25 July 2022: Articles 
Isolated Anemia in a 69-Year-Old Man with HIV-1: Features of Pure Red Cell Aplasia Mediated by Chronic Parvovirus-B19 Infection
Rare disease
Jason Wylde1ABCDEF, Massimo A. Berneri1ABCDEF, Jacques A.J. Malherbe12BCDEF, Sue Davel12ABCDEF*DOI: 10.12659/AJCR.936445
Am J Case Rep 2022; 23:e936445






Abstract
BACKGROUND: Pure red cell aplasia (PRCA) is an uncommon syndrome characterized by ineffective erythropoiesis and severe anemia. Among immunodeficient patients, including those with human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS), persistent parvovirus-B19 can cause PRCA. We report a rare case of an Australian man with parvovirus-B19 mediated PRCA secondary to a new diagnosis of HIV-1/AIDS. The case highlights the importance of early treatment initiation with anti-retroviral drugs and pooled immunoglobulins to enable marrow recovery and long-term disease remission.
CASE REPORT: A 64-year-old man residing in rural Indonesia presented with severe anemia. Apart from 8 kg of unintentional weight loss, he denied any occult bleeding, diatheses, or constitutional symptoms. His bloodwork revealed a normocytic, normochromic anemia (Hb 81 g/L) with profound reticulocytopenia (9.5×10⁹/L). Parvovirus-B19 serology and polymerase chain reaction testing confirmed active viremia. Lymphopenia and an undetectable CD4 T-lymphocyte count (<1%) were also noted; HIV-1 was subsequently diagnosed. Bone marrow sampling later confirmed features consistent with parvovirus-B19-driven PRCA secondary to HIV-1/AIDS. The patient received 1 g/kg intravenous immunoglobulin for two days and initiated anti-retroviral HIV therapy. Rapid reticulocytosis with slow incrementation of his hemoglobin were observed over one month. At three years following his diagnosis, he remains in remission.
CONCLUSIONS: Severe, isolated anemia in immunodeficient patients, particularly those with HIV-1/AIDS, should prompt consideration of parvovirus-B19-mediated PRCA. Depletion of CD4-T-lymphocyte populations enables the establishment of parvovirus-B19 reservoirs within erythroid progenitors, thereby hampering physiological erythropoiesis. Long-term remission can be achieved with the rapid institution of intravenous immunoglobulin and anti-retroviral HIV therapies.
Keywords: Anemia, HIV, Parvovirus, Red-Cell Aplasia, Pure, Acquired Immunodeficiency Syndrome, Aged, Australia, Graft vs Host Disease, HIV Infections, HIV-1, Humans, Immunoglobulins, Intravenous, Male, Middle Aged, Parvoviridae Infections, Parvovirus B19, Human
Background
Anemia is a common issue worldwide, with iron-deficiency anemia being recognized as the most prevalent in Australia [1]. Other common causes of anemia include renal failure, anemia due to chronic disease, hematological neoplasms (eg, myelodysplastic syndromes, lymphomas, leukaemias), solid tumor malignancies, gastrointestinal pathology (ie, malabsorption, bleeding), pregnancy, endocrine disorders, hemolysis, or hemoglobinopathies [1]. In addition to routine clinical assessments and examination, the initial identification and diagnosis of anemia is based on evaluation of the complete blood count and blood film. Further investigations and treatments are subsequently guided by these findings to isolate an underlying etiology.
In the absence of a clear cause, particularly when the anemia is severe and associated with reticulocytopenia, a primary marrow abnormality should be considered. Pure red cell aplasia (PRCA) is an uncommon but well-described syndrome characterized by marked reticulocytopenia and impaired erythropoiesis, resulting in a chronic normocytic and normochromic anemia [1,2]. Several conditions have been implicated to cause PRCA, including lymphoproliferative disorders, solid organ tumors (ie, thymomas), autoimmune diseases (eg, systemic lupus erythematosus), congenital predispositions (ie, Diamond-Blackfan anemia), and a myriad of viral infections [2–9]
The persistence of parvovirus-B19-mediated PRCA is extremely rare and is diagnosed serologically or through the molecular detection of parvovirus-B19 DNA in the peripheral blood or bone marrow [11,12]. A bone marrow biopsy supplements the diagnostic process and shows characteristic giant pronormo-blasts with viral inclusions, absent erythroblasts and erythroid aplasia or hypoplasia in parvovirus-B19-mediated PRCA [11,12]. Although the seroprevalence for parvovirus-B19 in Australia is high [13], severe immunocompromise (eg, HIV/AIDS) is a prerequisite for chronic infection and persistence of virally-mediated PRCA. In patients with chronic human immunodeficiency virus (HIV) infections and acquired immunodeficiency syndrome (AIDS), PRCA driven by chronic parvovirus-B19 has been previously described and affects up to 4.5% of patients [9,14–18]. HIV treatment guidelines both in Australia [19] and abroad [20] require the immediate initiation of highly active anti-retroviral therapy (HAART) following the detection of HIV.
