04 June 2024: Articles 
Rare Pathogens in Peritoneal Dialysis-Associated Peritonitis: A Comprehensive Case Study and Guideline Review
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Rare disease, Adverse events of drug therapy
Abbas Mohammadi1ABCDEF*, Hossein Akhondi1ADE, Dhiresh R. Joshi2DE, Seyed Abbas Mirabbasi1DEDOI: 10.12659/AJCR.943953
Am J Case Rep 2024; 25:e943953






Abstract
BACKGROUND: Peritoneal dialysis (PD) serves as a critical renal replacement therapy for individuals with end-stage renal disease (ESRD), leveraging the peritoneum for fluid and substance exchange. Despite its effectiveness, PD is marred by complications such as peritonitis, which significantly impacts patient outcomes. The novelty of our report lies in the presentation of a rare case of PD-associated peritonitis caused by 2 unusual pathogens, emphasizing the importance of rigorous infection control measures.
CASE REPORT: We report on an 80-year-old African-American female patient with ESRD undergoing PD, who was admitted twice within 8 months for non-recurring episodes of peritonitis. These episodes were attributed to the rare pathogens Achromobacter denitrificans/xylosoxidans and Carbapenem-resistant Acinetobacter baumannii. Despite presenting with similar symptoms during each episode, such as abdominal pain and turbid dialysis effluent, the presence of these uncommon bacteria highlights the intricate challenges in managing infections associated with PD. The treatment strategy encompassed targeted antibiotic therapy, determined through susceptibility testing. Notably, the decision to remove the PD catheter followed extensive patient education, ensuring the patient comprehended the rationale behind this approach. This crucial step, along with the subsequent shift to hemodialysis, was pivotal in resolving the infection, illustrating the importance of patient involvement in the management of complex PD-related infections.
CONCLUSIONS: This case underscores the complexities of managing PD-associated peritonitis, particularly with uncommon and resistant bacteria. It emphasizes the importance of rigorous infection control measures, the need to consider atypical pathogens, and the critical role of patient involvement in treatment decisions. Our insights advocate for a more informed approach to handling such infections, aiming to reduce morbidity and improve patient outcomes. The examination of the literature on recurrent peritonitis and treatment strategies provides key perspectives for navigating these challenging cases effectively.
Keywords: Peritoneal Dialysis, peritonitis, Acinetobacter baumannii, Achromobacter denitrificans, Humans, Female, Aged, 80 and over, Kidney Failure, Chronic, Anti-Bacterial Agents, Gram-Negative Bacterial Infections, Acinetobacter Infections, Practice Guidelines as Topic
Introduction
The worldwide incidence of end-stage renal disease (ESRD) diagnoses is 378 per million per year [1]. Peritoneal dialysis (PD) is the preferred modality for renal replacement therapy (RRT) in most patients with ESRD because of its reputation for safety and efficacy, whereas hemodialysis (HD) is less convenient and demands more advanced equipment [1]. The most common and serious complication of PD is peritonitis and exit-site infection [2]. PD-associated peritonitis occurs in approximately 30% to 40% of patients during their course of PD treatment [2]. This rate can be considered high, especially when compared to the desired outcomes for PD, which aim for lower rates of infection to improve patient quality of life and treatment efficacy. Efforts in clinical practice and research are continuously directed towards reducing this rate through improved sterile techniques, patient education, and the use of advanced PD equipment and protocols. The diagnosis of PD-associated peritonitis is established based on a comprehensive evaluation of clinical manifestations and laboratory findings (Table 1) [3].
In PD patients, occurrence of infections caused by some species like Achromobacter xylosoxidans (previously known as Alcaligenes xylosoxidans) or carbapenem-resistant
In the realm of PD-associated peritonitis, as per the International Society of PD (ISPD) guidelines 2022 and the literature, 2 scenarios emerge when peritonitis occurs within 4 weeks of completing therapy for a preceding infection – it can be attributed to either the same organism (relapse) or a different organism (recurrence). Beyond the 4-week timeframe, if reinfection occurs with the same organism, it is categorized as a repeated infection, while infection with a different organism is considered non-repeat (Table 2) [6, 7].
