24 August 2022: Articles 
An 80-Year-Old Man with Ischemic Heart Disease Who Developed Thrombotic Thrombocytopenic Purpura Following Treatment with Ticagrelor
Challenging differential diagnosis, Diagnostic / therapeutic accidents, Management of emergency care, Rare disease, Adverse events of drug therapy, Educational Purpose (only if useful for a systematic review or synthesis)
Simone A. Jarrett12ABCDEF*, Ammaar Wattoo12ABCDEF, Brenda Chiang12ABCDEF, Gabor Varadi23DF, Mohammad Al Madani24ADEFDOI: 10.12659/AJCR.936977
Am J Case Rep 2022; 23:e936977






Abstract
BACKGROUND: Thrombotic thrombocytopenic purpura (TTP) is associated with widespread microvascular thrombosis, low platelet count, and hemolysis. Ticagrelor is a relatively new agent which functions as a reversible inhibitor of the P2Y12 receptor working to prevent platelet aggregation and is used with or without aspirin in patients with acute coronary syndrome to reduce the risk of myocardial infarction and stroke. We describe the case of an 80-year-old man with ischemic heart disease who developed this rare and potentially fatal adverse reaction known as TTP following treatment with ticagrelor.
CASE REPORT: We report the case of an 80-year-old man who presented with an acute change in mental status 4 months after initiating ticagrelor following percutaneous coronary intervention. Laboratory testing on presentation revealed evidence of microangiopathic hemolytic anemia, thrombocytopenia, and elevated creatinine levels, suggestive of acute renal failure. The combination of his clinical symptoms and laboratory findings were concerning for TTP, likely secondary to ticagrelor use. The patient was treated with therapeutic plasma exchange, systemic steroids, and hemodialysis, which led to resolution of the hemolysis and recovery of renal function.
CONCLUSIONS: Although the association between ticagrelor and TTP is rare, early recognition of this life-threatening complication is essential to decrease morbidity and mortality associated with TTP. Since ticagrelor is now more commonly used, it is important that clinicians be aware of this complication.
Keywords: Adverse Drug Reaction Reporting Systems, Thrombotic thrombocytopenic purpura, acquired, ticagrelor, acute coronary syndrome, Aged, 80 and over, Hemolysis, Humans, Male, Plasma Exchange, Purpura, Thrombotic Thrombocytopenic
Background
Thrombotic thrombocytopenic purpura (TTP) is a rare and life-threatening disorder characterized by platelet aggregation leading to thrombocytopenia and microangiopathic hemolytic anemia (MAHA). Deficiency of the protease ADAMTS13 leads to large multimers of von Willebrand factor (vWF) which promote platelet adhesion to the endothelium. This causes microthrombi to form, which then lead to mechanical shearing of red blood cells and tissue injury [1]. This can manifest clinically as MAHA, thrombocytopenia, renal failure, altered mental status, and fever, historically known as the Moschcowitz pentad, although anemia and thrombocytopenia are the most specific findings [2].
Diagnosis of TTP is clinically challenging due to the diverse clinical manifestations, overlap in clinical presentation with other thrombotic microangiopathies, and limited availability of ADAMTS13 testing [3]. The literature suggests that TTP should be suspected in all patients who present with MAHA and thrombocytopenia unless another etiology is delineated. Despite its rarity, urgent management with initiation of therapeutic plasma exchange can be lifesaving [3]. The presence of ADAMTS13 deficiency in these patients strongly supports the diagnosis. Levels more than 10% are occasionally seen in patients with TTP [4]. However, this test alone does not suffice as the criterion standard by which a diagnosis can be definitively established or excluded.
Antiplatelet therapy is central to treatment strategies for patients with acute coronary syndrome (ACS) to reduce the risk of ischemic complications and to improve survival [5]. Dual antiplatelet therapy with aspirin and a platelet adenosine di-phosphate (ADP) P2Y12 receptor antagonist are the mainstay of treatment. ADP antagonists include thienopyridine anti-platelet agents such as ticlopidine and clopidogrel and nonthienopyridine agents such as ticagrelor. While these medications have the same molecular target, ticagrelor is structurally dissimilar from the other agents, has a faster onset of action, and provides greater inhibition of platelet aggregation in comparison with clopidogrel [6].
