26 April 2022: Articles 
A Case of Synthetic Cannabinoid (K2)-Induced Posterior Reversible Encephalopathy Syndrome (PRES)
Unusual clinical course, Challenging differential diagnosis
Haider Ghazanfar1ABCDEF*, Aruna MuthumanickamDOI: 10.12659/AJCR.936209
Am J Case Rep 2022; 23:e936209






Abstract
BACKGROUND: K2 is an artificially synthesized cannabinoid (SCB), manufactured as a non-consumption herbal incense but increasingly misused as a recreational drug. Posterior reversible encephalopathy syndrome (PRES) is a rare clinical and radiological entity characterized by brain edema, often in the setting of acute hypertension. Cases of PRES caused by recreational drug use have been reported in the literature.
CASE REPORT: We report an unusual case of PRES after consumption of K2 in a 24-year-old healthy woman who presented with episodic agitation and altered mental status. Magnetic resonance imaging showed nonspecific subtle high T2/FLAIR (fluid-attenuated inversion recovery) signal intensities in the region of the posterior parietal and occipital cortices. Her extensive drug screen report was positive for K2. Her mental status improved over the course of 3 weeks and she had returned to her baseline at 3-month follow-up.
CONCLUSIONS: Our case highlights the importance of having a high clinical suspicion in patients presenting with altered mental status and a history of recreational drug use. K2 is not detected by routine urine drug testing, so a high level of clinical suspicion is required to request an extensive drug screen. It is important for the physician to counsel active synthetic cannabinoid users regarding these rare complications.
Keywords: Cannabinoids, Posterior Leukoencephalopathy Syndrome, Recreational Drug Use, Toxicology, Adult, Brain Edema, Female, Humans, Hypertension, Magnetic Resonance Imaging, young adult
Background
K2, also colloquially called ‘Spice’, ‘Pot Pourri’, or ‘Mojo’, is the term for artificially engineered cannabinoids misused as psychedelic agents [1]. In 2016, among a cohort of college students, it was found that the weighted lifetime prevalence of K2 use at college entry was 7.6% [2]. Synthetic cannabinoids (SCBs) are increasingly gaining popularity as they are cheaper and are not detected by most standard drug screens [3]; therefore, its use is more common among low income individuals and high school and college students. K2 can be smoked using joints, pipes, and E-Cigarettes, or it can be brewed as a tea. While SCBs are often similar in their mechanism of action to natural marijuana, in vitro and in vivo studies have found that K2 functions as full agonists at cannabinoid receptor 1 (CBR1) and cannabinoid receptor 2 (CBR2), unlike (delta)9-THC, which is only a partial agonistic agent [4]. This has been postulated as the cause of the greater toxicity of K2 as compared to natural marijuana. We present the case of a young, healthy patient with no known comorbidities who developed posterior reversible encephalopathy syndrome (PRES) following ingestion of K2.
Case Report
Our patient was a 24-year-old woman brought by emergency medical service to the Emergency Department after an episode of abnormal behavior at home. Her mother reported that at around 1: 00 a.m., she found her daughter awake crying, clenching her teeth, and screaming incomprehensibly. She stated that her daughter had been experiencing such episodes intermittently over the past 3 days, along with vague, nonspecific, intermittent headaches. Her past medical and surgical histories were unremarkable. There was no significant family history of neurologic, psychiatric, or autoimmune conditions.
She was evaluated in the Emergency Department and was noted to have episodic agitation, with bouts of crying followed by blank staring. The patient had a pulse rate of 98 beats per minute, a temperature of 37.1°C, respiratory rate of 18 breaths per minute, and blood pressure of 114/76, and was saturating 98% on room air. On physical examination, the patient appeared anxious and drowsy. She was only oriented to place but could follow simple commands. She had bilateral vesicular breathing on lung auscultation. Cardiac examination revealed normal S1 and S2 heart sound. Abdominal examination and neurological examination were unremarkable.