Despite the wealth of knowledge on relapse and recurrent peritonitis, our understanding of non-repeat infections remains conspicuously sparse. Bridging this knowledge gap is crucial for enhancing our grasp of peritonitis’ varied clinical presentations and for refining our approach to treatment. There is a pressing need for further research to elucidate the underlying mechanisms and dynamics of non-repeat infections. Future studies are needed to shed light on the intricacies surrounding the mechanisms governing these specific scenarios [5,6]. This report delineates an exceptionally uncommon instance of non-repeat PD-associated peritonitis caused by CRAB,
Case Report
An 80-year-old woman undergoing long-term PD presented with altered mentation and sudden seizure-like movements. Her medical history was notable for hypertension, cerebrovascular accident, ESRD, and sick sinus syndrome, for which an implantable cardioverter-defibrillator was placed. The PD regimen involved ultrafiltration of 1 L to 2.6 L via continuous cycling peritoneal dialysis, with a total treatment duration of 10 h interspersed with days off. A week before, the patient had an outpatient visit for abdominal pain, leading to peritoneal fluid analysis that revealed the presence of
Upon presentation to the emergency room (ER), the patient exhibited aphasia and altered mentation. Initial vital sign included a blood pressure of 217/110 mmHg, heart rate of 89/min, respiratory rate of 16/min, and a temperature of 36.7ºC. Laboratory tests showed white blood cell (WBC) count 5.7 mm3/mcl, with neutrophils at 33% and lymphocytes at 49%, elevated blood urea nitrogen (BUN) at 66 mg/dl, creatinine at 3.78 mg/dL, lactic acid at 4.1 mmol/l, procalcitonin at 0.11 ng/ml, and C-reactive protein (CRP) at 1.5 mg/dl. Neuroimaging studies, including brain computed tomography (CT) scan, CT perfusion, and CT angiography with contrast, showed no abnormalities.
Due to the patient’s family report of recent PD-associated peritonitis, peritoneal fluid paracentesis was done, and the analysis exhibited pink hazy fluid with 158 red blood cell count (RBCs) cells/mcl, and 650 WBC cells/mcl, predominantly neutrophils (Table 3, Figure 1). The patient was admitted to the intermediate care unit (IMC) for management of peritonitis using various antibiotics. Initially, she received intravenous (IV) cefepime and metronidazole for 2 days. This regimen was then switched to IV meropenem and IV vancomycin, along with intraperitoneal ceftazidime for 1 day. Subsequently, the treatment was adjusted to IV meropenem, IV eravacycline, and intraperitoneal ceftazidime for 5 days. Ultimately, the antibiotic therapy was modified to intraperitoneal ceftazidime and IV eravacycline (Figure 1). Additionally, the patient experienced a witnessed seizure; a neurologist was consulted, and based on abnormal EEG findings, lacosamide was initiated for seizure management. The patient was discharged in stable condition with 2 additional weeks of intravenous eravacycline, opting to retain the PD catheter. At the time of discharge, the patient remained asymptomatic and repeat peritoneal fluid culture was negative.
Eight months later, the patient presented to the ER with mild abdominal discomfort. She exhibited full orientation and showed no signs of distress, albeit experiencing weakness. Her vital signs were within normal limits. Laboratory investigations revealed a WBC count of 6.9 mm3/mcl, with 47% neutrophils and 35% lymphocytes, hemoglobin level of 6.8 gm/dl, and normal electrolyte levels. Other laboratory values showed BUN 44 mg/dl, creatinine 5 mg/dl, and proNBP 7276 pg/ml. Peritoneal fluid analysis showed a cloudy and bloody fluid with 15 953 RBCs cells/mcl and 483 WBCs cells/mcl. During this admission, all cultures failed to yield any microorganisms, and the diagnosis was made based on clinical presentation and fluid analysis results (Tables 1, 3 and Figure 1). The patient’s treatment began with 5 days of IV meropenem, then transitioned to IP meropenem for 3 days. Following this, the antibiotic therapy was reverted to IV meropenem for an additional 3 days, during which she elected to undergo permanent hemodialysis and she received a permanent hemodialysis catheter. After initial treatment, peritoneal fluid transitioned to a clear, colorless state (Table 3, Figure 1). At discharge, she was placed on a 2-week regimen of IV ertapenem (Figure 1).