Effective therapies include drug combinations from at least two different drug classes and >95% lifelong adherence to therapy [19,20]. In PRCA caused by chronic parvovirus-B19 viraemia in HIV patients, the rapid institution of HAART therapy rekindles the immune response to sequester parvovirus-B19 particles and facilitates erythroid recovery in the marrow [17,18]. Intravenous immunoglobulin (IVIG) and transfusion support are also regarded as adjunctive therapeutic strategies used in combination with HAART to manage severe and persistent parvovirus-B19-mediated PRCA [14–18].
We report the rare case of an elderly man who presented with severe anemia, requiring multiple transfusions, which arose from a chronic, parvovirus-B19-mediated PRCA on a background of a new HIV-1 diagnosis and profound immunodeficiency. We discuss the diagnostic and treatment challenges of a severe, chronic anemia despite transfusion support, particularly in the setting of persistent immunodeficiency and chronic parvovirus-B19-mediated PRCA. The case highlights that the early recognition of a chronic infective etiology, particularly parvovirus-B19, in the context of an unexplained and persistent anemia, is paramount to initiating early treatment with both IVIG and HAART to maintain long-term remission.
Case Report
A 64-year-old man presented to our hospital for investigation and management of severe and chronic anemia that required repeated blood transfusions. The patient had resided in rural Indonesia for the past 15 years. Three months prior to his admission, he had presented to a local Indonesian hospital with syncope and severe anemia (hemoglobin [Hb] 44 g/L). Extensive esophago-gastro-duodenoscopy and colonos-copy investigations were performed, and a gastrointestinal source of bleeding was excluded. He was transfused with six units of packed red blood cells and discharged. He re-presented one week later in Indonesia with presyncope and recurrent severe anemia (Hb 41 g/L). He was transfused with a further four units of packed red blood cells and returned to Australia for ongoing management of his anemia.
On admission to our unit, he had postural dizziness, nausea, and diarrhea. He did not have hematemesis, melena, or hematochezia. He reported 8 kg of unintentional weight loss and increasing fatigue and lethargy in the preceding six months. He denied any acute bleeding diatheses, abnormal bruising, rashes, fevers, drenching nights sweats, or constitutional symptoms. He had not traveled outside of Indonesia within the last year and denied any recent insect or mosquito bites. His diet was varied and included meat products. He denied any previous history of anemia or malignancy. He was a current smoker with a total of 50 pack years and consumed ~40.0 g of alcohol socially per week. He did not engage in any recreational or illicit drug use and resided at home with his wife, with whom he had a monogamous relationship for eight years. Prior to this, he had unprotected coitus with multiple sex workers. His past medical history included ischemic heart disease with previous coronary artery bypass grafting surgery, hypertension, hyper-cholesterolemia, gastro-esophageal reflux disease, an inguinal hernia repair, and a previous empyema requiring drainage one year prior. His long-term medications included ramipril 2.5 mg daily, atorvastatin 80 mg daily, aspirin 100 mg daily and omeprazole 40 mg daily.
He presented as a thin man with several tattoos but without overt cachexia, lymphadenopathy, jaundice, rashes, or bruising. He displayed features of conjunctival pallor, but no hepatosplenomegaly. His cardiorespiratory examination was unre-markable, with appreciable dual heart sounds, no discernible flow murmur or gallop, and normal vesicular breath sounds.
