25 March 2023: Articles 
Bidirectional Intraoperative Chemotherapy Using Cisplatin and Ifosfamide for Intraperitoneal Mesothelioma in Severe Renal Impairment: A Case Report
Unusual clinical course, Unusual setting of medical care
Razan Almesned1ADEF*, Ayman Z. Azzam23ADE, Ayman Aldeheshi4E, Tarek M. Amin2ADEDOI: 10.12659/AJCR.938192
Am J Case Rep 2023; 24:e938192






Abstract
BACKGROUND: Malignant peritoneal mesothelioma (MPM) is an aggressive neoplasm with a poor prognosis. Bidirectional intraoperative chemotherapy (BDIC) using concurrent intraperitoneal and intravenous chemotherapy in combination with cytoreductive surgery (CRS) is an emerging treatment option for selected cases of MPM. It is a locoregional treatment that involves intraoperative chemoperfusion of heated chemotherapy. The administration of systemic along with intraperitoneal chemotherapy allows for a bidirectional chemotherapy gradient in peritoneal tumor cells. The aim of this treatment is eradication of microscopic residual cancer cells after major removal of macroscopic tumor nodules. To date, there is no consensus on the chemotherapeutic regimen that can be used in BDIC to manage MPM in patients with severe renal impairment. Administering intravenous ifosfamide with hyperthermic intraperitoneal cisplatin and doxorubicin is a promising regimen in treating peritoneal mesothelioma. Nephrotoxicity is a dose-limiting adverse effect of cisplatin and ifosfamide. Therefore, dose adjustment is required in patients with renal impairment.
CASE REPORT: In this report, we describe a 46-year-old female patient with recurrent MPM and severe renal impairment. Her treatment was managed with hyperthermic intraperitoneal cisplatin and doxorubicin along with intravenous ifosfamide following CRS. The cisplatin dose was reduced to 50% and the ifosfamide dose was reduced by 25%. The patient tolerated the procedure well, without deterioration in her renal function. At her 9-month follow-up, she did not report experiencing chemotherapy-related adverse effects, and her kidney function remained stable.
CONCLUSIONS: Severe renal impairment might not be a contraindication to using potentially nephrotoxic chemotherapeutic agents in CRS-BDIC.
Keywords: Cytoreduction Surgical Procedures, hyperthermic intraperitoneal chemotherapy, Mesothelioma, Malignant, Renal Insufficiency, Chronic, Female, Humans, Middle Aged, Cisplatin, Ifosfamide, Combined Modality Therapy, Antineoplastic Combined Chemotherapy Protocols, Hyperthermia, Induced, Mesothelioma, Doxorubicin
Background
Malignant peritoneal mesothelioma (MPM) is a rare neoplasm, with an overall prevalence of 1 to 2 cases per million [1]. It is associated with rapid fatality and a mean symptoms-to-survival time of 345 days [2]. Treatment options for MPM are limited. Initially, cases were managed with palliative systemic chemo-therapy alone or in combination with palliative surgery, with which median survival did not exceed 7 months [3]. Modern treatment of MPM includes the use of hyperthermic intraperito-neal (i.p.) chemotherapy (HIPEC), a locoregional treatment that involves the intraoperative chemoperfusion of heated chemo-therapy to eradicate microscopic tumor cells after the major removal of macroscopic tumor nodules [4]. Many studies reported survival benefits favoring cytoreductive surgery (CRS) plus HIPEC over systemic chemotherapy with palliative surgery [5–7]. A meta-analysis of various studies on MPM demonstrated a 5-year predicted overall survival of 42% [7]. These positive outcomes of CRS and HIPEC encouraged clinicians to use intraoperative intravenous (i.v.) ifosfamide concurrently with HIPEC after CRS in treating MPM. [8,9]. The i.v. administered chemotherapeutic agents reach the residual disease through the capillaries feeding the tumor nodules. The administration of systemic along with i.p. chemotherapy allows for a bidirectional chemo-therapy gradient in peritoneal tumor cells [10,11]. The chemo-therapy dose used in HIPEC is usually a single-shot treatment and in lower doses than the corresponding systemic treatment.