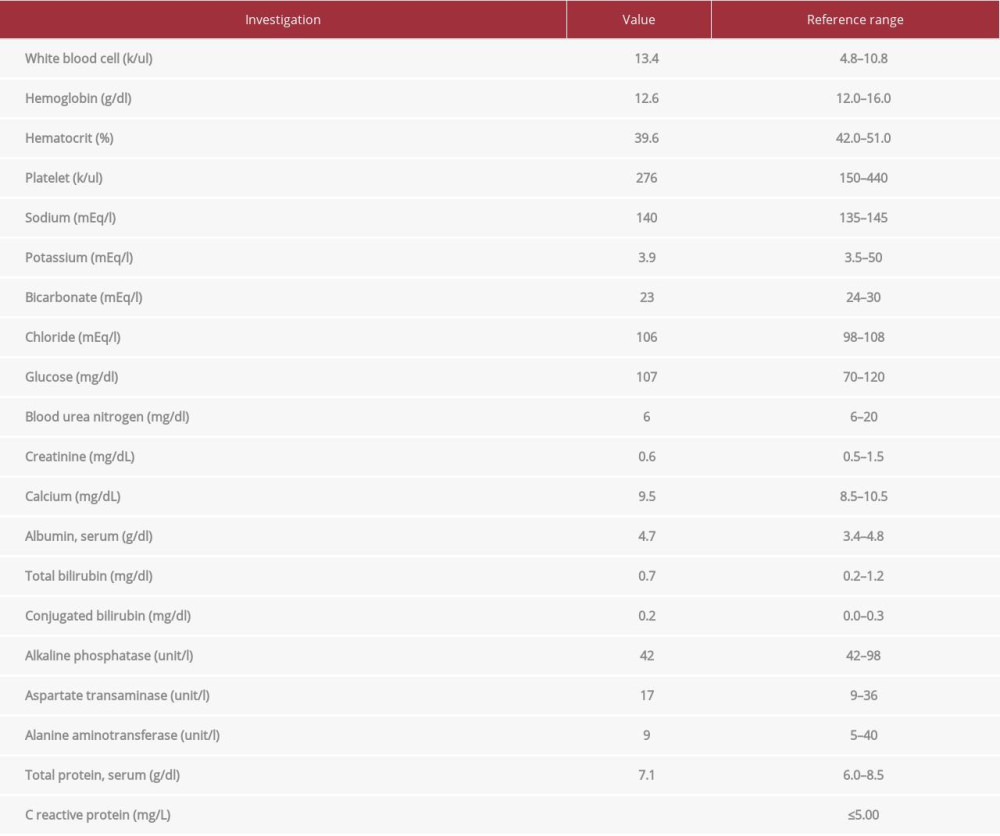
An initial computed tomography (CT) head was negative for any acute pathology, and a chest X-ray and a CT of the abdomen and pelvis were within normal limits. The complete cell count, electrolytes, creatinine, liver function test, creatine kinase, and ammonia blood test results were normal. Urinalysis revealed positive nitrites, leukocyte esterase, and bacteria. Her urine drug screen was positive for cannabinoids. Her initial investigation results are shown in Table 1.
She was started on ceftriaxone for possible urinary tract infection and was admitted to the inpatient service for further evaluation. On day 4 of hospitalization, she became increasingly agitated and was found to be at risk of physical harm to herself and others. Haloperidol was given as needed for delirium and agitation.
She developed 1 episode of partial complex seizures with postictal confusion. Broad-spectrum antibiotics were initiated empirically for suspected meningoencephalitis. A lumbar puncture was done, and cerebrospinal fluid (CSF) testing revealed 5 white blood cells, high glucose, normal proteins, negative bacterial antigens, cryptococcal antigen testing, Herpes simplex virus (HSV) PCR (polymerase chain reaction), and Cytomegalovirus (CMV) CSF PCR. Results of a work-up for other infectious diseases were negative, including testing for human immunodeficiency virus (HIV), hepatitis B, lyme disease, syphilis, and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) PCR. Blood and CSF cultures were negative, and antibiotics were discontinued. Antinuclear antibodies (ANA) were positive (1: 80) in a homogeneous nuclear pattern. Subsequent subserologies were negative, and complement levels were normal.
