10 October 2022: Articles 
Myxoid Liposarcoma of the Vulva: A Rare Malignancy Mimicking Benign Vulvar Mass
Challenging differential diagnosis, Rare disease
Dodi Suardi1ABE, Zafli Hamdani2B, Ivonne Golda Palungkun3B, Jessica Kireina1ABEF, Kemala Isnainiasih Mantilidewi1ABE*DOI: 10.12659/AJCR.937575
Am J Case Rep 2022; 23:e937575






Abstract
BACKGROUND: Liposarcoma of the vulva is an exceptionally rare malignant tumor. Clinically, vulvar liposarcoma often mimics benign lesions, thus misdiagnosis is common. Herein, we present a case of myxoid liposarcoma of the vulva. To the best of our knowledge, this is the first case report of vulvar liposarcoma from Indonesia.
CASE REPORT: We present a case of a 39-year-old woman with left vulvar mass of 6 years duration that progressively increased in size. The patient reported having pressure and discomfort, especially during movement, but reported no pain. Lipoma was initially suspected. Surgical excision was performed and histopathological examination revealed a well-differentiated myxoid liposarcoma. The base and excised margins of the tumor were free of malignant cells. Post-operative course was uneventful and she was discharged in a satisfactory condition. The patient had been under regular follow-up and is currently symptom- and recurrence-free. We also review other cases of vulvar liposarcoma to further comprehend characteristics of this rare malignant tumor.
CONCLUSIONS: Liposarcoma of the vulva occurs very rarely, but clinicians and pathologists should always consider it as a differential diagnosis when presented with vulvar mass. Biopsy of a vulvar mass is crucial. Surgical excision remains the mainstay of treatment. Adjuvant radiotherapy may be considered in certain cases. Comprehensive follow-up for recurrences or metastasis is recommended throughout life.
Keywords: Liposarcoma, Liposarcoma, Myxoid, Vulva, Vulvar Neoplasms, Adult, Diagnosis, Differential, Female, Humans, Lipoma, Vulvar Diseases
Background
Liposarcoma represents 20% of all sarcomas in adults, rendering it one of the most common soft tissue sarcomas [1]. Liposarcomas can occur anywhere in the body where adipose tissue is present, but they are most often encountered in the lower limbs, retroperitoneum, and shoulder, as they are large connective tissue spaces where cells can retain potential for lipogenesis [2]. Liposarcoma of the vulva is extremely rare and to date there have been 21 cases reported in the English literature [1,3–16].
Clinical features of vulvar liposarcoma often mimic that of a benign lesion, thus misdiagnosis is common [1,8–16]. Any delay in diagnosis and proper treatment can increase recurrence probability and worsens patient prognosis [9,11]. Since vulvar liposarcoma is exceptionally rare, any knowledge of its incidence may aid in instituting correct management and ensuring best prognosis for the patient.
Case Report
A 39-year-old woman presented to our facility with a left vulvar mass of 6 years duration that progressively increased in size. She reported having pressure and discomfort, especially during movement, since roughly 2 months ago, but aside from that the mass was evidently painless. No significant history of any other diseases was recognized. Physical examination revealed a painless polypoid mass located in the left labium majus. The mass had a diameter of around 8 cm, was soft, fluctuant, and mobile. No signs of inflammation were found. No inguinal lymphadenopathy was noticed. Other external and internal genitalia examinations were all within normal limits. No abnormality was found in any hematological or biochemical panels performed. We did not perform any imaging studies as they were rarely done for vulvar mass cases in our center. Lipoma was initially suspected and a surgery to excise the vulvar mass was planned.
