03 August 2022: Articles 
A Case of Lymphomatoid Granulomatosis in a Lymph Node with Unique Clinical and Histopathologic Features
Rare disease
Dharti Patel1ABDEF*, Robin Rinehart1D, Renny G. Abraham1DDOI: 10.12659/AJCR.936862
Am J Case Rep 2022; 23:e936862






Abstract
BACKGROUND: Lymphomatoid granulomatosis (LyG) is a rare lymphoproliferative disorder associated with Epstein-Barr virus (EBV) in which there is an infection of B cells and numerous reactive T cells. The lymphoproliferative disorder progresses to organ infiltration and resultant dysfunction of affected organs. Histologically, it is characterized by a triad of polymorphic lymphoid infiltrate, angiitis, and granulomatosis. The lungs are the most commonly involved sites for lymphomatoid granulomatosis, but other sites that can be involved include the liver, skin, and central nervous system. The signs and symptoms of LyG can vary, and can produce generalized symptoms such as cough, shortness of breath, and chest tightness, but can vary depending on the location of LyG.
CASE REPORT: We report a case of a 60-year-old man who presented with altered mental status. Cross-sectional imaging of the brain was negative for any acute intracranial process, but a fine-needle biopsy of a retroperitoneal lymph node revealed nodular polymorphous mononuclear infiltrates containing atypical large EBV-positive B cells with positive EBER and CD30, consistent with lymphomatoid granulomatosis. The patient was started on a regimen of brentuximab/bendamustine, and instructed to follow up with Oncology on an outpatient basis.
CONCLUSIONS: Treatment options for lymphomatoid granulomatosis are based on the disease grading. Lymphomatoid granulomatosis can be classified by using a grading system determined by the number of EBV-positive large B cell malignant cells, along with necrosis. The most effective treatment for lymphomatoid granulomatosis is unknown, but at this time treatment protocols are based on the grade of the disease. The clinical and histological features of lymphomatoid granulomatosis are discussed in this case report.
Keywords: Hematology, Medical Oncology, Lymphomatoid Granulomatosis, Epstein-Barr Virus Infections, Herpesvirus 4, Human, Humans, Lymph Nodes, Male, Middle Aged
Background
Lymphomatoid granulomatosis (LyG) was first described in 1972 by Liebow [1]. LyG is a rare lymphoproliferative disease involving various organs infected with Epstein-Barr virus (EBV)-positive B cells combined with reactive T cells, characterized by a triad of polymorphic lymphoid infiltrate, angiitis, and granulomatosis [2]. The disease is more common in men, and can sometimes be seen in children with immunodeficiency disorders, and is more prevalent in Western countries than in Asia [3]. Patients may have signs of fever, malaise, cough, and dyspnea, suggestive of infectious disease [4]. We present the case of a 60-year-old man who was admitted with altered mental status, who also had hepatosplenomegaly, pancytopenia, and lymphadenopathy, who was ultimately diagnosed with lymphomatoid granulomatosis.
Case Report
A 60-year-old man with a past medical history of HIV, remote history of hepatitis C, diabetes mellitus type II, and Hodgkin’s lymphoma was admitted to the hospital for altered mental status. On the physical exam, vitals were stable, with temperature 36.8°C, BP 104/55, pulse 84/min, respiratory rate 20/ min, and SpO2 98% on room air. A physical exam revealed that the patient had bilateral lymphadenopathy along the anterior cervical chain; a respiratory exam revealed shallow breathing with diffuse rhonchi; a cardiovascular exam revealed harsh systolic murmur grade 3; the abdomen was soft, nontender, no rebound; and a genitourinary exam he had left inguinal lymphadenopathy.
