31 May 2024: Articles ")
A Forgotten Double-J Ureteric Stent as the Core of a Bladder Stone: A Case Report and Literature Review
Unusual clinical course, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Rare coexistence of disease or pathology
Wen-Yan HuangDOI: 10.12659/AJCR.943781
Am J Case Rep 2024; 25:e943781






Abstract
BACKGROUND: Double-J (D-J) ureteric stents are widely applied in urological operations as they play a vital role in maintaining postoperative functionality of the patient’s urinary system and thereby accelerating recovery. D-J stent encrustation may occur due to prolonged retention and lead to secondary complications. We report the case of a forgotten D-J stent that gradually formed into a bladder stone.
CASE REPORT: A 54-year-old man was referred to the Urology Department due to intermittent hematuria, left flank pain, and lower urinary tract symptoms that persisted for 2 weeks. His history was significant for undergoing left ureterolithotripsy followed by the implantation of an ipsilateral D-J stents 2 years ago in a local hospital. The patient did not follow-up regularly or actively seek medical attention for his urinary tract symptoms. Computed tomographic urography revealed a hyperdense tubular object protruding from the left distal ureter to the bladder. The patient underwent cystolithotripsy, left ureteric stent removal, and left ureteroscopy to clear away the bladder stone and its D-J stent core.
CONCLUSIONS: Formation of bladder stones secondary to prolonged indwelling D-J stent and its encrustation is not uncommon in developing countries where the level of public education is low. Prompt D-J stent removal can prevent complications associated with its retention and avoid unnecessary secondary procedures. Endoscopic urologic procedures are safe and feasible management options, and doctor-to-patient communication is vital for a better prognosis.
Keywords: Intraoperative Complications, Ureteroscopy, Urinary Bladder Calculi, Urology, Humans, Male, Middle Aged, Stents, Ureter, Device Removal, Foreign Bodies, Lithotripsy
Introdcution
Implantation of a double-J (D-J) stent is a common urological procedure that ensures ureteral patency by mitigating the risk of ureteric obstruction and stricture formation after uro-logic procedures [1]. Timely removal of the D-J stent is crucial because prolonged indwelling D-J stents can cause complications such as encrustation, urinary tract infections (UTI), hematuria, and irritative bladder symptoms, and stent-related problems such as malposition, migration, and fragmentation [2]. Formation of bladder stones due to neglected D-J stents is rarely reported in the literature and occurs from 3 to 15 years after D-J stent implantation [3–5]. Similar events have occurred in retention of cystostomy tubes and other foreign objects [6]. The pathogenesis of giant bladder stone formation remains unclear, although urinary stasis contributes to 3–8% of cases, with other risk factors being UTI, metabolic abnormalities, and anatomical anomalies of the bladder [7].
We report the case of a 54-year-old man who incidentally was found to have a 3.5-cm bladder stone. Further radiographic evaluation found the stone attached to an encrusted D-J stent that also formed the stone’s core over a period of 2 years. He underwent successful endoscopic fragmentation of the bladder stone and removal of the stent. He was recommended to undergo staged percutaneous nephrostomy to relieve his left distal ureteric stricture and left hydronephrosis, but he rejected this secondary operation and opted for discharge once his left flank pain was relieved.
Case Report
A 54-year-old man was referred to the urological department’s outpatient clinic after his annual physical check-up found a large bladder stone and foreign object on ultrasound. He reported having intermittent hematuria, left flank pain, and a series of lower urinary tract symptoms for 2 weeks prior to the current presentation. Upon admission, he was afebrile and his vitals were stable. The physical examination was un-remarkable for tenderness around the left flank region and no routine biochemical abnormalities were detected. Urinalysis revealed elevated white blood cells (63.7/uL) and red blood cells (1661.5/uL). Two years ago, he underwent left ureterolithotripsy at a local hospital to treat a ureteric stone. Two left D-J stents were implanted to dilate the ureteral stricture found intraoperatively. His postoperative course was uneventful and he claimed to have followed up regularly.
The patient underwent a series of radiographic investigations. Ultrasound revealed mild left hydronephrosis, bilateral nephrolithiasis, generally thickened bladder wall, and a large bladder stone (maximum diameter 3.5 cm). His kidney ureter bladder (KUB) radiograph showed an irregular hyperdense object extending from the orifice of the left ureter into the bladder. Computed tomographic (CT) urography indicated a hyperdense tubular object from the distal ureter to the bladder, leading to the suspicion of D-J stent encrustation and further formation into the core of the bladder stone, accompanied with left hydronephrosis, and cystitis (Figure 1). Upon further history taking, the patient claimed that he did undergo D-J stent removal 1 month after the operation. Therefore, it was suspected that the outpatient physician failed to acknowledge the presence of 2 D-J stents and only removed 1. Despite experiencing postoperative hematuria once or twice a week, the patient was unwilling to seek medical attention. He was advised to undergo elective surgery, which he reluctantly agreed to.