Due to the importance of their use in the management of ACS, adverse events with these agents are widely reported [7]. The literature has shown that clopidogrel and ticlopidine have been implicated in the development of drug-induced TTP, but the mechanism remains unclear. Ticagrelor-associated TTP has only been reported twice previously in the literature, by Wang et al and Dogan et al. Consequently, clinical features and response to therapy remain poorly described in the literature. The aim of our study was to highlight this rare complication of ticagrelor and review the literature, while describing the case of a patient who presented with signs and symptoms of TTP following use of ticagrelor in the management of ischemic heart disease.
Case Report
An 80-year-old man with ischemic cardiomyopathy status after stenting of the right coronary artery presented to the Emergency Department with altered mental status, slurred speech, and melena. At baseline, the patient’s mental status was awake, alert, oriented to person, place, and time before the acute onset of his symptoms that morning. His medical history was significant for second-degree heart block after CRT-D placement complicated by pocket hematoma, atrial fibrillation, hypertension, hyperlipidemia, chronic kidney disease stage 2, heart failure with a reduced ejection fraction of 30%, and coronary artery disease.
Four months prior to presentation he underwent percutaneous coronary intervention to the right coronary artery, which was complicated by dissection. At that time, he was started on dual antiplatelet therapy with aspirin and ticagrelor. His other home medications included Lasix 20 mg oral daily, metoprolol succi-nate 25 mg oral daily, sacubitril/valsartan 24-26 mg oral twice a day, aspirin 81 mg oral daily, and atorvastatin 80 mg oral daily.
On arrival, he was hypotensive to 67/48 mmHg, hypothermic to 35.9°C, with oxygen saturation of 96% on room air. Physical examination revealed jugular venous distension, decreased breath sounds, bibasilar crackles, and dysarthria. He was also disoriented and confused. A stroke alert was called and the patient underwent emergent CT head non-contrast, which showed nonspecific white matter changes and no acute intracranial bleed. CT of the chest, abdomen, and pelvis revealed small bilateral pleural effusions, pulmonary edema, and colonic diverticulosis.
Laboratory testing was significant for creatinine of 4.8 mg/dL from a baseline of 1 mg/dL, BUN of 159 mg/dL, AST 273 units/L, ALT 313 units/L, lactate 1.7 mmol/L, troponin 0.21 ng/mL, and BNP 1539 ng/L. He was also noted to be anemic with hemoglobin 8.7 g/dL, hematocrit 26.4%, red cell distribution width (RDW) 18.1%, mean corpuscular volume 95 fL, thrombocytopenic to 40 000 platelets/mcL, and an INR of 1.3. His urinalysis showed WBC 31–50, RBC 11–20, and squamous cells 0–5. Arterial blood gas was pH 7.36, pCO 28 mmHG, and pO2 135 mmHg. A point-of-care echocardiogram showed LVEF ~10% with no pericardial effusion. His EKG revealed normal sinus rhythm with heart rate 73 bpm, normal axis, and T wave inversion in V3–V6, which was new compared to previously. He was emergently stabilized with 1.5 L normal saline fluid resuscitation, started on i.v. norepinephrine infusion, and pantoprazole infusion. He then was admitted to the Intensive Cardiac Care Unit.
His presentation with altered mental status, unexplained thrombocytopenia, anemia, and acute renal failure raised concerns for a diagnosis of TTP. He had findings in keeping with 4 out of the 5 criteria for the diagnosis of TTP [8]. Therefore, a blood smear and hemolytic lab panel including Coombs’s testing, LDH, haptoglobin, bilirubin, and reticulocyte count was ordered. Blood film (Figure 1) revealed numerous acanthocytes, 5–6 schistocytes per high-power field, numerous RBC fragments, polychromasia, occasional spherocytes, large platelets, and decreased platelet count, overall consistent with microangiopathic hemolytic anemia. His LDH was elevated at 562 U/L and his haptoglobin was low at 10 mg/dL, again consistent with hemolysis. His Coomb’s test was negative.
Hematology was consulted and recommended checking the ADAMTS13 level. His ADAMTS13 level was 55%, not suggestive of ADAMTS13 deficiency. The patient was assessed as having TTP secondary to ticagrelor use; therefore, ticagrelor was discontinued. He received 12 sessions of plasma exchange with steroid therapy and was started on continuous renal replacement therapy for treatment of acute renal failure. He had gradual improvement of his mental status and renal function and was discharged to a subacute rehabilitation facility. Unfortunately, the patient was readmitted to the hospital after being in rehabilitation for 1 month with symptoms consistent with a heart failure exacerbation. His hospital course was complicated by sepsis and cardiac arrest, and he eventually died.