The patient underwent surgical excision of the mass. Frozen section was not performed as the mass was initially suspected to be benign. Macroscopic description of the mass was consistent for a skinned, gelatinous, and fatty tumor measuring about 15×12×9 cm. The cut surface was greyish white, fatty, gelatinous, and glistening (Figure 1). Microscopically, the tumor contains abundant myxoid stroma with arborizing capillary network (“chicken wire”) (Figure 2). Lipoblasts were also seen. No tumor necrosis was found. The base and excised margins of the tumor were free of malignant cells. Histopathological examination revealed the diagnosis of well-differentiated myxoid liposarcoma grade I (based on FNCLCC grading system). The operative and post-operative course were uneventful. She was discharged in a satisfactory condition and had good wound healing. The patient had been under regular follow-up and during each follow-up she was assessed clinically. Currently, at 4 months after surgery, she appears to be symptom- and recurrence-free. She will undergo 6-month evaluations for 2 years, then annually.
Discussion
Vulvar malignancy forms around 5% of all female genital malignancies. Sarcomas account for 1–3% of vulvar malignancies. Liposarcoma of the vulva is extremely uncommon. [17,18]. The World Health Organization (WHO) classifies liposarcoma into 5 histological subtypes: well-differentiated liposarcoma (WDLPS), dedifferentiated liposarcoma (DDLPS), myxoid liposarcoma (MLPS), pleomorphic liposarcoma, and myxoid pleomorphic liposarcoma [19]. Well-differentiated liposarcoma is the most common subtype, followed by myxoid liposarcoma. To confirm the diagnosis of liposarcoma, histopathological examination is essential, whereas molecular pathology examination is desirable whenever available [20]. Due to its location and rarity, diagnosis of vulvar liposarcoma poses a great challenge for both clinicians and pathologists. Misdiagnosis, especially of a benign tumor, is very common. [1,8–16].
The treatment of choice for vulvar liposarcoma is surgical excision. The recurrence rate varies greatly, from 36% to 72%, depending mainly on the presence of negative surgical margins. Any tumor left behind from the initial procedure may increase recurrence probability. Thus, every possible effort should be taken to ensure complete resection during the first surgery [10]. Evidence suggests that vulvar liposarcomas are both responsive and sensitive to radiotherapy [1,9]. Adjuvant radiotherapy should be considered in high-grade lesions or those with positive resection margin, as it may help reduce the likelihood of tumor recurrence [1,21]. On the other hand, chemotherapy’s role in vulvar liposarcoma is unproven. Chemotherapy has been a standard treatment for recurrent liposarcoma. Chemosensitivity levels of each histological subtypes vary greatly. Both well-differentiated and dedifferentiated liposarcomas have been reported to show minimal response to chemotherapy, while myxoid, round cell, and pleomorphic liposarcomas are known to be highly chemosensitive. Adjuvant chemotherapy should only be considered in chemosensitive subtype with metastatic potential [16,22]. Taking into account liposarcoma’s high recurrence rate, thorough follow-up throughout life is recommended [16]. Lack of established protocol specific for vulvar liposarcoma necessitates us to follow the general guidelines available from the National Comprehensive Cancer Network and the European Society of Medical Oncology on soft tissue sarcoma. Both guidelines suggest following patients with high-grade sarcomas every 3–6 months for around 2–3 years, then twice a year for up to 5 years, and annually thereafter. Patients with low-grade sarcomas are recommended to be followed for local relapse every 3–6 months in the first 2–5 years, and then annually [23,24]. We plan to follow our patient every 6 months for 2 years and annually thereafter. Factors affecting vulvar liposarcoma prognosis include pathological subtype, tumor grade, size, depth, and surgical margins.
