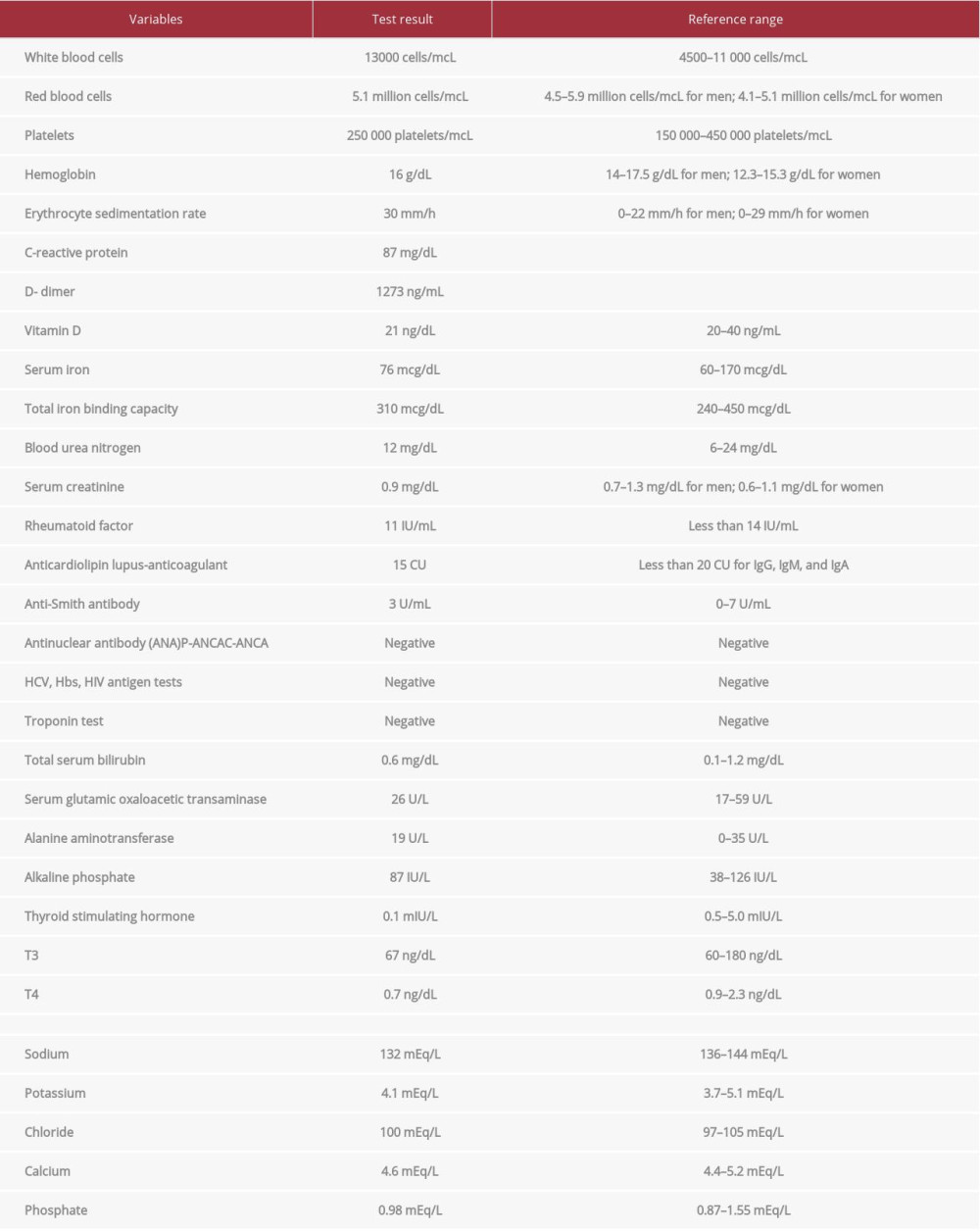
Upon arrival, the patient’s vital signs were blood pressure of 72/64 mmHg (hypotensive), heart rate of 132 beats/min (tachycardia), respiratory rate of 31 breaths/min (tachypnea), temperature of 37.4°C, and oxygen saturation of 82% at rest without oxygen therapy. Laboratory test results were within normal limits apart from an increased white blood cell count, C-reactive protein level, and D-dimer level (Table 1). The troponin test was negative. Radiologically, a computed tomography (CT) scan showed small ground-glass opacity in the right upper lobe. In addition, a 12-lead electrocardiogram showed sinus tachycardia. Moreover, transthoracic echocardiography was performed in the relaxation phase and revealed pericardial effusion with features of cardiac tamponade (dilated right atrium with systolic right atrium collapse, diastolic right ventricle collapse, dilated and plethoric inferior vena cava with failure of the inspiratory collapse of the inferior vena cava to more than 50%) (Video 1). The patient was free from any diseases, for example, connective tissue disorder, malignancy, endocarditis, myocarditis, and pericarditis. Finally, the patient was diagnosed with pericardial effusion, and cardiac tamponade secondary to COVID-19.