Under general anesthesia, he was placed in the lithotomy position. Preoperative prophylactic antibiotic (amoxicillin clavulanate potassium, 1.2 g) was administered intravenously. A 6/7.5 Fr rigid ureteroscope (Richard Wolf GmbH, Knittlingen, Germany) was introduced into the bladder under direct vision, which identified a large bladder stone connected to an encrusted D-J stent protruding from the left ureteric opening. Pneumatic lithotripsy (Swiss LithoClast Master, EMC Urology, Switzerland) was performed to pulverize the bladder stone and the stone fragments were removed with an ELLIK evacuator (KARL STORZ, Tuttlingen, Germany) and sent for composition analysis. The D-J stent remained intact and was carefully pulled out with grasping forceps (Figure 2). The ureteroscope was advanced to the left ureter following the inserting of a guidewire that was unable to pass through the severely stenosed distal segment of the left ureter despite several attempts. Since the procedure exceeded 3 hours, the chief surgeon decided to conclude the operation after placing a Foley catheter and opted for a staged percutaneous nephrostomy (PCN). Composition analysis revealed the stone was composed of calcium hydrogen phosphate dihydrate and calcium oxalate dihydrate.
The patient’s postoperative course was uneventful and the Foley catheter was removed on postoperative day 2. Postoperative CT found no residual bladder stone (Figure 3). The urological team recommended preoperative assessment of renal function with bilateral renal emission CT and CT urography prior to PCN to manage his hydronephrosis. However, the patient declined any adjuvant investigation or secondary procedure. Once his left flank plain was relieved, he requested to be discharged and did not attend his 1-month postoperative follow-up.
Discussion
Forgotten or retained D-J stents are a source of morbidity that leads to unnecessary secondary surgical intervention and can diminish rapport between patients and physicians. Stent encrustation is one of the most common complications of prolonged D-J stent retention and prolonged indwelling duration is the most significant risk factor [8]. A study reported that the encrustation rate was 26.8% at less than 6 weeks, 56.9% at 6–12 weeks, and 75.9% at more than 12 weeks [9]. In this case, the accidental neglect of the remaining D-J stent 2 years ago became the core of the bladder stone. The patient’s lack of awareness to his urinary symptoms led to poor outcomes of his prior treatment, and his reluctance to undergo a staged operation for definitive management of his urinary stricture also reflects how patients’ decisions can influence postoperative prognosis.
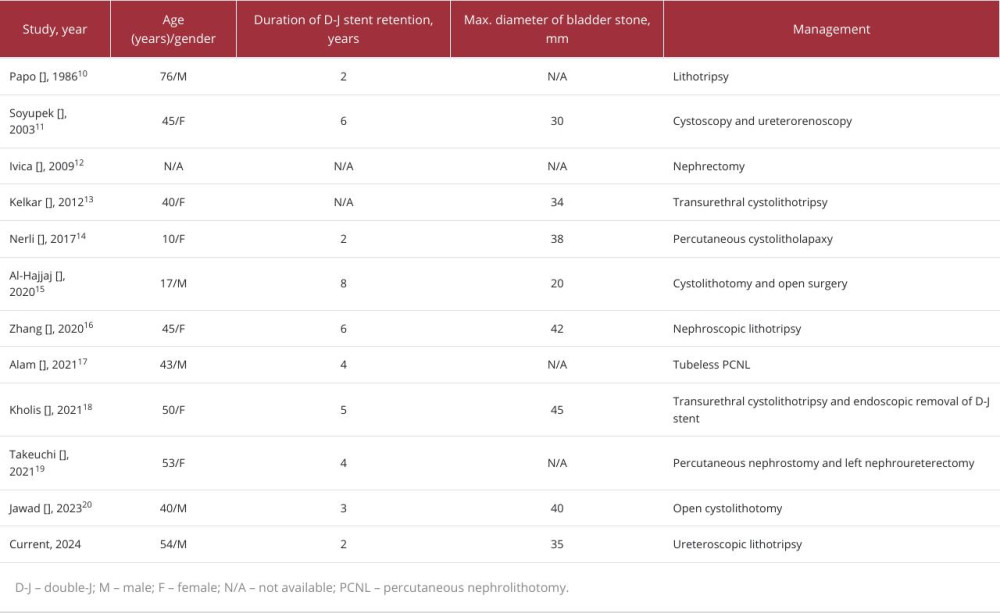
We performed a literature review including cases of bladder stone formation secondary to prolonged indwelling D-J stenting. The keywords used were ‘bladder,’ ‘stone,’ ‘lithiasis,’ ‘calculi,’ and ‘double-J stent.’ A total of 11 case reports were identified and are summarized in Table 1. The mean duration of D-J stent retention was 4.2±2.0 years and the mean maximum diameter of the bladder stone was 35.5±7.9 mm [10–20]. Treatment options varied depending on the stone burden and other accompanying complications. Lithotripsy was conducted to pulverize the stone into fragments suitable for endoscopic retrieval. Certain cases required open surgery. Although the secondary formation of bladder stones is rather uncommon compared to stent fragmentation and renal stone formation, there is an obvious trend that the incidence of stent encrustation is increasing, especially in developing countries.