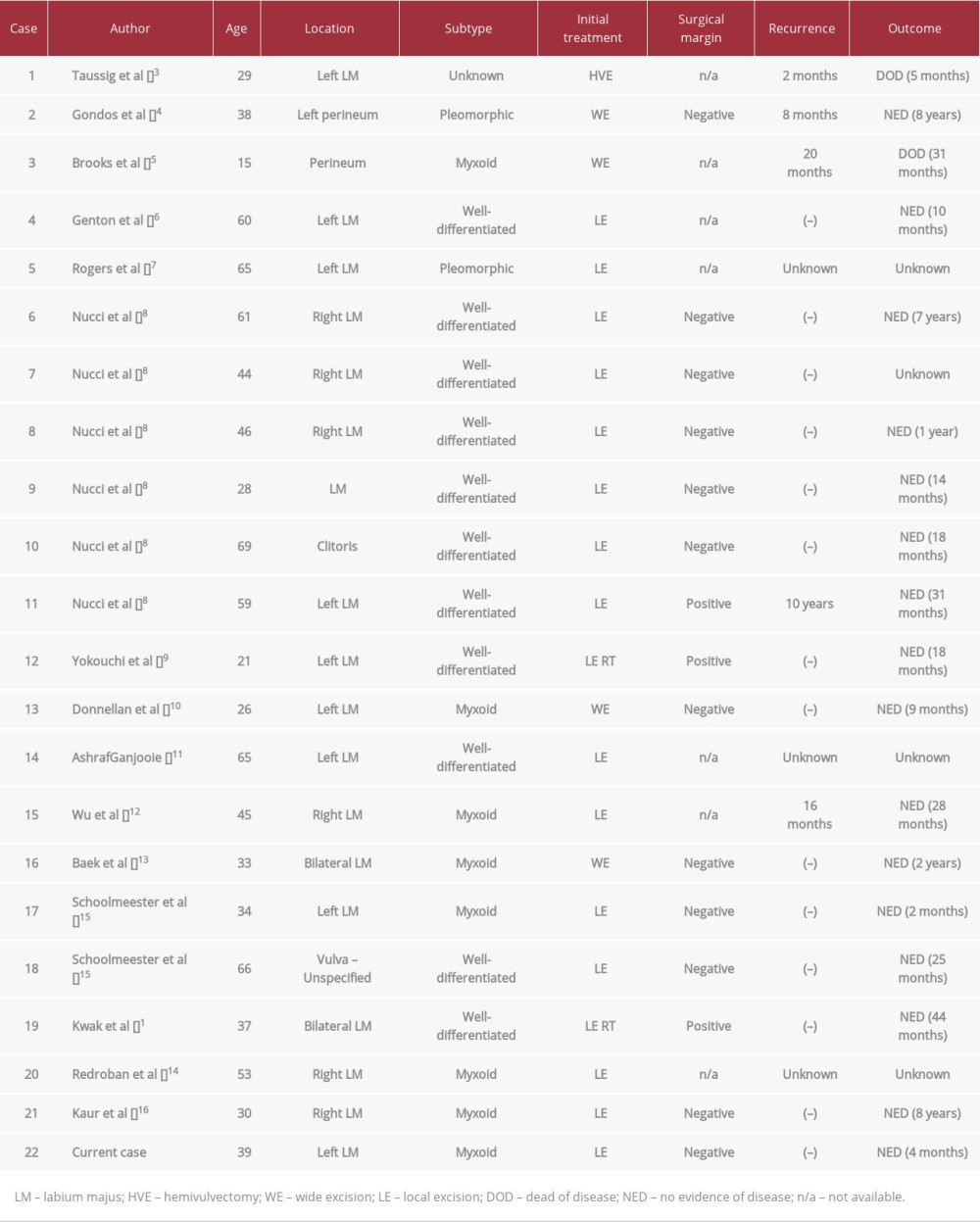
Table 1 lists the 22 reported cases of vulvar liposarcoma in the English literature, including our case [1,3–16]. Liposarcoma most often occurs in the fifth decade of life [11]. The 22 vulvar liposarcoma patients had mean age of 43.7±16.3 years. Fifty percent of the cases (11/22) had well-differentiated liposarcoma. The tumor can involve either the labia majora, clitoris, or perineum, with left labium majus being the most frequent site of origin. Nearly all vulvar liposarcoma cases were first thought to be benign lesions, and most were managed initially with surgical excision. There were 3 patients with positive surgical margins: 2 of whom received adjuvant radiotherapy and experienced no recurrence, while the other had no adjuvant radiotherapy and experienced recurrence. This finding supports previous literature on the efficacy of radiotherapy in reducing recurrence risk. Prognosis of vulvar liposarcoma varied widely. Two patients died due to this disease. The first patient experienced recurrence at 2 months after surgery, subsequently receiving chemotherapy and wide excision but died after 3 months. The second patient experienced recurrence 20 months after initial surgery, subsequently receiving chemotherapy, but died after 11 months. In total, there were 5 recurrences, 1 pleomorphic liposarcoma case, 1 well-differentiated liposarcoma, 2 myxoid liposarcoma, and 1 of unknown subtype (Table 1). These cases are still not sufficient to produce any conclusive remarks on general characteristic of vulvar liposarcoma
Myxoid liposarcoma is the second most common type of liposarcoma, accounting for 20–30% of all liposarcoma [25]. Our present case is the eighth reported cases of myxoid liposarcoma of the vulva. Patients with MLPS tended to be of younger age (range=15 to 53 years; mean=34.4±11.6 years) (Table 1). Macroscopically, MLPS typically presents as a large, circumscribed, and multinodular neoplasm with smooth, gelatinous, and glistening surface. Higher-grade tumors are usually firmer, with a fleshy tan surface. On histopathological examinations, MLPSs are moderately cellular, lobulated tumors with enhanced cellularity at periphery, mixture of non-lipogenic cells and small signet ring lipoblast, prominent myxoid stroma, and rich, branching, thin-walled vasculature known as “chicken wire” capillary. Myxoid liposarcoma also typically lacks nuclear