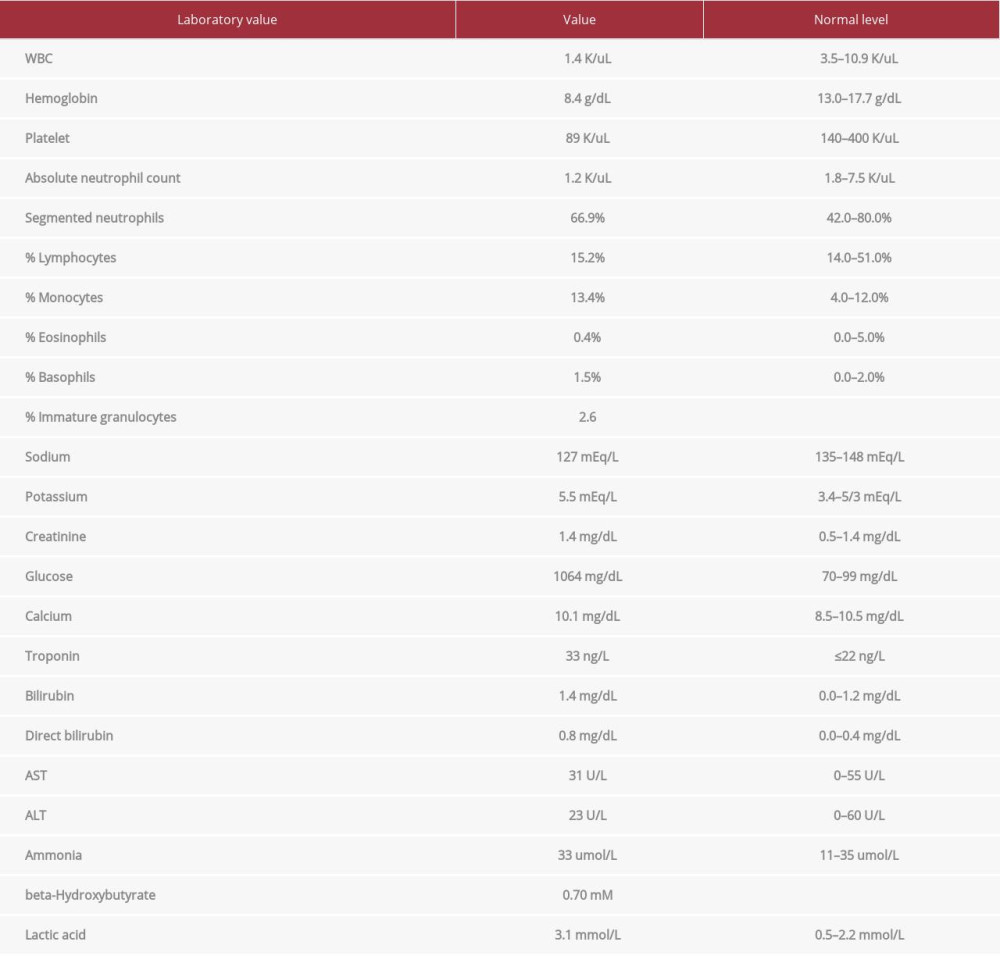
Upon his admission to the hospital, laboratory tests revealed pancytopenia, hyponatremia, hyperkalemia, acute kidney injury, with lactic acidosis (Table 1). A workup for his altered mental status was initiated, with a CT head without contrast not revealing any acute intracranial process; a chest X-ray PA showed airspace opacity of the lateral right lung base, concerning for pneumonia, and blood cultures were drawn in the ER prior to a lumbar puncture. The patient was started on broad-spectrum antibiotics with vancomycin and cefepime; his glucose level was managed with insulin and fluid resuscitation. Blood cultures grew MRSA, a lumbar puncture revealed glucose of 351, colorless fluid, 6 RBC, lymphocytes 30, protein 66.3,and no detection of Enterovirus,
As the patient had MRSA with a cardiac murmur, Cardiology agreed to do a TEE, which ruled out any vegetations. He was showing improvement in his condition with antibiotics and proper glucose control, and was becoming hemodynamically stable, but started to have abdominal pain. A CT scan of the abdomen was positive for moderate splenomegaly without discrete splenic lesions, multiple, and prominent and enlarged lymph nodes (left cardiophrenic, retrocrural, celiac, mesenteric, portacaval, aortocaval, and iliac) (Figure 1). The largest lymph node right common iliac station measured 25.4 mm (Figure 2). Visualization of the lower thorax showed enlarged hilar, subcarinal, and periesophageal lymph nodes. His workup had already ruled out many infectious causes for splenomegaly, but due to the patient’s past history of lymphoma, there was concern for the spread of his lymphoma. The largest lymph node was sampled, and Oncology was consulted. Aspiration revealed EBV-EBER-positive, CD30-positive, and Cd15 rarely positive. LCA, BOB-1, ALK, CD79a, bcl-2, CD3, OCT 2, CD20, PAX-5, and CD68 were also positive in the aspiration sample. In the background of the aspiration, there were also lymphocytes and histiocytes present. AE1/AE3 and HHV8 were negative. Histopathology staining showed fibrinoid necrosis and atypical lymphocytes in the background (Figure 3).