The risk factors identified in our patient included advanced age, chronic health conditions, previous episodes of PD-associated peritonitis, history of catheter use, and potentially suboptimal PD technique. In response, we tailored antibiotic treatment according to the culture findings and followed ISPD guidelines, ensuring an effective and targeted approach to manage the infection. Additionally, recognizing the PD catheter as a potential colonization source, its removal was deemed necessary to mitigate the risk of further infection. Considering the transition to hemodialysis, we also suggested the possibility of returning to PD in the future, cautiously noting that careful management and monitoring would be essential to minimize the risk of recurrent peritonitis.
Discussion
This study presents an unusual occurrence of non-repeat PD-associated peritonitis involving
The decision to remove her catheter was driven by thorough physician–patient communication and empathy. Despite her attachment to the PD catheter, the critical need for its removal might not have been fully explained. Infections prompt an immediate review and possible removal of the source, such as an external catheter, to prevent complications. Patients’ hesitance to remove catheters often lead to extended antibiotic treatment for different reasons like due to poor drug delivery to the infection site. However, removing catheters generally leads to more effective treatment, underscoring the need for clear communication and patient cooperation in managing infections [8].
This case underscores concerns regarding patient and healthcare provider knowledge on PD catheter maintenance and infection management. The necessity for informed decision-making in real-world scenarios, encompassing appropriate antibiotic use, hospitalization indications, and catheter removal, is highlighted. The observed deviations from established guidelines emphasize the crucial need for healthcare providers to align their managements with current ISPD recommendations for enhanced antibiotic stewardship (Figure 1) [3]. For CRAB-associated peritonitis, available data on risk factors is scarce, yet it highlights that certain conditions may elevate the risk of developing this infection. These potential risk factors include being age 60 years or older, anemia, hypoalbuminemia, hypokalemia, the presence of diverticulosis, and diabetes [4]. Catheter removal is warranted in instances of refractory peritonitis, and it is advisable to consider earlier removal if the patient’s clinical status is declining. This approach aims to safeguard the peritoneum from potential future peritonitis and mitigate morbidity and mortality. Prolonged efforts to manage refractory peritonitis solely through antibiotic intervention, without catheter removal, are linked to prolonged hospitalization, damage to the perito-neal membrane, heightened susceptibility to fungal peritonitis, and elevated mortality rates [9,10].
The study by Thirugnanasambathan et al stands out as one of the most extensive investigations into patients experiencing both repeated and non-repeat PD-associated peritonitis [6]. Their findings reveal a distinctive temporal pattern, highlighting that the likelihood of a subsequent episode being characterized as repeated, as opposed to non-Repeat peritonitis, reaches its peak in the second month, at 41%. Subsequently, this probability gradually diminishes, stabilizing at 14% from the sixth month onward. Moreover, the median duration between successive episodes of PD-associated peritonitis is delineated as 84 days for instances of repeat peritonitis and 175 days for non-repeat cases. Non-repeat peritonitis is characterized by a culture-negative profile, coupled with a heightened occurrence of non-pseudomonas gram-negative, streptococcal, and fungal organisms. Furthermore, the 2 entities are distinct in that non-repeat peritonitis leads to hospital admission and gets better with simple antibiotics. Repeated peritonitis requires more complex antibiotic treatment. These nuanced findings underscore the multifaceted nature of PD-associated peritonitis, shedding light on temporal patterns, microbial characteristics, and clinical outcomes associated with repeated and non-repeat occurrences [6].