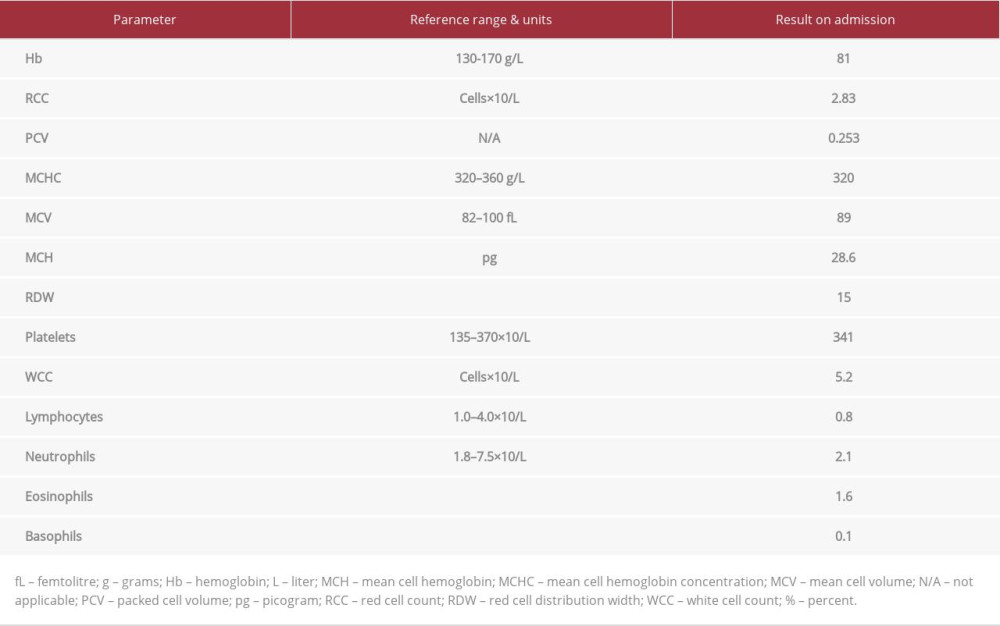
His initial blood investigations revealed a moderate normocytic, normochromic anemia (Table 1), and normal total leukocyte and platelet counts. He was transfused with a further one unit of packed red blood cells, with minimal improvement in his hemoglobin (76 g/L). His hemolysis screen including bilirubin, lactate dehydrogenase (LDH), Coombs test, and haptoglobins, were all unremarkable. His reticulocyte count was inappropriately suppressed (0.4%, 9.5 x 109/L, reference range: 20–130×109/L). Blood film analyses showed a normochromic anemia with no schistocytes, parasitic inclusions, or leukoerythroblastic changes. There were no features of an underlying plasma cell dyscrasia with normal serum protein electrophoresis, serum free light chains, and immunoglobulins. His liver function revealed mild cholestatic abnormalities with raised alkaline phosphatase (222 U/L, reference range: 30–110 U/L) and gamma-glutamyl transferase (145 U/L, reference range: <60 U/L). His iron studies showed a hyperferritinemia (1780 μg/L, reference range: 30–620 μg/L) with normal transferrin saturation (41%, reference range: 14–45%). His other blood parameters, including renal function, routine biochemistry, coagulation profile, thyroid function, hepatitis B and C serologies, syphilis serology, cryptococcal antigen, cytomegalovirus (CMV) viral load, vitamin B12, folate, and autoimmune markers (ie, antinuclear antibody – ANA, anti-neutrophilic cytoplasmic antibodies – ANCA), were unremarkable.
Incidentally, his initial bloodwork showed lymphopenia (Table 1), which had been present for two years prior to his admission. Peripheral blood flow cytometry was subsequently performed, showing an undetectable CD4 T-lymphocyte count (<1%) with concurrent reduced CD19 B-lymphocyte levels (6%). HIV-1 and HIV-2 serology with confirmatory western blot analysis and polymerase chain reaction (PCR) testing identified a new diagnosis of HIV-1 with his RNA viral load quantified at 131 826 copies/mL (5.12 log10 copies/mL); these features were consistent with severe AIDS. HIV-2 was not detected. A chemokine receptor 5-delta 32 variant (CCR5Δ32) variant was not detected. The precise mode of HIV-1 infection was unknown and was suspected to be secondary to his previous contacts with sex workers and/or tattooing in Indonesia.
Immunology and Infectious Diseases input were sought to assist with the interplay between his severe, persistent anemia despite multiple blood transfusions and HIV-1/AIDS diagnosis. Parvovirus-B19 serology was performed, and a positive immunoglobulin M (IgM) and G (IgG) were isolated. Subsequent PCR testing confirmed the presence of a chronic parvovirus-B19 infection; this was thought to be causing a PRCA syndrome and could account for his isolated, severe anemia. He was transferred to a tertiary hospital center for further work-up. A bone marrow aspirate and trephine biopsy were performed which confirmed a diagnosis of PRCA secondary to chronic parvovirus B19 infection (Figure 1) in the setting of his HIV-1/AIDS diagnosis. He received two doses of IVIG at a dose of 1 g/kg, without complications. Brisk reticulocytosis with slow incrementation in his hemoglobin were observed (Figure 2). His repeat parvovirus-B19 serology and PCR testing remained positive one month later despite stabilization of his hemoglobin.