Discussion
This case highlights a rare and life-threatening adverse effect of ticagrelor use. It is important for clinicians to be aware of this adverse reaction as ticagrelor is now a commonly prescribed medication in patients with ACS.
Ticagrelor is a non-thienopyridine inhibitor of P2Y12, preventing platelet aggregation by reducing binding of ADP to P2Y124 [9]. Thienopyridines, on the other hand, such as ticlopidine, clopidogrel, and prasugrel, while sharing the same target as ticagrelor, are structurally different and have an alternative binding site on P2Y12.
Drug-associated TTP has been previously attributed to ticlopi-dine and clopidogrel [10]. The pathophysiology of ticlopidine-associated with TTP appears to be immune-mediated, with 100% of patients in the SERF-TTP (Surveillance, Epidemiology & Risk Factors for TTP) sample having detectable levels of neutralizing antibodies to ADAMTS13 [11]. The cases appear to present up to 12 weeks following initiation [11]. In contrast, cases of clopidogrel-associated TTP present within 14 days of initiation of therapy. These patients also generally have normal ADAMTS13 activity and no detectable neutralizing antibodies [12]. The proposed mechanism, considering the absence of evidence of autoimmunity, involves damage or stimulation of the endothelium, leading to secretion of vWF. Prolonged treatment with plasmapheresis is typically necessary.
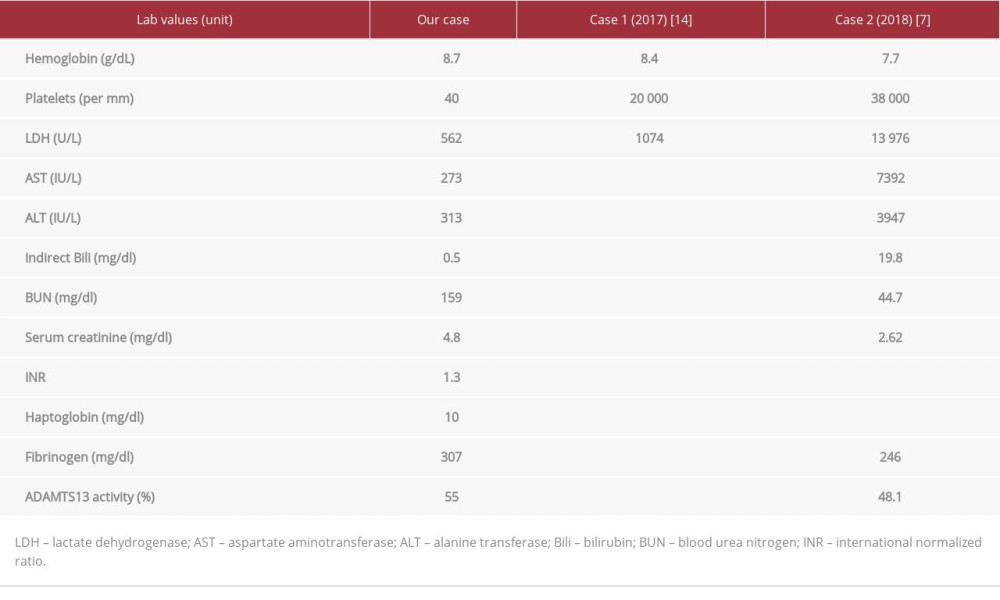
To the best of our knowledge, there are only 2 previously reported cases of ticagrelor-associated TTP (see Table 1). The cases reported by Wang et al and Dogan et al involved male patients with symptom onset occurring 5 and 8 weeks, respectively, after initiation of therapy, while our patient presented 4 months after starting ticagrelor [7,13]. Of note, both cases had a prompt response to therapeutic plasma exchange, which is like our case. Wang et al also found ADAMTS13 activity of 48%, similar to our patient, who had 55% activity [7]. This activity level is suggestive of a non-immune-mediated TTP, and the pathophysiology behind ticagrelor-associated TTP could be more like clopidogrel-associated TTP than ticlopidine-associated TTP. However, the time course after medication initiation and response to therapy are consistent with ticagrelor-mediated TTP. This again shows how little we know about this adverse medication effect and elucidates the importance of needing more literature and research on this topic. Evaluation for the presence of neutralizing antibodies in future cases would also be important in further understanding the pathophysiology of these medications.