Subsequently, we planned to drain pericardial effusion with a wedge resection of the ground-glass-opacity through u-VATS. The patient was sent to undergo surgery under general anesthesia, and double-lumen endotracheal intubation was performed in the supine position. Then, the patient was positioned to the left lateral decubitus position and a 3-cm incision in the mid-axillary line in the fifth intercostal space was performed. The pericardium was full of fluid, and with a no. blade 15, we created a small pericardial window. An amount of 1200 cc of serosanguinous fluid was drained and tested negative for COVID-19 (Video 2). Then, we did a wedge resection in the right-upper lobe with staplers. A single chest drain was placed, and the incision was sutured in layers. Fluid cytology was negative for malignant cells, an acid-fast bacilli smear was negative, and no growth on fungal and bacterial cultures was reported.
In conclusion, all vital signs of the patient were normal apart from intermittent decreasing blood pressure. After 3 days in the Restorative Care Unit, the patient was discharged home. He experienced no recurrence of pericardial effusion.
Discussion
SARS-CoV-2 is a new virus that causes COVID-19. Early studies in Wuhan, China, showed that patients with COVID-19 frequently develop fever, upper respiratory symptoms, and pneumonia [5]. However, the pericardial association has been rarely reported [6,7]. People who have pre-existing cardiovascular disease are more prone to develop serious illness and have a higher death rate [8]. The precise mechanism behind SARS-CoV-2-induced acute myocardial injury is unclear [9]; however, it might be related to a cytokine storm [10] or myocardial ACE2 receptors [11]. COVID-19 causes numerous cardiovascular complications including arrhythmia, myocarditis, acute myocardial injury, cardiogenic shock, and thromboembolism [12,13]. However, cardiac tamponade has rarely been reported as a COVID-19 complication [12–14].
Here, we report a case of a patient who recovered from COVID-19 with large symptomatic pericardial effusion causing life-threatening cardiac tamponade secondary to COVID-19. Pericardial effusion was reported in 4.55% of 2738 patients with COVID-19 [15]. To date, only a few cases of pericardial effusion causing cardiac tamponade in patients with COVID-19 have been reported in the literature, and all of them were treated by pericardiocentesis, colchicine, pericardial window, aspirin, ibuprofen, steroids, and antiviral drugs [9,14,16–33]. Conversely, our case report demonstrates the first case treated by u-VATS. Although there are multiple treatment options for draining pericardial effusion, the recurrence rate of the surgical window option is reported to be the lowest [34,35]. Pericardial effusion has been reported in pericarditis due to tuberculous, malignant tumors, uremia, collagen-vascular disorders, trauma, post-¬myocardial infarction, irradiation, and unknown etiology of pericarditis [36]. Our patient was free from any diseases, such as connective tissue disorder, malignancy, endocarditis, myocarditis, and pericarditis. Little is known about the association between hemorrhagic pericardial effusion and viral infections; however, it has been linked to the Coxsackie virus [37].