CRS-BDIC using i.v. ifosfamide and i.p. cisplatin plus doxorubicin is an aggressive therapeutic approach that entails morbidity and mortality risks [8]. Among the reported nonsurgical complications is nephrotoxicity, which could be precipitated by the use of cisplatin and ifosfamide. The reported incidence of nephrotoxicity with cisplatin use in HIPEC ranges from 3.7% to 36% [12–14]. Two retrospective studies of BDIC using a systemic ifosfamide and i.p. cisplatin-doxorubicin regimen reported 0% and 33.3% rates of nephrotoxicity [8,15].
Herein, we report a case of a patient with MPM who was known to have stage 5 chronic kidney disease (CKD), and underwent CRS-BDIC using an i.v. ifosfamide and i.p. cisplatindoxorubicin regimen.
Case Report
A 46-year-old woman was referred to our tertiary care center as a case of recurrent mesothelioma with liver metastasis. In 2019 in another center, she underwent CRS, including pelvic exenteration, hysterectomy, oophorectomy, partial peritonectomy, omentectomy, partial resection of the right diaphragm, resection of the rectosigmoid colon, resection of segments 6 and 7 of the liver, ileal conduit urinary diversion, and colostomy creation, followed by HIPEC. In March 2020, she had a recurrence and underwent exploratory laparotomy, local peritonectomy, resection of segment 5 of the liver, and reversal of colostomy, with a loop ileostomy elsewhere. The second operation was complicated by acute kidney injury attributed to a high-output stoma, which progressed to CKD. After that, she received 4 cycles of carboplatin with pemetrexed, which was complicated by multiple admissions due to dehydration and acute kidney injury episodes that mandated withholding of chemotherapy.
Magnetic resonance imaging (Figures 1, 2) and positron emission tomography (Figure 3) showed a peripheral subhepatic lesion in segment 7, measuring 0.7×1.3 cm.
The patient was not exposed to any of the well-known risk factors of mesothelioma, including radiation exposure, asbestos, erionite, or silicate exposure.
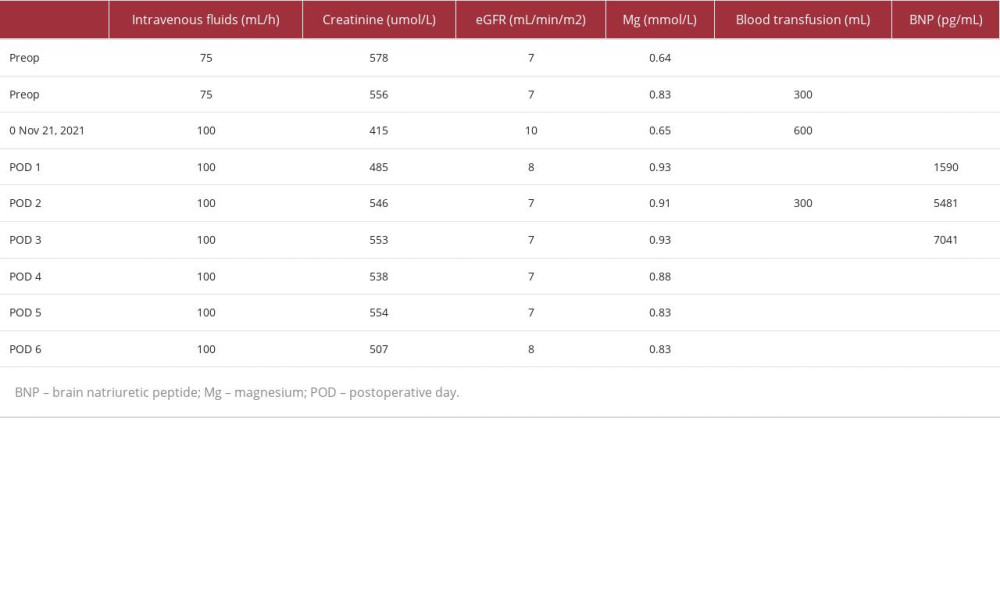
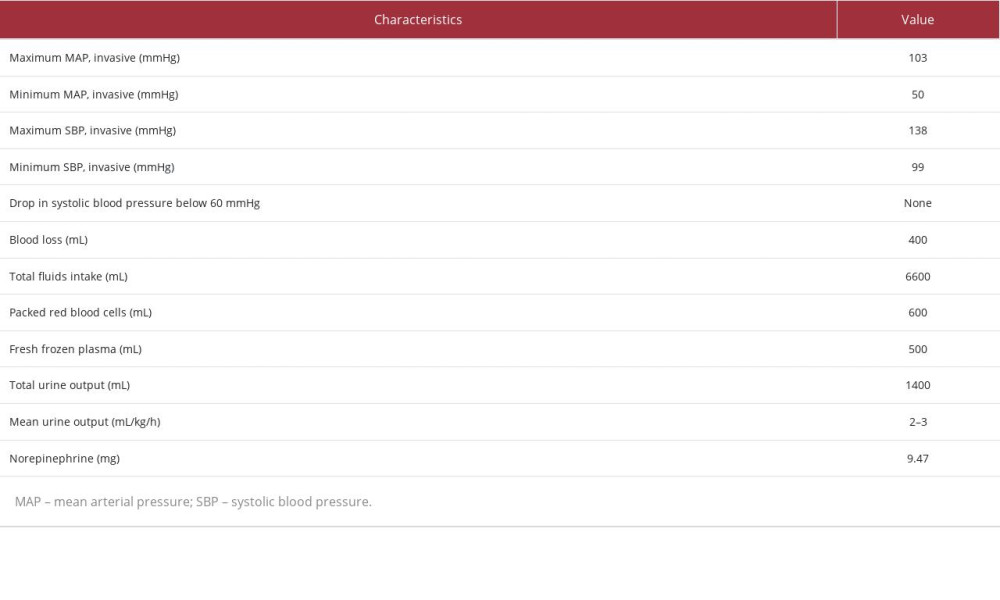