Cessation of ticagrelor is an important initial step in the management of these patients, although stent thrombosis is a risk. The concomitant therapy with steroids and plasma exchange was crucial in the management of our patient, which was also noted in similar cases. If those interventions were not successful, rituximab would have been considered for the next line of treatment.
While the differential diagnosis of acute anemia in the setting of gastrointestinal bleed is broad, in this case other etiologies were considered as the patient also presented with altered mental status and profound hypotension. Potential etiologies of his presentation included septic shock due to infection, hemorrhagic shock due to bleeding peptic ulcer or intracranial hemorrhage in the setting of antiplatelet and anticoagulation use, as well as cardiogenic shock with hepatic congestion and coagulopathy due to his history of heart failure. Diseases leading to hemolysis and altered mental status such as disseminated intravascular coagulation and hemolytic uremic syndrome were also considered in the differential, but ultimately a diagnosis of thrombotic thrombocytopenic purpura was made.
Lack of awareness of this complication could ultimately lead to death and it is therefore important that these complications be documented. It is also important to note that ticagrelor should not be prescribed again in patients who have developed ticagrelor-mediated TTP. We believe this may be one of the few case reports in the literature reporting this rare adverse effect and we deem it important that the general population should be aware of it.
Conclusions
This unique case highlights the important but not well investigated rare adverse effect of ticagrelor use. With increasing usage of ticagrelor, this adverse effect can occur at what seems to be any point in time of use, and physicians should maintain a high index of clinical suspicion to make this diagnosis and prevent mortality in light of its increasing use in patients with acute coronary syndrome.
References:
1.. Sadler JE, Pathophysiology of thrombotic thrombocytopenic purpura: Blood, 2017; 130; 1181-88
2.. Yagi H, [Clinical features and laboratory findings of thrombotic thrombocytopenic purpura associated with ticlopidine]: Rinsho Byori, 2005; 53(7); 630-38 [in Japanese]
3.. Chiasakul T, Cuker A, Clinical and laboratory diagnosis of TTP: An integrated approach: Hematology Am Soc Hematol Educ Program, 2018; 2018; 530-38
4.. Froehlich-Zahnd R, George JN, Vesely SK, Evidence for a role of anti-ADAMTS13 autoantibodies despite normal ADAMTS13 activity in recurrent thrombotic thrombocytopenic purpura: Haematologica, 2012; 97; 297
5.. Dhillon S, Ticagrelor: A review of its use in adults with acute coronary syndromes: Am J Cardiovasc Drugs, 2015; 15; 51-68
6.. Dobesh PP, Oestreich JH, Ticagrelor: Pharmacokinetics, pharmacodynamics, clinical efficacy, and safety: Pharmacotherapy, 2014; 34; 1077
7.. Wang X, Zhang S, Li L, Ticagrelor-induced thrombotic thrombocytopenic purpura: A case report and review of the literature: Medicine (Baltimore), 2018; 97(26); e11206
8.. Nuñez Zuno JA, Khaddour K, Thrombotic thrombocytopenic purpura evaluation and management: StatPearls [Internet] Apr 30, 2022, Treasure Island (FL), StatPearls Publishing 2022 Jan. Available at: https://www.ncbi.nlm.nih.gov/books/NBK470585/
9.. Husted S, van Giezen JJJ, Ticagrelor: The first reversibly binding oral P2Y12 receptor antagonist: Cardiovascular Therapeutics, 2009; 27; 259
10.. Zakarija A, Kwaan HC, Moake JL, Ticlopidine- and clopidogrel-associated thrombotic thrombocytopenic purpura (TTP): Review of clinical, laboratory, epidemiological, and pharmacovigilance findings (1989–2008): Kidney Int Suppl, 2009; 75; S20
11.. Zakarija A, Luu TH, Kwaan HC, Thienopyridine-associated thrombotic thrombocytopenia purpura: Updated antibody results from the SERF-TTP study: Blood, 2009; 114; 892
12.. Rashmika PM, Dipa AD, Kamran MM, Clopidogrel induced thrombotic thrombocytopenic purpura: Journal of Cardiology & Cardiovascular Therapy, 2016; 2(3); 555588
13.. Doğan A, Özdemir B, Bal H, Ticagrelor-associated thrombotic thrombocytopenic purpura: Anatol J Cardiol, 2017; 17; 73-74
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133