His hospital admission was further complicated by several other AIDS-defining features. He developed norovirus and
It was also noted that he had persistent eosinophilia (1.70–2.53×109/L, reference range: <0.50×109/L) during his admission with whole-body pruritus. This was associated with waxing and waning eczematous patches affecting his bilateral cubital fossae and chest. In view of the patient’s AIDS diagnosis and residence in rural Indonesia, he received an empiric, four-day course of albendazole 400 mg bid to cover for potential parasitic infections.
With respect to his new chronic HIV-1/AIDS diagnosis, he was promptly started on HAART, including cobicistat 150 mg/elvitegravir 150 mg (integrase inhibitor)/emtricitabine 200 mg (nucleoside analog, reverse transcriptase inhibitor)/tenofovir alafenamide 10 mg (nucleotide analog, reverse transcriptase inhibitor) [Genvoya] daily without any adverse effects. He initially received oral atovaquone 150 mg daily for
Discussion
Anemia, although a common medical presentation, can arise from multiple etiologies and requires careful and thorough interrogation to isolate the underlying cause. PRCA is an uncommon bone marrow syndrome characterized by ineffective erythropoiesis and severe anemia [1,2]. Although multiple causes have been identified [2–8], erythroid suppression by parvovirus-B19 infection is infrequently implicated [9,10]. Acute infections can cause a transient aplastic crisis with mild-to-moderate anemia that resolves with clearance of the virus and without the need for transfusion. Parvovirus-B19 seroprevalence rates among adult Australians are high and correlate with increasing age [11]. Non-resolving erythroid aplasia in the setting of persistent parvovirus-B19 infections are rare and occur in severely immunocompromised patients [9,14–18]. We have reported a rare case of parvovirus-B19-mediated PRCA in an elderly man with a concurrent new diagnosis of chronic HIV-1 and severe AIDS. The case highlights that the effective institution of IVIG and HAART therapy are central to resolving parvovirus-B19-mediated PRCA in HIV/AIDS patients.
Cellular immunity against parvovirus-B19 is mediated by the presentation of viral capsid proteins (VP1, VP2) to CD4 T-lymphocytes via human leukocyte antigen (HLA) Class II molecules [21]. In patients with established HIV-1 infection and AIDS, CD4 T-lymphocyte populations are invariably depleted. This results in uncontrolled parvovirus-B19 viral replication and destruction of erythroid progenitors, leading to severe anemia. Although the mainstay of treatment of PRCA syndromes often focuses on immunosuppressive regimens (ie, cyclosporin, corticosteroids, rituximab) [2,22], viral-based etiologies require an alternate approach. IVIG is reported as an effective therapy to manage virally-driven PRCA [2,23]. It consists of multi-donor serum IgG fractions that bolster the immune response against parvovirus-B19 in immunodeficient individuals [23]. Paradoxically, in patients with autoimmune-mediated PRCA, it suppresses aberrant immunological responses and restores physiological erythropoiesis [24].
Due to the inherent rarity of chronic parvovirus-B19-mediated PRCA, there is a paucity of high-quality clinical literature guiding its clinical management with HAART and IVIG. The prevalence of parvovirus-B19-mediated PRCA in AIDS patients is estimated to be 0.95–4.5% [14]. The successful treatment of parvovirus-B19-mediated PRCA with IVIG was first published in 1989 [15]. Koduri and colleagues (1999) published a further case series evaluating IVIG treatment for parvovirus-B19 PRCA in eight chronically HIV-infected adult patients, which demonstrated similar success [16]. IVIG treatments were prescribed at a dose of 1 g/kg for 1–2 days [16]. Although remission was achieved for approximately six months, disease relapse was identified in all but two patients. Lower CD4 T-lymphocyte counts (<80 cells/mm3) were attributed as a key risk factor predisposing patients to earlier relapse, with these patients requiring subsequent IVIG maintenance therapy [16]. A more recent retrospective French study by Crabol et al (2013) evaluated a total of 133 patients with PRCA (of which 39 had HIV) and reported effective resolution after IVIG was administered at ~2.3 g/kg for approximately five days [9]. Disease relapse requiring further IVIG affected 34% of patients, occurred at an average of 4.3 months, and was more common among male HIV patients [9]. In Australia, the National Blood Authority recommends a total of 2 g/kg IVIG in immunosuppressed patients to treat chronic parvovirus-B19-mediated PRCA, divided over 2–5 days [25]. Of interest, our patient has remained in remission for three years following treatment with IVIG and the immediate institution of HAART for his HIV, with which he has remained adherent. It is likely that these observed, early relapses in the aforementioned studies [9,16] arose due to inadequate CD4 T-lymphocyte recovery, either due to older, less efficacious anti-retroviral HIV therapies, non-compliance with prescribed treatments, or reduced doses of initial IVIG therapy. Other case reports have shown that parvovirus-B19-mediated PRCA can be successfully treated in the short term with HAART alone, without the need for IVIG [17,18]. However, the relapse rate among such patients is unknown due to the paucity of long-term follow-up data.