pleomorphism, giant tumor cells, obvious areas of spindling, or blatant mitotic activity. There are 2 ends of this morphological entity; pure myoxid liposarcoma and round cell liposarcoma. Pure myxoid liposarcoma is generally considered a low-grade tumor, but the presence of hypercellular or round cell morphology is associated with significantly poorer prognosis. High-grade MLPSs show >5% hypercellularity, diminished myxoid matrix, less-obvious capillary vasculature, with increased nuclear grade and mitotic activity. Brooks et al reported a case of a 15-year-old girl with poorly differentiated round cell liposarcoma who eventually died after experiencing recurrence [5]. Myxoid liposarcoma has a recurrence rate of 12–25%. Distant metastasis occurs in around 30–60% of cases. Unlike other types of liposarcoma, myxoid liposarcoma has a tendency to metastasize to extrapulmonary sites [20].
Histologically, vulvar myxoid liposarcoma can be mistaken for other myxoid tumors (benign and malignant) more commonly found in the vulva. Benign myxoid lesions of the vulva may include superficial angiomyxoma and myxoid leiomyoma. Malignant myxoid soft tissue lesions include myxofibrosarcoma, aggressive angiomyxoma, myxoid dermatofibrosarcoma protuberans, and embryonal rhabdomyosarcoma [14,26]. These differential diagnoses were ruled out in our case due to the presence of myxoid matrix containing arborizing capillaries (“chicken wire”) and variable number of small non-pleomorphic lipoblasts.
Our case underscores the need for thorough assessment of patients with vulvar mass. Our patient, along with many other reported cases, presented with what appeared to be a typical benign vulvar mass, but histopathological examinations revealed otherwise. Since favorable prognosis of vulvar liposarcoma depends on their early diagnosis and complete excision, clinicians and pathologists should always consider liposarcoma as a differential diagnosis of vulvar mass.
Conclusions
To conclude, liposarcoma occurs very rarely in the vulva. Thus, no protocol regarding its diagnosis and management has been established. Misdiagnosis is common, as vulvar liposarcoma often exhibit benign features. Biopsy of a vulvar mass is crucial. Surgical excision remains the mainstay of treatment. Adjuvant radiotherapy may be considered in certain cases. Comprehensive follow-up for recurrences or metastasis is recommended throughout life.