Factors increasing the risk of culture-negative peritonitis encompass recent antibiotic utilization and inadequate culture technique [11,12]. In our clinical encounter, we observed a patient with a second peritonitis, which was culture-negative. After hospitalization and antibiotic treatment, there was resolution of peritoneal fluid clarity. This prompts an exploration into the underlying mechanisms, raising questions about potential factors such as contamination, compromised immune response, age, or the influence of prior antibiotic exposure – elements that warrant investigation to discern the predisposing factors contributing to recurrent infections in this patient cohort.
Among instances of first-time peritonitis associated with PD, 72.4% were ascribed to gram-positive cocci, with only 7.6% linked to Acinetobacter species. Within the Acinetobacter infections, A. baumannii accounted for 87.5%. A. baumannii has become a significant public health concern due to its increasing resistance to various antimicrobial agents. Historically, imipenem and meropenem have exhibited efficacy against it; however, the rise in reports of carbapenem-resistant strains of A. baumannii underlines emerging challenges in combating this pathogen [4]. Achromobacter, a gram-negative bacteria, is predominantly reported in patients with cystic fibrosis and chronic conditions like chronic renal failure [13]. Our case raises concerns about the safety of PD despite its increasing use as a first-line dialysis modality [14]. We emphasize the importance of IP antibiotics and PD catheter removal as essential treatments [2].
The IP route of antibiotic administration is recommended as the primary choice, unless the patient manifests systemic sepsis indicators. Customized, center-specific empirical antibiotic regimens are recommended, ensuring coverage for both gram-positive and gram-negative organisms. For gram-positive organisms, first-generation cephalosporin or vancomycin is recommended, while third-generation cephalosporin or an aminoglycoside is suggested for gram-negative organisms. Cefepime monotherapy is deemed a potentially acceptable alternative in the formulation of empirical antibiotic regimens [3]. The treatment approach for peritonitis varies based on the causative organism (Table 4) [3]. If there is no clinical response after 5 days, early catheter removal is recommended. Extending antibiotic treatment beyond ISPD recommendations, as demonstrated in a randomized controlled study, does not decrease the risk of relapse, recurrence, or repeat peritonitis. Additionally, it may elevate the risk of repeat peritonitis and pose a heightened risk of secondary fungal peritonitis [15].
The adoption of this practice exhibits variability across international centers. Ensuring the proper immobilization of the PD catheter and mitigating mechanical stress on the exit-site emerges as a potentially beneficial strategy for reducing exit-site infection rates. It is imperative to underscore the mandatory nature of promptly treating exit-site or catheter tunnel infections, as this is crucial in diminishing the subsequent risk of peritonitis [16–18]. A meta-analysis reveals that the administration of pre/peri-operative intravenous vancomycin may mitigate the risk of early peritonitis [19]. Additionally, antifungal prophylaxis, using either oral nystatin or fluconazole, is associated with a diminished risk of fungal peritonitis subsequent to an antibiotic regimen [19].
In the realm of preventive measures, specifically concerning exit-site care, the current recommendation advocates the topical application of antibiotic cream or ointment to the PD catheter exit site. Additional preventive measures include advising PD patients to promptly consult their dialysis center if the aseptic conditions of PD exchanges are compromised, denoted as wet contamination. Furthermore, antibiotic prophylaxis is advised before undergoing colonoscopy and invasive gynecological procedures. Draining PD fluid to maintain abdominal emptiness before endoscopic gastrointestinal and invasive or instrumental gynecological interventions is recommended. It is suggested to restrict the presence of pets in the room where PD exchanges occur, as well as where dialysis tubing, equipment, and machinery are stored [3].
Our investigation has unveiled an exceedingly rare case of peritoneal dialysis-associated peritonitis, showcasing a relapse with uncommon bacterial involvement. The findings underscore existing gaps in healthcare knowledge, particularly concerning the optimal management of such cases. Our study illuminates deficiencies in recognizing when hospitalization is warranted, selecting the most suitable antibiotics in adherence to stewardship principles, and establishing robust follow-up protocols for patients grappling with this condition.