The metabolic make-up of urine is a determining factor of stent encrustation [21]. The increase in urine pH, urinary tract infection, and stent encrustation are closely associated in a vicious cycle [22]. Therefore, prophylactic antibiotics may be required. Current commercially available stents are mostly made of polyurethanes or silicone [23]. Rebl et al conducted a comparison study on different stent designs that can resist encrustation even after prolonged exposure to urine [21], finding that Styroflex was a superior polymer in terms of surface characteristics, slight hydrophilicity, and negative surface charge, which may serve as reference for future design of stents.
Iatrogenic causes are the most common causes of ureteric strictures, and the previous operation may have contributed to his early stenosis [24,25]. Ureteric strictures can cause urinary stones, infection, and impaired renal function [26]. There are several treatment options for ureteric strictures, but initial treatment strategies involve decompression of the obstructed kidney [27]. Since even a guidewire could not pass through the patient’s left ureter, inserting a new D-J stent was not an option [28]. Therefore, our patient was recommended to undergo PCN to relieve his left hydronephrosis before further management of his urethral stricture, but he declined.
Regardless, it is the physician’s responsibility to closely monitor the postoperative course of patients, especially in the case of D-J stenting where the risk of encrustation or stone formation rises along with the prolonged indwelling interval, which can be life-threatening. Prompt removal can significantly minimize the risk of complications. CT is more accurate than KUB for diagnosis and estimation of the actual stone burden of encrusted stents [29]. Careful preoperative evaluation is necessary as encrusted stents are relatively fragile and can lead to ureteral avulsion and D-J stent rupture. The routine approach is removal with grasping forceps under cystoscopic guidance. Endoscopic procedures such as percutaneous nephrolithotomy, cystolithotripsy, and ureteroscopic lithotripsy are also available options, but treatment should be individualized for each patient. Postoperative CT evaluation can ensure that no D-J stent fragments were retained and that stone clearance was achieved.
Patients are also accountable for their own health. Patient factors, including lack of information on their condition, poor economic status, poor compliance, negligence towards the importance of their procedure, and lower educational status, were the main reasons of D-J stent negligence [30]. With the advancements of technology, there are multiple platforms to use in conducting a postoperative follow-up. In our case, we were unable to effectively communicate with our patient and he was unwilling to undergo further management because his flank pain was relieved. Nonetheless, a patient’s choices must also be respected while the physician must continue to uphold their own responsibilities.
Conclusions
A bladder stone formed along a neglected D-J stent is a rare complication. Endoscopic management of encrusted D-J stents and secondary stones is a safe and feasible method. Urologists should implement strict protocols for D-J stent implantation and removal, such as accurate surgical procedure documentation and providing sufficient patient education to prevent this complication. Additionally, patients should be aware of their health condition and actively seek medical attention as early as possible.