Her preoperative eGFR ranged between 5 and 8 mL/min/m2, and her creatinine level ranged between 734 and 484 umol/L (Table 1). In our center on November 21, 2021, she underwent CRS and HIPEC using 50% of i.p. cisplatin 25 mg/m2 (37.5 mg) plus doxorubicin 7.5 mg/m2 (22.5 mg) infused over 60 min concomitantly with a 75% i.v. ifosfamide dose of 1040 mg/m2. Both i.p. and i.v. chemotherapy were started simultaneously after completing the resection of the subhepatic mesothelioma, partial wedge liver resection, colostomy closure, and appendectomy. Intraoperatively, continuous monitoring was performed using standard ASA and EV1000 hemodynamic monitoring systems (Table 2). A dialysis catheter was inserted in the left internal jugular vein, and a continuous renal replacement therapy machine was present on standby in case the patient became overloaded or developed chemotherapy-related adverse events. Close monitoring of the urine output was done during the operation hourly and every 15 min during the BDIC phase. Her intraoperative urine output was between 2 and 3 mL/kg/h, and mean arterial pressure was between 70 and 90 mmHg. The procedure was completed successfully without immediate complications, and the patient was moved to the Intensive Care Unit in a stable condition. She maintained adequate blood pressure, without the need for inotropes or vasopressors. In the Intensive Care Unit, her mean arterial pressure was maintained above 65, without inotropic support. Her renal function was monitored closely after surgery by a nephrologist. She did not require intraoperative or postoperative hemodialysis.
Histologic sections showed diffuse sheets and nests of epithelioid cells adherent to the liver and bowel wall, with no invasion into the liver parenchyma or bowel mucosa. Multiple foci of necrosis with micro-abscess formation were seen. The tumor cells were medium to large, with irregular contours, abundant eosinophilic cytoplasm, and visible nucleoli. By immunohisto-chemistry analysis, the tumor cells were positive for Pan-CK, CK 5/6, and Calretinin, confirming the diagnosis of mesothelioma (Figures 4–7).
Her postoperative course was complicated with pelvic collection, which was managed with drainage and i.v. antibiotics. The patient was followed up 9 months after the procedure. Her kidney function was stable, and she did not experience chemotherapy-related adverse effects. Her serum creatinine level was 478 umol/L, and her eGFR was 8 mL/min/m2.