Conclusions
In conclusion, the emergence of peritonitis cases due to uncommon pathogens like Achromobacter and CRAB highlights the critical need for comprehensive knowledge of prevention and treatment tactics. This encompasses recognizing particular environmental influences and patient behaviors, prioritizing education for PD patients, and promoting antibiotic stew-ardship and the reconsideration of new guidelines in practice. Implementing these practices is vital for an integrated management strategy among healthcare practitioners.
Tables
Table 1.. Diagnostic criteria for peritoneal dialysis-associated peritonitis [20].![Diagnostic criteria for peritoneal dialysis-associated peritonitis [20].](https://jours.isi-science.com/imageXml.php?i=t1-amjcaserep-25-e943953.jpg&idArt=943953&w=1000) Table 2.. Classification of peritoneal dialysis-associated peritonitis scenarios.
Table 2.. Classification of peritoneal dialysis-associated peritonitis scenarios.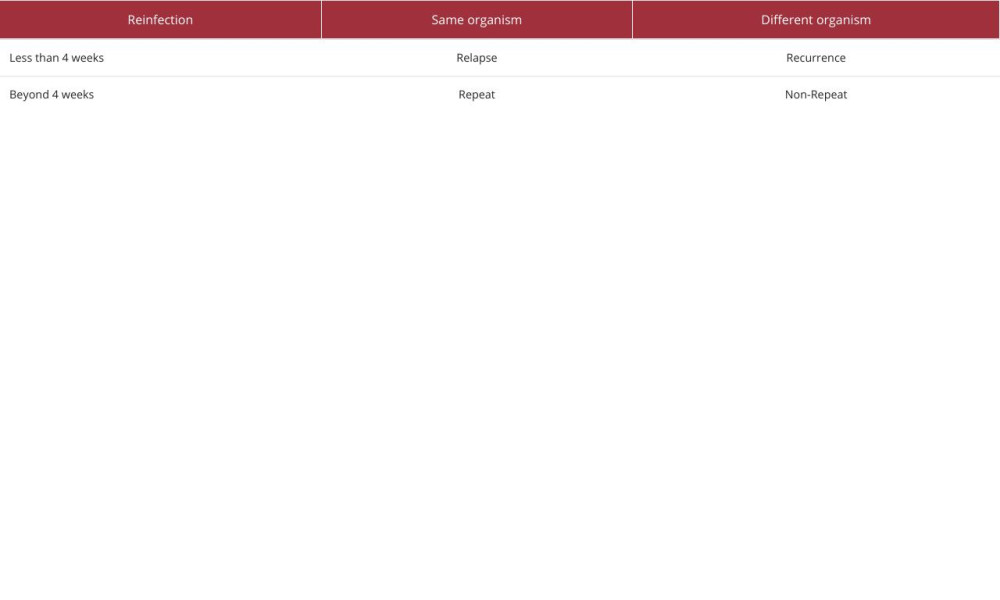 Table 3.. Peritoneal dialysis fluid analysis results from our patient.