Another slide revealed numerous Epstein-Barr virus-encoded small RNA, with quantification of more than 50 Epstein-Barr virus particles per high-power field. There was also necrosis present, diagnosing grade III LyG (Figure 4). Oncology started the patient on a regimen of brentuximab/bendamustine. He was hemodynamically stable, and was discharged home to follow up with Oncology as an outpatient. He was rehospitalized a few weeks later for another symptom, and had his oncology treatments were put on hold.
Discussion
Lymphomatoid granulomatosis is a rare disease characterized by proliferation of B cells mixed with other reactive T cells that are infiltrated by the Epstein-Barr virus [5]. Lymphomatoid granulomatosis affects males twice as often as females. LyG is more common in middle-age adults in the fourth to sixth decades of life, but it can occur at any age. It has also been reported in children [3].The prevalence of lymphomatoid granulomatosis is unknown. Diseases that have been associated with LyG include organ transplantation, Wiskott-Aldrich syndrome, human immunodeficiency virus (HIV), X-linked lymphoproliferative syndrome, and common variable immunodeficiency syndrome [6]. Our patient has a history of HIV, but was not compliant with his medications for over 25 years. Patients usually present with nonspecific symptoms with cough, dyspnea, chest pain, generalized B symptoms of fever, malaise, weight loss, arthralgias, and myalgias [7]. Patients who have infiltrates in the CNS can show signs of diplopia, hearing loss, dysarthria, ataxia, and altered mental status. Skin manifestations can be painful, and include subcutaneous nodules, maculopapular eruptions, and ulcerations. A few patients are asymptomatic [8]. Lymphomatoid granulomatosis involves a variety of extranodal sites, but the lungs are the most commonly affected (90% of cases) organs in this rare disease. Other common sites include the brain, liver, and skin, and very few cases have been reported in the lymph nodes and spleen [9]. Our patient had LyG in a lymph node.
Histologically, it is characterized by large atypical CD20+ B cells, with a variety of small lymphocytes, plasma cells, and histiocytes in addition to numerous CD3+ cells. The infiltrate can be angio-destructive, with fibrinoid necrosis of involved vessel walls [10]. Positive stains for LyG include CD20, EBV, LMP1, EBER, and CD30. EBNA2 is frequently positive, with background T cells of CD3, with CD4 more often than CD8.CD15 stains [11]. Our patient presented with positive EBER stains, and EBV with less CD15 stains, which is pathognomonic for LyG. Common sites include the lung, skin, or head and neck. Biopsy will reveal necrotizing, angiocentric, and angio-destructive infiltrative processes. The characteristic feature seen with LyG is a combination of polymorphic infiltration of plasma cells, immunoblasts, and typical large lymphoid cells with infiltration into the wall of pulmonary vessels [12].
The Stanford Staging for LyG is into 3 tiers of 3 grades. Grade 1 shows no large atypical cells, little necrosis, and EBV in situ+ cells are rare; grade 2 is occasional large atypical cells, moderate necrosis, EBV in site+ cells 5-20 per high-power field, and some cases spontaneously resolve; grade 3 usually shows large atypical cells, with extensive necrosis.
The most effective treatment for LyG is unknown. Based on the grading of LyG, treatment can be started. For low grades (1 and 2), immune modulators with interferon alpha-2b have been highly effective. Dosing initially can be started with IFN-α, dosed at 7.5 million international units (MIU) 3 times weekly. IFN-α can be escalated as tolerated, every 1 to 2 weeks and continued for 1 year [13]. In patients who have a higher grade, interferon alpha-2b with rituximab has been used.
Targeting high-grade LyG is believed to be more of an autonomous process with a different regimen used. One study showed that the combination of low-dose oral cyclophosphamide and prednisone had a mean remission duration of approximately 5 years [14]. In a prospective study, patients were treated with DA-EPOCH-R (dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab) every 3 weeks for up to 6 cycles of therapy; 18 patients were on this regimen, showing a 77% response rate. In grade 3 LyG, a combination of high-dose chemotherapy with autologous stem cell transplant has been done, but there are only a few anecdotal case reports. Given the low number of patients and the lack of comparative data, superiority among the various immunochemotherapy regimens cannot be determined, and routine use of high-dose chemotherapy/autologous stem cell transplantation as a front-line or adjuvant therapy cannot be recommended in LYG [15].
