01 July 2024: Articles ")
Cryptogenic Multifocal Ulcerating Stenosing Enteropathy: A Rare Case of Small Bowel Stenosis
Challenging differential diagnosis, Diagnostic / therapeutic accidents, Management of emergency care, Rare disease
Jie Peng1BCE, Yalu ZhangDOI: 10.12659/AJCR.944218
Am J Case Rep 2024; 25:e944218






Abstract
BACKGROUND: Cryptogenic multifocal ulcerating stenosing enteropathy (CMUSE) is a rare noninfectious chronic inflammatory disease of the digestive tract confined to the small bowel. Chronic inflammatory wasting leads to protein loss and weight reduction, and some patients eventually develop small bowel stenosis. The etiopathogenesis of CMUSE remains unknown.
CASE REPORT: A thin 62-year-old man was admitted to the hospital with abdominal pain and distension accompanied by bilateral lower-extremity edema for 2 months. After a series of medical tests, rheumatic or immune-related diseases, hyperthyroidism, and tuberculosis were excluded, and common digestive system diseases were also excluded. Abdominal CT showed incomplete obstruction of the small bowel. Enteroscopy showed small-bowel luminal narrowing. The patient subsequently underwent partial resection of the small bowel with end-to-side anastomosis. The small-bowel stricture was about 120 cm from the ileocecal junction, and about 12 cm of small bowel was resected. Postoperative pathology of the resected material revealed multifocal ulceration of the mucosa with massive inflammatory cell infiltration and extensive hyperplastic fibrous tissue, consistent with the characteristics of CMUSE disease. At follow-up 6 months after surgery, he had no abdominal pain or distension, and his anemia and lower-extremity edema were improved.
CONCLUSIONS: CMUSE diagnosis requires a combination of patient history, imaging, endoscopy, pathology, and exclusion of other digestive disorders, such as Crohn’s disease. It is a chronic wasting disease, often accompanied by weight loss, abdominal pain, melena, and hypoproteinemia. Surgery is an important treatment for intestinal strictures caused by CMUSE.
Keywords: Enteritis, Intestinal Diseases, Double-balloon enteroscopy, Abdominal Pain, Humans, Male, Middle Aged, Intestinal Obstruction, Intestine, Small, Ulcer, Constriction, Pathologic
Introduction
Cryptogenic multifocal ulcerating stenosing enteropathy (CMUSE) is a rare disease that presents clinically with anemia, abdominal pain, abdominal distension, hypoproteinemia, and malnutrition [1]. Regarding the nomenclature, it is called CMUSE in Europe and USA, and chronic nonspecific multiple ulcers of the small intestine (CNSU) in Japan, but whether these 2 diseases are the same is unclear [2].
The diagnostic criteria for CMUSE have not yet been fully established [3]. Perlmutter et al [4] proposed 5 main points of diagnosis of CMUSE: (1) unexplained small-intestinal stenosis and obstruction; (2) superficial ulcers in the mucosa and submucosa; (3) Chronic course, recurrent attacks, and easy recurrence after surgery; (3) normal inflammatory response parameters; (4) effective glucocorticoid therapy; and (5) no other small-intestinal ulcerative diseases. The diagnostic criteria for CMUSE proposed by Matsumoto et al focus more on intestinal lesions [5]: (1) persistent and occult blood loss from the GI tract except during bowel rest or postoperative period; (2) confirmation of characteristic small-intestinal lesions by macroscopy, radiography, or enteroscopy, including: i) circular or oblique in alignment; ii) sharply demarcated from surrounding normal mucosa; iii) geographic or linear in shape; iv) multiple lesions < 4 cm from each other; v) ulcers not reaching proper muscular layer; vi) scarred ulcers presumed to be the healing stage of those characterized by i.v. if treated by bowel rest. In 2017, Hwang et al proposed new diagnostic criteria [6]: (1) unexplained small-bowel strictures; (2) superficial ulcers of the mucosa and submucosa; (3) chronic or recurrent ulcerative strictures and abdominal pain; (3) no signs of systemic inflammation; and (4) persistent occult blood loss from the gastrointestinal tract, except during bowel rest or the postoperative period.