Figures
References:
1.. Kwak J, Shin S, Kim J, Lee N, Unusual bilateral vulvar liposarcoma: Obstet Gynecol Sci, 2014; 57; 549-52
2.. Zafar R, Wheeler Y, Liposarcoma: StatPearls March 26, 2022, Treasure Island (FL), StatPearls Publishing
3.. Taussig FJ, Louis S, Sarcoma of the vulva: Am J Obstet Gynecol, 1982; 33; 1017-26
4.. Gondos B, Casey M, Liposarcoma of the perineum: Gynecol Oncol, 1982; 14; 133-40
5.. Brooks J, LiVolsi V, Liposarcoma of the perineum: Am J Obstet Gynecol, 1987; 156; 73-75
6.. Genton C, Maroni E, Vulval liposarcoma: Arch Gynecol, 1987; 240; 63-66
7.. Rogers R, Thorp J, Liposarcoma of the vulva: J Reprod Med, 1995; 40; 863-64
8.. Nucci M, Fletcher C, Liposarcoma (atypical lipomatous tumors) of the vulva: Int J Gynecol Obstet, 1998; 17; 17-23
9.. Yokouchi J, Negishi Y, Abe K, Radiotherapy for liposarcoma of the vulva: Gynecol Oncol, 2000; 79; 315-17
10.. Donnellan R, Moodley M, Vulval myxoid liposarcoma: Int J Gynecol Cancer, 2001; 11; 321-22
11.. AshrafGanjooie T, Case report of vulvar liposarcoma: J Obstet Gynaecol Res, 2004; 30; 80-83
12.. Wu T, Tarn J, Vulvar myxoid liposarcoma: Taiwan J Obstet Gynecol, 2007(46); 293-94
13.. Baek J, Park C, Joo S, A case of liposarcoma of the perineum: Korean J Obstet Gynecol, 2007; 50; 932-35
14.. Redroban L, Montalvo N, Vulvar myxoid liposarcoma, an extremely rare diagnosis: A case report and review of literature: Int J Gynecol Pathol, 2019; 38(1); 17-20
15.. Schoolmeester JK, Leifer AJ, Wang L, Hameed MR, Vulvar myxoid liposarcoma and well-differentiated liposarcoma with molecular cytogenetic confirmation: Case reports with review of malignant lipomatous tumors of the vulva: Int J Gynecol Pathol, 2015; 34(4); 390-95
16.. Kaur T, Singh RP, A rare case of a gigantic myxoid liposarcoma of vulva: Case report: Int J Reprod Contracept Obstet Gynecol, 2021; 10(3); 1174
17.. Alkatout I, Schubert M, Garbrecht N, Vulvar cancer: Epidemiology, clinical presentation, and management options: International Journal of Women’s Health, 2015; 7; 305
18.. Chokoeva AA, Tchernev G, Cardoso JC, Vulvar sarcomas: Short guideline for histopathological recognition and clinical management. Part 1: Int J Immunopathol Pharmacol, 2015; 28(2); 168-77
19.. Choi JH, Ro JY, The 2020 WHO Classification of Tumors of Soft Tissue: Selected changes and new entities: Adv Anat Pathol, 2021; 28(1); 44-58
20.. Fletcher C, Bridge J, Pancras C, Mertens F, WHO Classification of Tumours of Soft Tissue and Bone: WHO Classification of Tumours, 2013; 5
21.. Dalal KM, Antonescu CR, Singer S, Diagnosis and management of lipomatous tumors: J Surg Oncol, 2008; 97(4); 298-313
22.. Crago AM, Dickson MA, Liposarcoma: Multimodality management and future targeted therapies: Surg Oncol Clin North Am, 2016; 25(4); 761
23.. von Mehren M, Randall RL, Benjamin RS, Soft tissue sarcoma, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology: J Natl Compr Cancer Netw, 2018; 16(5); 536-63
24.. , Soft and visceral sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up: Ann Oncol, 2012; 23; vii92-99
25.. Chowdhry V, Goldberg S, DeLaney TF, Myxoid liposarcoma: Treatment outcomes from chemotherapy and radiation therapy: Sarcoma, 2018; 2018; 8029157
26.. Goyal LD, Garg P, Kaur M, Sharma D, Recurrent dermatofibrosarcoma protuberans of the vulva: A rare occurrence and review of literature: J Family Reprod Health, 2021; 15; 136-40
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133