She underwent an electroencephalogram, which was nonspecific and demonstrated bilateral slowing and disorganization of background rhythms suggestive of diffuse encephalopathy. MRI did not reveal any hemorrhage, masses, or recent infarcts. High T2/FLAIR signal intensities were seen in the regions of the parietal cortices, suggestive of PRES (Figure 1).
Given the MRI findings above, the acute onset of neurocognitive symptoms including headaches, seizures, confusion, nausea, and vomiting, and history of cannabinoid intake, without any clinical evidence of an infectious or autoimmune process, the diagnosis of posterior reversible encephalopathy syndrome was made. She was continued on levetiracetam for seizure prophylaxis and olanzapine as needed for agitation. Her extensive drug screen report was positive for K2. Her clinical condition improved after 3 weeks of inpatient hospitalization, and she was discharged home with outpatient neurology follow-up.
Three months after discharge, she reported feeling well and was getting ready to return to work. She also stated that she was no longer using cannabis and K2.
Discussion
Most systemic effects of K2 ingestion are the result of its full agonist effect on CB1R and CB2R [5]. CB1Rs are abundant in many regions of the brain, while CB2Rs are concentrated in the hippocampus and ventral tegmental area, and regulate the dopaminergic pathway [6,7]. One of the postulated mechanisms of PRES caused by K2 consumption is activation of CB receptors, which leads to acute inhibition of synaptic neurotransmitter release in the brain [8]. Patients with K2 toxicity can present with vomiting, headache, chest pain, tachycardia, inability to speak, memory loss, numbness, seizures, stroke, hallucinations, paranoia, anxiety attacks, aggressive behavior, and suicidal ideation [7]. In severe cases, K2 intoxication can lead to cardiac arrest [9] and acute liver failure [10]. Our patient experienced episodic agitation, altered mental status, and partial complex seizures with postictal confusion.
PRES is a clinico-radiologic disorder characterized by symptoms of headaches, seizures, visual disturbances, and altered mental status, with the finding of white matter vasogenic edema of the posterior occipital and parietal lobes. PRES is often triggered by elevated blood pressure and the associated cerebral vascular damage and interstitial extravasation. Blood pressure plays a pivotal role in the pathogenesis of toxin-mediated PRES. A possible mechanism is the cerebral vasoconstriction causing infarcts in the brain, failure of cerebral autoregulation with edema, and endothelial damage with blood-brain barrier disruption. It is believed that the rapid rise in blood pressure is more important than the blood pressure itself [11,12]. Our case demonstrates that PRES syndrome can occur in patients without hypertension; therefore, the possibility of PRES should not be dismissed in normotensive patients.
PRES can also manifest in patients who are normotensive at presentation. Immunosuppressive or immunomodulatory therapies have also been in implicated in the causation of PRES. In a large case series, it was shown that half of the patients with PRES had a history of immunosuppressive medication intake [13]. There is no direct connection between the serum levels of immunosuppressive medication and the development of PRES [14]. Few cases of PRES are be related to consumption of alcohol [15], cocaine [16], mephedrone [17], kratom [18], and K2 [3] have been reported in the literature. We report the second case of PRES caused by consumption of K2.
Radiological abnormalities of PRES are often apparent on CT but are best described by MRI [19,20]. The typical findings of PRES include bilateral areas of white matter edema in the posterior cerebral hemispheres, especially the parietal-occipital regions. The presence of vasogenic edema has been linked with worse clinical outcomes but not with the severity of presentation [21]. Our patient had nonspecific subtle high T2/FLAIR signal intensities in the regions of the posterior parietal and occipital cortices.