Figures
References:
1.. Damodaran V, Els B, Daras E, The “ins and outs” of the magnetic ureteral stent: A novel innovation in Endourology: Curr Urol, 2023; 17(2); 92-99
2.. Geavlete P, Georgescu D, Mulțescu R, Ureteral stent complications – experience on 50,000 procedures: J Med Life, 2021; 14(6); 769-75
3.. Kumsa ID, Gebreamlak AL, Leul MM, A case report on the management of neglected and forgotten DJ stent for 15 years with severe encrustation and multiple renal and bladder stones: Int J Surg Case Rep, 2023; 103; 107859
4.. Zhang F, Yu J, Wang Q, Lu Y, Urinary bladder stone due to retained indwelling ureteral stent: A case report: Medicine (Baltimore), 2020; 99(39); e22293
5.. Jawad A, Hamdar H, Nahle AA, Bladder stone formation due to neglected double J stent: A case report: Ann Med Surg (Lond), 2023; 85(11); 5716-19
6.. Hidayatullah F, Renaldo J, Kloping YP, Giant bladder calculi due to four years neglected cystostomy: Radiol Case Rep, 2023; 18(11); 3949-53
7.. Childs MA, Mynderse LA, Rangel LJ, Pathogenesis of bladder calculi in the presence of urinary stasis: J Urol, 2013; 189(4); 1347-51
8.. Tomer N, Garden E, Small A, Palese M, Ureteral stent encrustation: Epidemiology, pathophysiology, management and current technology [published correction appears in J Urol. 2022;208(1): 225]: J Urol, 2021; 205(1); 68-77
9.. Kawahara T, Ito H, Terao H, Yoshida M, Matsuzaki J, Ureteral stent encrustation, incrustation, and coloring: Morbidity related to indwelling times: J Endourol, 2012; 26(2); 178-82
10.. Papo J, Waizbard E, Merimsky E, Spontaneous breakage of a double pigtail stent and bladder stone formation: J Urol (Paris), 1986; 92(9); 617-19
11.. Soyupek S, Oksay T, Koşar A, Fragmentation of a forgotten double J stent and excreted with urine: Case report: Int Urol Nephrol, 2003; 35(1); 91-92
12.. Ivica S, Dragan S, Long-term indwelling double-J stents: Bulky kidney and urinary bladder calculosis, spontaneous intraperitoneal perforation of the kidney and peritonitis as a result of “forgotten” double-J stent: Vojnosanit Pregl, 2009; 66(3); 242-44
13.. Kelkar V, Patil D, Management of forgotten double J stent and severe multiple large encrusted stones in the bladder and renal pelvis: Cent European J Urol, 2012; 65(4); 238-41
14.. Nerli RB, Patil SM, Magdum P, Retained double J stent with huge renal and bladder calculi extracted by percutaneous nephrolithotomy and percutaneous cystolitholapaxy in a single encounter: J Endourol Case Rep, 2017; 3(1); 67-69
15.. Al-Hajjaj M, Kazan MN, Neglected double J stent for 8 years with giant bladder calculi formation: A case report: Urol Case Rep, 2020; 32; 101195
16.. Zhang F, Yu J, Wang Q, Lu Y, Urinary bladder stone due to retained indwelling ureteral stent: A case report: Medicine (Baltimore), 2020; 99(39); e22293
17.. Alam S, Ramasamy N, Thirunavukkarasu C, Kumaresan N, Tubeless percutaneous nephrolithotomy (PCNL) for forgotten and retained stent in renal allograft recipient: An interesting case report and lessons learnt: BMJ Case Rep, 2021; 14(1); e238438
18.. Kholis K, Palinrungi MA, Syahrir S, Neglected double-J stent with giant bladder stone: A case report: Pan Afr Med J, 2021; 39; 213
19.. Takeuchi S, Ozawa K, Fujimoto S: Hinyokika Kiyo, 2021; 67(10); 459-63
20.. Jawad A, Hamdar H, Nahle AA, Bladder stone formation due to neglected double J stent: A case report: Ann Med Surg (Lond), 2023; 85(11); 5716-19
21.. Rebl H, Renner J, Kram W, Prevention of encrustation on ureteral stents: Which surface parameters provide guidance for the development of novel stent materials?: Polymers (Basel), 2020; 12(3); 558
22.. Kram W, Buchholz N, Hakenberg OW, Ureteral stent encrustation. Pathophysiology: Arch Esp Urol, 2016; 69; 485-93
23.. Chew BH, Denstedt JD, Technology insight: Novel ureteral stent materials and designs: Nat Clin Pract Urol, 2004; 1; 44-48
24.. Tran H, Arsovska O, Paterson RF, Chew BH, Evaluation of risk factors and treatment options in patients with ureteral stricture disease at a single institution: Can Urol Assoc J, 2015; 9(11–12); E921-E24
25.. Darwish AE, Gadelmoula MM, Abdelkawi IF, Ureteral stricture after ureteroscopy for stones: A prospective study for the incidence and risk factors: Urol Ann, 2019; 11(3); 276-81
26.. Wang Y, Ren X, Ji C, A modified biodegradable mesh ureteral stent for treating ureteral stricture disease: Acta Biomater, 2023; 155; 347-58
27.. Kulkarni R, Metallic stents in the management of ureteric strictures: Indian J Urol, 2014; 30(1); 65-72
28.. Singh V, Srinivastava A, Kapoor R, Kumar A, Can the complicated forgotten indwelling ureteric stents be lethal?: Int Urol Nephrol, 2005; 37(3); 541-46
29.. Weedin JW, Coburn M, Link RE, The impact of proximal stone burden on the management of encrusted and retained ureteral stents: J Urol, 2011; 185(2); 542-47
30.. Jhanwar A, Bansal A, Prakash G, Endourological management of forgotten double J ureteral stents: A single centre study: SM J Urol, 2017; 3(1); 1023
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953110
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952798
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952736
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953993
Most Viewed Current Articles
07 Dec 2021 : Case report
22,757,193
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,264
175,264
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,171
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,170
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133