Due to large pericardial effusion and symptoms of cardiac tamponade, this patient, who arrived with tachycardia and developed shortness of breath, underwent u-VATS. In this case, 1200 mL of pericardial fluid was drained, revealing a nonhemorrhagic pericardial effusion. His overall health improved after the u-VATS approach. Further studies are required to evaluate the benefit of u-VATS in patients with pericardial effusion. Because of our experience with single-port or u-VATS technology, we believe we can manage even the most challenging cases, such as this one. U-VATS should only be done by skilled surgeons.
Conclusions
Life-threatening cardiac tamponade with pericardial effusion is an exceedingly rare complication in patients who have recovered from COVID-19. Generally, patients diagnosed with pericardial effusion undergo a pericardiocentesis procedure. However, our patient underwent a surgical u-VATS approach with an excellent outcome.
References:
1.. Fried JA, Ramasubbu K, Bhatt R, The variety of cardiovascular presentations of COVID-19: Circulation, 2020; 141; 1930-36
2.. Johny D, Subramanyam K, Baikunje N, Hosmane GB, Cardiac tamponade and massive pleural effusion in a young COVID-19-positive adult: BMJ Case Rep, 2021; 14; e244518
3.. Diaz-Arocutipa C, Saucedo-Chinchay J, Imazio M, Pericarditis in patients with COVID-19: A systematic review: J Cardiovasc Med, 2021; 22; 693-700
4.. Hua A, O’Gallagher K, Sado D, Byrne J, Life-threatening cardiac tamponade complicating myo-pericarditis in COVID-19: Eur Heart J, 2020; 41(22); 2130
5.. Guan W, Ni Z, Hu Y, Clinical characteristics of coronavirus disease 2019 in China: N Engl J Med, 2020; 382; 1708-20
6.. Inciardi RM, Lupi L, Zaccone G, Cardiac involvement in a patient with coronavirus disease 2019 (COVID-19): JAMA Cardiol, 2020; 5; 819-24
7.. Salehi S, Abedi A, Balakrishnan S, Gholamrezanezhad A, Coronavirus disease 2019 (COVID-19): A systematic review of imaging findings in 919 patients: Am J Roentgenol, 2020; 215; 87-93
8.. Zheng YY, Ma YT, Zhang JY, Xie X, COVID-19 and the cardiovascular system: Nat Rev Cardiol, 2020; 17; 259-60
9.. Purohit R, Kanwal A, Pandit A, Acute myopericarditis with pericardial effusion and cardiac tamponade in a patient with COVID-19: Am J Case Rep, 2020; 21; e925554
10.. Wong CK, Lam CWK, Wu AKL, Plasma inflammatory cytokines and chemokines in severe acute respiratory syndrome: Clin Exp Immunol, 2004; 136; 95-103
11.. Turner AJ, Hiscox JA, Hooper NM, ACE2: From vasopeptidase to SARS virus receptor: Trends Pharmacol Sci, 2004; 25; 291-94
12.. Driggin E, Madhavan MV, Bikdeli B, Cardiovascular considerations for patients, health care workers, and health systems during the COVID-19 pandemic: J Am Coll Cardiol, 2020; 75; 2352-71
13.. Vetta F, Vetta G, Marinaccio L, Coronavirus disease 2019 (COVID-19) and cardiovascular disease: A vicious circle: J Cardiol Cardiovasc Res, 2020; 1; 1-12
14.. Cairns L, El Khaleq YA, Storrar W, Scheuermann-Freestone M, COVID-19 myopericarditis with cardiac tamponade in the absence of respiratory symptoms: A case report: J Med Case Rep, 2021; 15; 1-4
15.. Bao C, Liu X, Zhang H, Li Y, Liu J, Coronavirus disease 2019 (COVID-19) CT findings: A systematic review and meta-analysis: J Am Coll Radiol, 2020; 17; 701-9
16.. Asif T, Kassab K, Iskander F, Alyousef T, Acute pericarditis and cardiac tamponade in a patient with COVID-19: A therapeutic challenge: Eur J Case Rep Intern Med, 2020; 7; 001701
17.. Dabbagh MF, Aurora L, D’Souza P, Cardiac tamponade secondary to COVID-19: Case Rep, 2020; 2; 1326-30