Table 3.. Peritoneal dialysis fluid analysis results from our patient.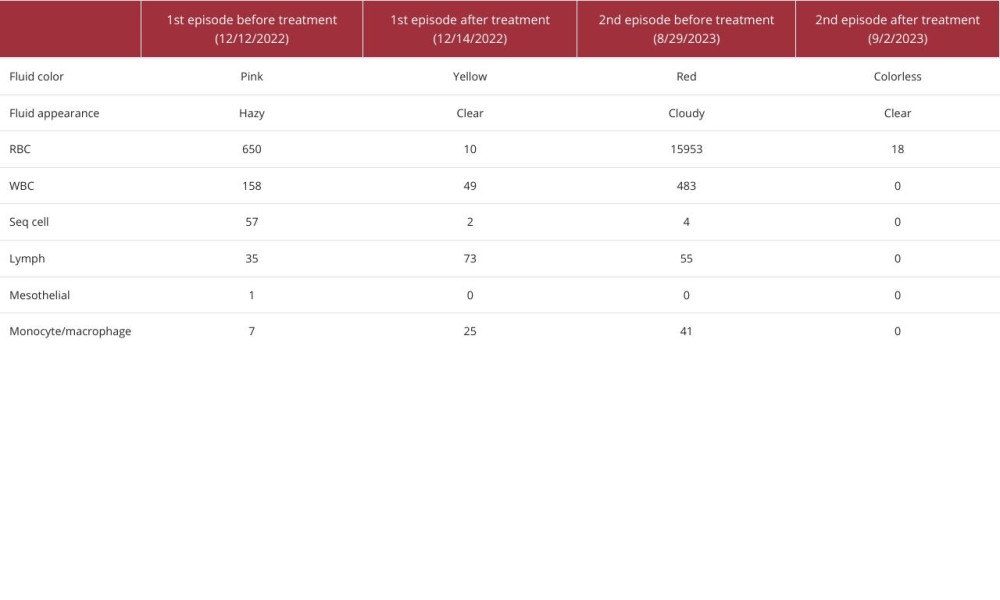 Table 4.. Recommended antibiotics and treatment duration guidelines for peritonitis according to causative organism.
Table 4.. Recommended antibiotics and treatment duration guidelines for peritonitis according to causative organism.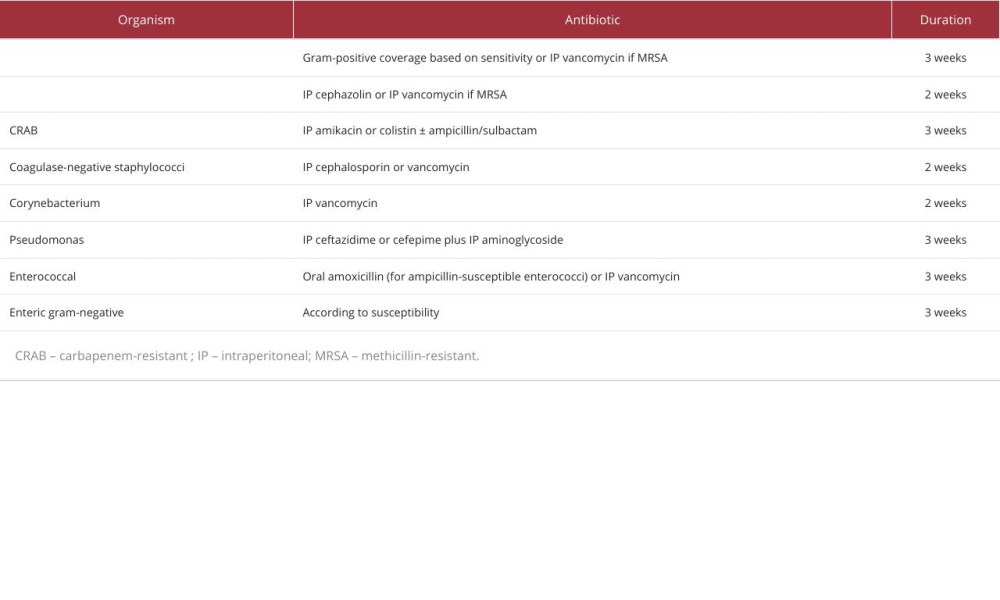
References:
1.. Ye H, Yang X, Yi C, Urgent-start peritoneal dialysis for patients with end stage renal disease: A 10-year retrospective study: BMC Nephrology, 2019; 20(1); 238
2.. Perl J, Harel Z, Nessim SJ, Peritoneal fluid analysis in peritoneal dialysis – associated peritonitis: JAMA, 2022; 328(21); 2157-58
3.. Li PK-T, Chow KM, Cho Y, ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment: Perit Dial Int, 2022; 42(2); 110-53
4.. Zhang W, Wu YG, Qi XM: Perit Dial Int, 2014; 34(3); 317-21
5.. Donderski R, Grajewska M, Mikucka A: Case Rep Nephrol, 2018; 2018; 9454520
6.. Thirugnanasambathan T, Hawley CM, Badve SV, Repeated peritoneal dialysis-associated peritonitis: A multicenter registry study: Am J Kidney Dis, 2012; 59(1); 84-91
7.. Li PK, Chow KM, Cho Y, ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment: Perit Dial Int, 2022; 42(2); 110-53
8.. Berrington A, Gould FK, Use of antibiotic locks to treat colonized central venous catheters: J Antimicrob Chemother, 2001; 48(5); 597-603
9.. Choi P, Nemati E, Banerjee A, Peritoneal dialysis catheter removal for acute peritonitis: A retrospective analysis of factors associated with catheter removal and prolonged postoperative hospitalization: Am J Kidney Dis, 2004; 43(1); 103-11
10.. Lu W, Kwan BC, Chow KM, Peritoneal dialysis-related peritonitis caused by Pseudomonas species: Insight from a post-millennial case series: PLoS One, 2018; 13(5); e0196499
11.. Szeto CC, Wong TY, Chow KM, The clinical course of culture-negative peritonitis complicating peritoneal dialysis: Am J Kidney Dis, 2003; 42(3); 567-74
12.. Fahim M, Hawley CM, McDonald SP, Culture-negative peritonitis in peritoneal dialysis patients in Australia: Predictors, treatment, and outcomes in 435 cases: Am J Kidney Dis, 2010; 55(4); 690-97