Another option that has been used in refractory LyG or relapses is a hematopoietic stem cell transplant. The European Group for Blood and Marrow Transplantation did a study on a small number of patients with multiple relapses who were treated with a stem cell transplant. A total of 10 patients were studied, and results revealed that 6 patients remained alive and disease free, 2 had relapses, and 4 had died after transplantation. More studies need to be done to prove the efficacy of hematopoietic stem cell transplantation as a cure for LyG [16].
Conclusions
This case report provides further insight into the clinical presentation, diagnosis, and treatment of a unique disease. The presentation of this patient with LyG in the lymph node versus in the pulmonary system is in itself rare. Treatment outcomes for those who have this disease have been shown to have benefited from combination therapy and even having a hematopoietic stem cell transplant with those who have refractory disease. More research with prospective studies are needed to establish the efficacy in new regimens for lymphomatoid granulomatosis.
Figures
References:
1.. Sýkorová A, Campr V, Kašparová P, [Lymphomatoid granulomatosis – the past and present.]: Vnitr Lek, 2014; 60; 225-38 [in Czech]
2.. Swerdlow SH, Campo E, Pileri SA, The 2016 revision of the World Health Organization classification of lymphoid neoplasms: Blood, 2016; 19; 2375-90
3.. Song JY, Pittaluga S, Dunleavy K, Lymphomatoid granulomatosis – a single institute experience: Pathologic findings and clinical correlations: Am J Surg Pathol, 2015; 39; 141-56
4.. Luce JA, Lymphoma, lymphoproliferative disease and other primary malignant tumors. Murray, Nadel, Mason, Broaddus: Text book of respiratory medicine, 2005; 2, Philadelphia, Elsevier Saunders
5.. Jaffe ES, Wilson W, Lymphomatoid granulomatosis: NORD guide to rare disorders, 2003; 48-49, Philadelphia, PA, Lippincott Williams & Wilkins
6.. Matos C, Gonçalves A, Pereira SG, Lymphomatoid granulomatosis in HIV-2: A rare entity: Cureus; 20211311; 19992-2021
7.. Katzenstein AL, Doxtader E, Narendra S, Lymphomatoid granulomatosis: Insights gained over 4 decades: Am J Surg Pathol, 2010; 34; 35-48
8.. Gangar P, Venkatarajan S, Granulomatous lymphoproliferative disorders: Granulomatous slack skin and lymphomatoid granulomatosis: Dermatol Clin, 2015; 33; 489-96
9.. Sigamani E, Chandramohan J, Nair S, Lymphomatoid granulomatosis: A case series from South India: Indian J Pathol Microbiol, 2018; 61; 228-32
10.. Fletcher CDM: Tumors of the lung and pleura Diagnostic histopathology of tumors, 2021, Elsevier
11.. Guinee DG, Perkins SL, Travis WD, Proliferation and cellular phenotype in lymphomatoid granulomatosis: Implications of a higher proliferation index in B cells: Am J Surg Pathol, 1998; 22(9); 1093-100
12.. Halvani A, Owlia MB, Sami R, Lymphomatoid granulomatosis with splenomegaly and pancytopenia: Zhongguo Fei Ai Za Zhi, 2010; 13; 84-86
13.. Melani C, Roschewski M, Pittaluga S, Phase II study of interferon-alpha and DA-EPOCH+/-R in lymphomatoid granulomatosis: Blood, 2018; 132(Suppl.1); 785
14.. Fauci AS, Haynes BF, Costa J, Lymphomatoid granulomatosis. Prospective clinical and therapeutic experience over 10 years: N Engl J Med, 1982; 14; 68-74
15.. Hu YH, Liu CY, Chiu CH, Hsiao LT, Successful treatment of elderly advanced lymphomatoid granulomatosis with rituximab-CVP combination therapy: Eur J Haematol, 2007; 78; 176-77
16.. Siegloch K, Schmitz N, Wu HS, Hematopoietic stem cell transplantation in patients with lymphomatoid granulomatosis: A European group for blood and marrow transplantation report: Biol Blood Marrow Transplant, 2013; 19; 1522-25
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952791

Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133