18.. Dalen H, Holte E, Guldal AU, Acute perimyocarditis with cardiac tamponade in COVID-19 infection without respiratory disease: BMJ Case Rep, 2020; 13; e236218
19.. Derveni V, Kaniaris E, Toumpanakis D, Acute life-threatening cardiac tamponade in a mechanically ventilated patient with COVID-19 pneumonia: IDCases, 2020; 21; e00898
20.. Farina A, Uccello G, Spreafico M, SARS-CoV-2 detection in the pericardial fluid of a patient with cardiac tamponade: Eur J Intern Med, 2020; 76; 100
21.. García-Cruz E, Manzur-Sandoval D, Lazcano-Díaz EA, Soria-Castro E, Jiménez-Becerra S, Cardiac tamponade in a patient with myocardial infarction and COVID-19: Electron microscopy: Case Rep, 2020; 2; 2021-23
22.. Hakmi H, Sohail A, Brathwaite C, Cardiac tamponade in COVID-19 patients: Management and outcomes: J Card Surg, 2020; 35; 3183-90
23.. Heidari A, Hashemi SE, Hemorrhagic pericardial effusion leading to cardiac tamponade, as presenting feature of COVID-19 in a young man: A case report: Acta Biomed, 2020; 91; e2020146
24.. Kermani-Alghoraishi M, Pouramini A, Kafi F, Khosravi A, Coronavirus disease 2019 (COVID-19) and severe pericardial effusion: From pathogenesis to management: A case report based systematic review: Curr Probl Cardiol, 2021; 74; 100933
25.. Khatri A, Wallach F, Coronavirus disease 2019 (Covid-19) presenting as purulent fulminant myopericarditis and cardiac tamponade: A case report and literature review: Hear Lung, 2020; 49; 858-63
26.. Parsova KE, Pay L, Oflu Y, Hacıyev R, Çinier G, A rare presentation of a patient with COVID-19: cardiac tamponade: Turk Kardiyol Dern Ars, 2020; 48; 703-6
27.. Reddy A, Nethercott S, Duehmke R, Dry’pericarditis with rapid progression to tamponade as a feature of COVID-19: Eur Med J, 2021; 10; emj/2000244
28.. Robak O, Dudek M, Ladny JR, Cardiac tamponade as a cause of COVID-19: Cardiol J, 2020; 27; 900-1
29.. Ruiz-Rodríguez JC, Chiscano-Camon L, Ruiz D, Cardiac tamponade as a cause of cardiac arrest in severe COVID-19 pneumonia: Resuscitation, 2020; 155; 1-2
30.. Sauer F, Dagrenat C, Couppie P, Pericardial effusion in patients with COVID-19: Case series: Eur Hear J Case Rep, 2020; 4; 1
31.. Singh R, Fuentes S, Ellison H, A case of hemorrhagic cardiac tamponade in a patient with COVID-19 infection: CASE (Phila), 2020; 4; 316-19
32.. Tiwary T, Baiswar S, Jinnur P, A rare case of COVID-19 myocarditis with cardiac tamponade in a young diabetic adult with renal failure: Cureus, 2020; 12; e11632
33.. Walker C, Peyko V, Farrell C, Pericardial effusion and cardiac tamponade requiring pericardial window in an otherwise healthy 30-year-old patient with COVID-19: A case report: J Med Case Rep, 2020; 14; 158
34.. O’Brien PKH, Kucharczuk JC, Marshall MB, Comparative study of subxiphoid versus video-thoracoscopic pericardial “window”: Ann Thorac Surg, 2005; 80; 2013-19
35.. Neragi-Miandoab S, Linden PA, Ducko CT, VATS pericardiotomy for patients with known malignancy and pericardial effusion: survival and prognosis of positive cytology and metastatic involvement of the pericardium: A case control study: Int J Surg, 2008; 6; 110-14
36.. Braunwald E, Fauci AS, Kasper DL: Harrison’s principles of internal medicine, 2001, McGraw Hill
37.. Hamasaki A, Uchida T, Yamashita A, Cardiac tamponade caused by acute coxsackievirus infection related pericarditis complicated by aortic stenosis in a hemodialysis patient: A case report: Surg Case Rep, 2018; 4; 141
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133