13.. Isler B, Kidd TJ, Stewart AG, Achromobacter infections and treatment options: Antimicrob Agents Chemother, 2020; 64(11); e01025-20
14.. Szeto CC, Li PK, Peritoneal dialysis-associated peritonitis: Clin J Am Soc Nephrol, 2019; 14(7); 1100-5
15.. Szeto CC, Ng JK, Wing-Shing Fung W, Extended antibiotic therapy for the prevention of relapsing and recurrent peritonitis in peritoneal dialysis patients: A randomized controlled trial: Clin Kidney J, 2021; 14(3); 991-97
16.. Szeto CC, Li PK, Johnson DW, ISPD Catheter-related infection recommendations: 2017 update: Perit Dial Int, 2017; 37(2); 141-54
17.. Boudville N, Johnson DW, Zhao J, Regional variation in the treatment and prevention of peritoneal dialysis-related infections in the Peritoneal Dialysis Outcomes and Practice Patterns Study: Nephrol Dial Transplant, 2019; 34(12); 2118-26
18.. Lin J, Ye H, Li J, Prevalence and risk factors of exit-site infection in incident peritoneal dialysis patients: Perit Dial Int, 2020; 40(2); 164-70
19.. Campbell D, Mudge DW, Craig JC, Antimicrobial agents for preventing peritonitis in peritoneal dialysis patients: Cochrane Database Syst Rev, 2017; 4(4); CD004679
20.. Perl J, Harel Z, Nessim SJ, Peritoneal fluid analysis in peritoneal dialysis-associated peritonitis: JAMA; 2022 [Online ahead of print]
Tables
Table 1.. Diagnostic criteria for peritoneal dialysis-associated peritonitis [20].Table 2.. Classification of peritoneal dialysis-associated peritonitis scenarios.Table 3.. Peritoneal dialysis fluid analysis results from our patient.Table 4.. Recommended antibiotics and treatment duration guidelines for peritonitis according to causative organism.Table 1.. Diagnostic criteria for peritoneal dialysis-associated peritonitis [20].Table 2.. Classification of peritoneal dialysis-associated peritonitis scenarios.Table 3.. Peritoneal dialysis fluid analysis results from our patient.Table 4.. Recommended antibiotics and treatment duration guidelines for peritonitis according to causative organism. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133