PRES should be promptly recognized, as it is reversible with appropriate management. There are no clinical studies on the management of PRES, and most of the current recommendations are based on observational data and focus on blood pressure control. In a patient presenting with a hypertensive emergency, the initial goal should be to lower diastolic blood pressure to 100–105 mmHg within 2–6 h, with maximum initial fall not exceeding 25% [22]. For patients with hypertension without end-organ damage, blood pressure-lowering guidelines are the same as described for hypertensive emergencies. Aggressive blood pressure-lowering should be avoided because it can lead to complications. Seizures can occur in PRES, and antiepileptic treatment has been used in selected patients [23]. Immunosuppressive therapy should be decreased or discontinued in patients with PRES [24]. Steroids have been used in the treatment of PRES, but they are not routinely recommended due to the associated risk of hypertension, which can worsen PRES [25]. Supportive care is the standard of care for patients presenting with PRES. Our patient clinically improved with supportive care.
Delayed diagnosis and treatment can lead to irreversible neurological deficit and death [26]. It is vital to have a low threshold for suspecting PRES based on clinical presentation, as neuro-imaging lags behind the clinical progression. In hypertensionor toxin/drug-associated PRES, the effective therapy is the withdrawal of the drug, control of blood pressure, and antiseizure medication. In most cases, the syndrome is fully reversible within days to weeks [27]. According to a retrospective review, recurrence of PRES was seen in 4% of patients [28]. On rare occasions, some patients develop epilepsy after recovering from PRES [29]. Our patient did not develop epilepsy after recovering from PRES.
Conclusions
Our case highlights the importance of having a high clinical suspicion in patients presenting with altered mental status and a history of recreational drug use. K2 is not detected by routine urine drug testing, so a high level of clinical suspicion is required to request an extensive drug screen. It is important for the physician to counsel active synthetic cannabinoid users regarding these rare complications.
References:
1.. Gunderson EW, Haughey HM, Ait-Daoud N, “Spice” and “K2” herbal highs: A case series and systematic review of the clinical effects and bio-psychosocial implications of synthetic cannabinoid use in humans: Am J Addict, 2012; 21(4); 320-26
2.. Egan KL, Suerken CK, Reboussin BA, K2 and Spice use among a cohort of college students in southeast region of the USA: Am J Drug Alcohol Abuse, 2015; 41(4); 317-22
3.. Parajuli P, Regmi MR, Lara-Garcia OE, Man vs. man-made marijuana: A case of drug-induced posterior reversible encephalopathy syndrome (PRES) due to K2, a synthetic cannabinoid (SCB): J Community Hosp Intern Med Perspect, 2020; 10(4); 361-64
4.. Fantegrossi WE, Moran JH, Radominska-Pandya A, Prather PL, Distinct pharmacology and metabolism of K2 synthetic cannabinoids compared to Δ(9)-THC: Mechanism underlying greater toxicity?: Life Sci, 2014; 97(1); 45-54
5.. Aung MM, Griffin G, Huffman JW, Influence of the N-1 alkyl chain length of cannabimimetic indoles upon CB(1) and CB(2) receptor binding: Drug Alcohol Depend, 2000; 60(2); 133-40
6.. Zou S, Kumar U, Cannabinoid receptors and the endocannabinoid system: Signaling and function in the central nervous system: Int J Mol Sci, 2018; 19(3); 833
7.. Mills B, Yepes A, Nugent K, Synthetic cannabinoids: Am J Med Sci, 2015; 350(1); 59-62