HIV can also directly cause a myriad of bone marrow anomalies, including anemia and eosinophilia [26–29]. In advanced disease, HIV contributes to reticulocytopenia [27]. The pathogenesis underpinning this observation may arise from HIV infecting mesenchymal stem cells [30] and erythroid progenitors [31], thereby adversely affecting the marrow milieu and cytokine microenvironment. These effects ultimately form a hypo-regenerate marrow, which contributes to impaired erythropoiesis [27,30,31]. HIV also inhibits erythropoietin secretion, thereby further blunting physiological erythropoiesis [32,33]. Within the marrow, albeit paradoxically, hypercellularity is also observed secondary to myeloid hyperplasia and/or dysplasia [26]. Of interest, eosinophilia is frequently reported in HIV patients with advanced disease [28,29]. Parasitic infections (eg, schistosomiasis), drug reactions, and relapsing cutaneous conditions (eg, eczema) are commonly associated with HIV-driven eosinophilia [28,29]. Nevertheless, prolonged HIV infections with progression to AIDS invariably causes profound hematological abnormalities, and when combined with parvovirus-B19-mediated PRCA, significantly impedes the ability of the marrow to mount a physiological response against severe and ensuing anemia.
Conclusions
Severe and persistent anemia warrants consideration of an underlying marrow disorder. In patients with profound immunodeficiency, particularly HIV-1, PRCA can arise due to chronic parvovirus-B19 infections. Bone marrow aspirate and trephine biopsies, coupled with serological and PCR testing for parvovirus-B19, is the current diagnostic criterion standard. Such patients require early intervention with IVIG and immediate initiation of HIV-targeted anti-retroviral therapy. The rapid initiation of these treatments, coupled with lifelong continuance of HAART, serves to facilitate prompt marrow recovery and maintenance of long-term disease remission.
Figures
References:
1.. Pasricha SRS, Flecknoe-Brown SC, Allen KJ, Diagnosis and management of iron deficiency anaemia: A clinical update: Med J Australia, 2010; 193; 525-32
2.. Means RT, Pure red cell aplasia: Blood, 2016; 128; 2504-9
3.. Vlachaki E, Diamantidis MD, Klonizakis P, Pure red cell aplasia and lymphoproliferative disorders: An infrequent association: Sci World J, 2012; 2012; 475313-17
4.. Thompson CA, Steensma DP, Pure red cell aplasia associated with thymoma: Clinical insights from a 50-year single-institution experience: Br J Haematol, 2006; 135; 405-7
5.. Habib GS, Saliba WR, Froom P, Pure red cell aplasia and lupus: Semin Arthritis Rheu, 2002; 31; 279-83
6.. Ide T, Sata M, Nouno R, Yamashita F, Clinical evaluation of four cases of acute viral hepatitis complicated by pure red cell aplasia: Am J Gastroenterol, 1994; 89; 257-62
7.. Xu L, Fang J, Weng W, Pure red cell aplasia associated with cytomegalovirus and Epstein-Barr virus infection in severe cases of Chinese children: Hematology, 2013; 18; 56-59
8.. Vishal K, Shalu G, Smita S, Pure red cell aplasia associated with cytomegalovirus infection: J Pediat Hematol Onc, 2010; 32; 315-16
9.. Crabol Y, Terrier B, Rozenberg F, Intravenous immunoglobulin therapy for pure red cell asplasia related to human parvovirus B19 infection: A retrospective study of 10 patients and review of the literature: Clin Infect Dis, 2013; 56; 968-77
10.. Brown KE, Anderson SM, Young NS, Erythrocyte P antigen: Cellular receptor for B19 parvovirus: Science, 1993; 262; 114-17