Discussion
Cisplatin is a valuable chemotherapeutic agent used in treating various solid organ malignancies. Nephrotoxicity is a dose-limiting adverse effect of cisplatin that can manifest as acute kidney injury, chronic kidney injury, electrolyte disturbances, and anemia [16]. Using i.v. cisplatin in patients with renal impairment places them at increased risk for further deterioration of their renal function. A retrospective study that reviewed 821 patients who received i.v. cisplatin and survived for at least 5 years showed <2% of patients with CKD stage 1 and 6% of patients with CKD stage 3 before treatment progressed to have an eGFR <29 mL/min per 1.73 m2; and <2% of patients with CKD stage 2 progressed to CKD stage 4 [17]. However, none of the patients required hemodialysis [17]. A study that included 113 patients who received cisplatin reported that 19 (12.1%) patients developed new-onset stage 3 CKD; this increase in risk was observed to be directly proportional to the dose administered and the number of cycles [18]. In the same study, the incidence of stage 2 CKD after receiving cisplatin increased from 18.6% to 40.7% [18].
Studies that examined the pharmacokinetics of cisplatin use in HIPEC demonstrated the systematic absorption of cisplatin [19]. When 50 mg/m2 of cisplatin is given i.p., around 46% got absorbed from the peritoneal cavity into the plasma [19]; thus, nephrotoxicity was frequently described after HIPEC using cisplatin at various rates [12,13,16].
Multiple measures have been suggested to prevent cisplatin-induced nephrotoxicity. Hydration with isotonic fluid is the primary approach used to reduce cisplatin nephrotoxicity; however, despite aggressive hydration, the risk of cisplatin nephrotoxicity is not eliminated [20,21]. Prior to the introduction of hydration regimens, initial studies showed a 50% incidence of nephrotoxicity [22,23]. After the introduction of various hydration methods, the incidence of nephrotoxicity lowered to levels reaching 3.7% in some reports [13]. There are no randomized clinical trials investigating the effectiveness of different hydrations regimens.
Ifosfamide is one of the few chemotherapeutic agents that demonstrated heat synergy in pharmacokinetic studies [8]. Ifosfamide and its metabolites have been found in the tumor nodules when it was administered continuously in BDIC [8]. There are available recommendations on the use of reduced doses of chemotherapeutic agents including ifosfamide in the setting of renal impairment [24,25]. Aronoff et al recommend a 25% reduction of the usual dose for patients with eGFR <10 mL/min and full dose for patients with eGFR between 10 and 50 mL/min [24]. Kintzel and Dorr, on the other hand, recommend a 25% dose reduction in creatinine clearance of 45 mL/min and 30% reduction in creatinine clearance of 30 mL/ min [25]. There are only 2 reports in the literature on ifosfamide-induced nephrotoxicity when used in BDIC, which showed 0% and 33.3% [8,15]. The discrepancy between the 2 rates could be explained by the percentage of elderly patients (>65 year of age) included, which was 0% and 27.7%, respectively [8,15].
Conclusions
This case report highlights the success of CRS-BDIC using potentially nephrotoxic chemotherapeutic agents in a patient with renal impairment. However, further studies on this group of patients are needed to aid in patient selection, choice of chemotherapeutic agents, dose adjustment, method of administration, and perioperative care to establish the best practice.