8.. Walsh KB, Andersen HK, Molecular pharmacology of synthetic cannabinoids: Delineating CB1 receptor-mediated cell signaling: Int J Mol Sci, 2020; 21(17); 6115
9.. Ibrahim S, Al-Saffar F, Wannenburg T, A unique case of cardiac arrest following K2 abuse: Case Rep Cardiol, 2014; 2014; 120607
10.. Sheikh IA, Lukšič M, Ferstenberg R, Culpepper-Morgan JA, Spice/K2 synthetic marijuana-induced toxic hepatitis treated with N-acetylcysteine: Am J Case Rep, 2014; 15; 584-88
11.. Gao B, Lyu C, Lerner A, McKinney AM, Controversy of posterior reversible encephalopathy syndrome: What have we learnt in the last 20 years?: J Neurol Neurosurg Psychiatry, 2018; 89(1); 14-20
12.. Rabinstein AA, Mandrekar J, Merrell R, Blood pressure fluctuations in posterior reversible encephalopathy syndrome: J Stroke Cerebrovasc Dis, 2012; 21(4); 254-58
13.. Fugate JE, Claassen DO, Cloft HJ, Posterior reversible encephalopathy syndrome: Associated clinical and radiologic findings: Mayo Clin Proc, 2010; 85(5); 427-32
14.. Covarrubias DJ, Luetmer PH, Campeau NG, Posterior reversible encephalopathy syndrome: Prognostic utility of quantitative diffusion-weighted MR images: Am J Neuroradiol, 2002; 23(6); 1038-48
15.. Bhagavati S, Choi J, Atypical cases of posterior reversible encephalopathy syndrome. Clinical and MRI features: Cerebrovasc Dis, 2008; 26(5); 564-66
16.. Bazuaye-Ekwuyasi E, Chow RD, Schmalzle S, An atypical subacute presentation of posterior reversible encephalopathy syndrome: J Community Hosp Intern Med Perspect, 2017; 7(4); 269-74
17.. Omer TA, Doherty C, Posterior reversible encephalopathy syndrome (PRES) complicating the ‘legal high’ Mephedrone: BMJ Case Rep, 2011; 2011; bcr0220113904
18.. Castillo A, Payne JD, Nugent K, Posterior reversible leukoencephalopathy syndrome after kratom ingestion: Proc (Bayl Univ Med Cent), 2017; 30(3); 355-57
19.. Hugonnet E, Da Ines D, Boby H, Posterior reversible encephalopathy syndrome (PRES): Features on CT and MR imaging: Diagn Interv Imaging, 2013; 94(1); 45-52
20.. Bartynski WS, Boardman JF, Distinct imaging patterns and lesion distribution in posterior reversible encephalopathy syndrome: Am J Neuroradiol, 2007; 28(7); 1320-27
21.. Schweitzer AD, Parikh NS, Askin G, Imaging characteristics associated with clinical outcomes in posterior reversible encephalopathy syndrome: Neuroradiology, 2017; 59(4); 379-86
22.. Vaughan CJ, Delanty N, Hypertensive emergencies: Lancet, 2000; 356(9227); 411-17
23.. Stott VL, Hurrell MA, Anderson TJ, Reversible posterior leukoencephalopathy syndrome: A misnomer reviewed: Intern Med J, 2005; 35(2); 83-90
24.. Hayes D, Adler B, Turner TL, Mansour HM, Alternative tacrolimus and sirolimus regimen associated with rapid resolution of posterior reversible encephalopathy syndrome after lung transplantation: Pediatr Neurol, 2014; 50; 272
25.. Hunter RW, Ivy JR, Bailey MA, Glucocorticoids and renal Na+ transport: Implications for hypertension and salt sensitivity: J Physiol, 2014; 592(8); 1731-44
26.. Fugate JE, Rabinstein AA, Posterior reversible encephalopathy syndrome: Clinical and radiological manifestations, pathophysiology, and outstanding questions: Lancet Neurol, 2015; 14(9); 914-25
27.. Lee VH, Wijdicks EF, Manno EM, Rabinstein AA, Clinical spectrum of reversible posterior leukoencephalopathy syndrome: Arch Neurol, 2008; 65(2); 205-10
28.. Sweany JM, Bartynski WS, Boardman JF, “Recurrent” posterior reversible encephalopathy syndrome: Report of 3 cases – PRES can strike twice!: J Comput Assist Tomogr, 2007; 31; 148-56
29.. Heo K, Cho KH, Lee MK, Development of epilepsy after posterior reversible encephalopathy syndrome: Seizure, 2016; 34; 90-94
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133