11.. Means RT, Pure red cell aplasia: Blood, 2016; 128; 2504-9
12.. Nasir IA, Medugu T, Dangana A, Human parvovirus B19-associated hematopathy in HIV disease: Need for clinicopathological revisit: J Biomed Res, 2018; 32; 1-2
13.. Faddy HM, Gorman EC, Hoad VC, Seroprevalence of antibodies to primate erythroparvovirus 1 (B19V) in Australia: BMC Infect Dis, 2018; 18; 631
14.. Chernak E, Dubin G, Henry D, Infection due to parvovirus B19 in patients infected with human immunodeficiency virus: Clin Infect Dis, 1995; 20; 170-73
15.. Kurtzman G, Frickhofen N, Kimball J, Pure red-cell aplasia of 10 years’ duration due to persistent parvovirus B19 infection and its cure with immunoglobulin therapy: N Engl J Med, 1989; 321; 519-23
16.. Koduri PR, Kumapley R, Valladares J, Teter C, Chronic pure red cell aplasia caused by parvovirus B19 in AIDS: Use of intravenous immunoglobulin – a report of eight patients: Am J Hematol, 1999; 61; 16-20
17.. Vaz SO, Guerra IC, Freitas MI, Marques L, Pure red cell aplasia and HIV infection: What to suspect?: BMJ Case Rep, 2018; 2018; bcr-2018-224625
18.. Sanphasitvong W, Poovorawan K, Boonsuk P, Parvovirus B19 infection in HIV patient with pure red cell aplasia: SE Asian J Trop Med, 2005; 36; 1216-20
19.. Chen LF, Hoy J, Lewis SR, Ten years of highly active antiretroviral therapy for HIV infection: Med J Australia, 2007; 186; 146-51
20.. Günthard HF, Saag MS, Benson CA, Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2016 recommendations of the International Antiviral Society-USA panel: JAMA, 2016; 316; 191-210
21.. von Poblotzki A, Gerdes C, Reischl U, Lymphoproliferative responses after infection with human parvovirus B19: J Virol, 1996; 70; 7327-30
22.. Sawada K, Fujishima N, Hirokawa M, Acquired pure red cell aplasia: Updated review of treatment: Br J Haematol, 2008; 142; 505-14
23.. Schwab I, Nimmerjahn F, Intravenous immunoglobulin therapy: How does IgG modulate the immune system?: Nat Rev Immunol, 2013; 13; 176-89
24.. Nimmerjahn F, Ravetch JV, The anti-inflammatory activity of IgG: The intravenous IgG paradox: J Exp Med, 2007; 204; 11-15
25.. : Pure red cell aplasia (PRCA) [Internet] August 7, 2018, Canberra, Australia, National Blood Authority Australia Available from: www.blood.gov.au/system/files/documents/Pure-red-cell-aplasia-PRCA-CV3.pdf
26.. Tripathi AK, Misra R, Kalra P, Bone marrow abnormalities in HIV disease: J Assoc Phys I, 2005; 53; 705-10
27.. Kreuzer KA, Rockstroh JK, Pathogenesis and pathophysiology of anemia in HIV infection: Ann Hematol, 1997; 75; 179-87
28.. Sivaram M, White A, Radcliffe KW, Eosinophilia: Clinical significance in HIV-infected individuals: Int J STD AIDS, 2012; 23; 635-38
29.. Skiest DJ, Keiser P, Clinical significance of eosinophilia in HIV-infected individuals: Am J Med, 1997; 102; 449-53
30.. Scadden DT, Zaira M, Woon A, Human immunodeficiency virus infection of human bone marrow stromal fibroblasts: Blood, 1989; 74; 317-22
31.. Folks TM, Kessler SW, Orenstein JM, Infection and replication of HIV-1 in purified progenitor cells of normal human bone marrow: Science, 1998; 242; 919-22
32.. Spivak JL, Barnes DC, Fuchs E, Quinn TC, Serum immunoreactive erythropoietin in HIV infected patients: JAMA, 1989; 261; 3104-7
33.. Camacho J, Poveda F, Zamorano AF, Serum erythropoietin levels in anaemic patients with advanced human immunodeficiency virus infection: Br J Haematol, 1992; 82; 119-21
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133