Figures
References:
1.. Alessio B, Padoan I, Mencarelli R, Frego M, Peritoneal mesothelioma: A review: MedGenMed, 2007; 9(2); 32
2.. Manzini VDP, Malignant peritoneal mesothelioma: Tumori, 2005; 91(1); 1-5
3.. Chahinian AP, Pajak TF, Holland JF, Diffuse malignant mesothelioma. Prospective evaluation of 69 patients: Ann Intern Med, 1982; 96(6 I); 746-55
4.. González-Moreno S, Hyperthermic intraperitoneal chemotherapy: Rationale and technique: World J Gastrointest Oncol, 2010; 2(2); 68-75
5.. Passot G, Vaudoyer D, Villeneuve L, What made hyperthermic intraperitoneal chemotherapy an effective curative treatment for peritoneal surface malignancy: A 25-year experience with 1,125 procedures: J Surg Oncol, 2016; 113(7); 796-803
6.. Verma V, Sleightholm RL, Rusthoven CG, Malignant peritoneal mesothelioma: National practice patterns, outcomes, and predictors of survival: Ann Surg Oncol, 2018; 25(7); 2018-26
7.. Helm JH, Miura JT, Glenn JA, Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: A systematic review and meta-analysis: Ann Surg Oncol, 2015; 22(5); 1686-93
8.. van der Speeten K, Stuart OA, Pharmacokinetic study of perioperative intravenous ifosfamide: Int J Surg Oncol, 2011; 2011; 185092
9.. le Roy F, Gelli M, Hollebecque A, Conversion to complete cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma after bidirectional chemotherapy: Ann Surg Oncol, 2017; 24(12); 3640-46
10.. Valle SJ, Alzahrani NA, Liauw W, Hyperthermic intraperitoneal chemotherapy (HIPEC) methodology, drugs and bidirectional chemotherapy: Indian J Surg Oncol, 2016; 7(2); 152-59
11.. de Bree E, Michelakis D, Stamatiou D, Pharmacological principles of intraperitoneal and bidirectional chemotherapy: Pleura Peritoneum, 2017; 2(2); 47-62
12.. Ye J, Ren Y, Wei Z, Nephrotoxicity and long-term survival investigations for patients with peritoneal carcinomatosis using hyperthermic intraperitoneal chemotherapy with cisplatin: A retrospective cohort study: Surg Oncol, 2018; 27(3); 456-61
13.. Hakeam HA, Breakiet M, Azzam A, The incidence of cisplatin nephrotoxicity post hyperthermic intraperitoneal chemotherapy (HIPEC) and cytoreductive surgery: Ren Fail, 2014; 36(10); 1486-91
14.. Sahai SK, Zalpour A, Rozner MA, Preoperative evaluation of the oncology patient: Med Clin N Am, 2010; 94(2); 413-26
15.. Hakeam H, Ayman A, Waleed AT, Amen T, Systemic complications of the bidirectional intraoperative chemotherapy with intravenous ifosfamide and hyperthermic intraperitoneal chemotherapy (HIPEC) using cisplatin plus doxorubicin: Pleura Peritoneum, 2019; 4(4); 20190025
16.. Miller RP, Tadagavadi RK, Ramesh G, Reeves WB, Mechanisms of cisplatin nephrotoxicity: Toxins (Basel), 2010; 2(11); 2490-518
17.. Latcha S, Jaimes EA, Patil S, Long-term renal outcomes after cisplatin treatment: Clin J Am Soc Nephrol, 2016; 11(7); 1173-79
18.. Suer E, Mermerkaya M, Gülpinar Ö, Does the number of cycles of cisplatin based chemotherapy have any effect on renal function in patients with testicular germ cell tumor?: J Urol, 2013; 190(6); 2081-85
19.. Cashin PH, Ehrsson H, Wallin I, Pharmacokinetics of cisplatin during hyperthermic intraperitoneal treatment of peritoneal carcinomatosis: Eur J Clin Pharmacol, 2013; 69(3); 533-40
20.. Crona DJ, Faso A, Nishijima TF, McGraw KA, A systematic review of strategies to prevent cisplatin-induced nephrotoxicity: Oncologist, 2017; 22(5); 609-19
21.. Launay-Vacher V, Rey JB, Isnard-Bagnis C, Prevention of cisplatin nephrotoxicity: State of the art and recommendations from the European Society of Clinical Pharmacy Special Interest Group on Cancer Care: Cancer Chemother Pharmacol, 2008; 61(6); 903-9
22.. Cvitkovic E, Spaulding J, Bethune V, Improvement of Cisdichlorodiammineplatinum (NSC 119875): Therapeutic index in an animal model: Cancer, 1977; 39(4); 1357-61
23.. Wittes RE, Brescia F, Young CW, Combination chemotherapy with cis diamminedichloroplatinum (II) and bleomycin in tumors of the head and neck: Oncology, 1975; 32(5–6); 202-7
24.. Aronoff GR, Bennett WB, Berns JS: Drug prescribing in renal failure: Dosing guidelines for adults and children, 2007, Philadelphia, PA, American College of Physicians
25.. Kintzel PE, Dorr RT, Anticancer drug renal toxicity and elimination: Dosing guidelines for altered renal function: Cancer Treat Rev, 1995; 21(1); 33-64
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133