Imaging and endoscopy are important methods for diagnosing CMUSE. CT examination provides a reference for the diagnosis of CMUSE. A retrospective study by Ramos et al found that the CT findings of CMUSE were mainly multiple, short segment (<2 cm), circumferential stenosis, intestinal wall thickening, proximal small-intestinal dilatation, and generally no manifestations of intestinal perforation, but they had similar imaging features to Crohn’s disease and NSAID-related enteritis [7]. Furthermore, endoscopic examination, including double-balloon enteroscopy, wireless capsule endoscopy, retrograde motorized spiral enteroscopy, is an important means of exploring small-intestinal lesions and diagnosing CMUSE [8]. However, caution is required when performing capsule endoscopy because the endoscope may not pass through. CMUSE patients were endoscopically characterized by short circumferential ulcerative strictures, predominantly small bowel, no abnormalities in the colon, and ≥1 stricture site [9].
Only about 200 cases of CMUSE have been reported worldwide, and there is limited understanding of the pathogenesis, clinical manifestations, diagnosis, and proper treatment [10]. Clinical manifestations of CMUSE are very similar to those of Crohn’s disease, involving only the small bowel, intestinal tuberculosis, non-steroidal anti-inflammatory drugs (NSAID)-associated enteritis, and eosinophilic enteritis involving the small intestine, thus it is easily misdiagnosed. There are currently limited reports on CMUSE-induced intestinal stenosis. Herein, we report a patient who underwent surgical treatment for cryptogenic multifocal ulcerative stenosing enteritis to improve the understanding of this rare disease.
Case Report
PRESENT HISTORY:
A 62-year-old man with body mass index (BMI) of 18 kg/m2 was admitted due to abdominal pain and distension for 2 months on August 16, 2023. He initially visited the gastroenterology clinic 3 times, without improvement. To identify the cause, he was hospitalized to complete the relevant examinations. The right lower-abdominal distension and pain were mainly persistent, but tolerable, with loss of appetite and significantly reduced food intake, accompanied by gradual edema of both lower limbs, without fever, jaundice, hematemesis, or melena. He had insomnia, decreased stool frequency, normal urination, and weight loss of about 10 kg within the past 6 months.
PAST MEDICAL HISTORY:
The patient had a history of coronary heart disease and cardiac insufficiency, without regular treatment. He denied any history of hepatitis, tuberculosis, hypertension, diabetes, cerebrovascular disease, food or drug allergy, or family history of genetic diseases. Importantly, he denied any history of surgery, trauma, or taking non-steroidal anti-inflammatory drugs.
PHYSICAL EXAMINATION:
His body temperature was 36.5°C, pulse was 61 beats/min, respiration was 19 breaths/min, and blood pressure was 114/70 mmHg (1 mmHg≈0.133 kPa). He was thin, had pale skin with slight laxity, his subcutaneous adipose tissue was atrophic, and his consciousness was unimpaired. The shape of the bowel was visible around the umbilicus, the abdomen was raised, and the flexibility of the abdominal texture was similar to touching the tip of the nose. He had mild tenderness in the whole abdomen, no muscle tension or rebound tenderness, and there was no palpable mass in the abdomen.
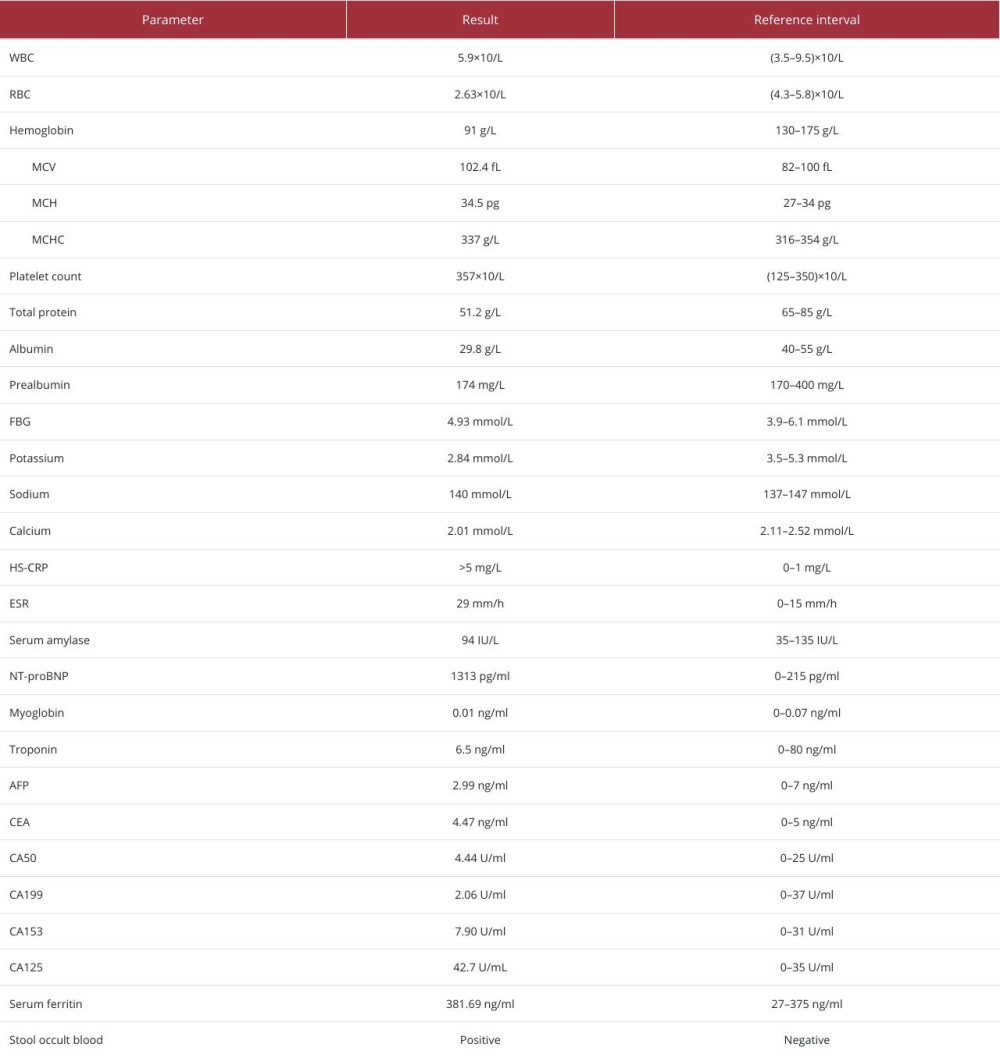
TEST RESULTS:
The specific test data and relative reference ranges are summarized in Table 1. Coagulation function testing and liver and kidney function tests showed no significant abnormalities. Thyroid function (T3, T4, TSH), thyroglobulin, thyroglobulin antibody, and thyroid peroxidase antibody levels were normal. Antinuclear antibody profiles and vasculitis antibody profile were normal. Mycobacterium tuberculosis enzyme-linked immunospot assay (T-SPOT.TB) was nonreactive.
MAIN EXAMINATIONS:
(1) Abdominal ultrasound showed a hepatic cyst; colonic dilatation with fecalith formation (considering incomplete intestinal obstruction), thickening of colonic wall; and abdominal effusion. (2) Abdominal standing plain film revealed incomplete intestinal obstruction. Extensive dilated bowel loops with air-fluid levels in the middle abdomen (Figure 1A). (3) Abdominal CT revealed wall thickening with enhancement in some small intestines and proximal bowel obstruction (Figure 1B). (4) Double-balloon enteroscopy showed significant narrowing of the intestinal lumen and difficulty in passing the enteroscope (Figure 1C).
ADDITIONAL EXAMINATIONS:
(1) Electrocardiogram (ECG): sinus rhythm; left ventricular high voltage. (2) Echocardiography showed mitral regurgitation (mild), aortic regurgitation (small), and left ventricular ejection fraction of 64%. (3) Chest CT showed scattered inflammation, emphysema and bullae in both lungs. (4) Gastroscopy: esophagitis, chronic non-atrophic gastritis. (5) Histopathological examination after gastroscopic biopsy showed: (biopsy of distal esophagus) chronic inflammation of the mucosa, small foci of mild dysplasia of the squamous epithelium.
DIAGNOSIS:
CMUSE, intestinal stenosis, abdominal effusion, anemia, hypoproteinemia, hypokalemia, malnutrition, chronic gastritis, pulmonary inflammation, pulmonary bullae, heart failure, history of coronary heart disease.
TREATMENT:
The symptoms of abdominal distension and abdominal pain were not obvious in the early stage, so the patient had not received any anti-inflammatory therapy, and was given diuresis, nutritional support, and maintenance of water and electrolyte balance after admission. The intestine stenosis was not detected until the patient was hospitalized for CT and enteroscopy, with an estimated duration of at least 2 months. In addition, due to the inability to accept multiple relapses of small-intestine stricture at the same location, the patient refused endoscopic dilation, and opted for surgical treatment, although there is a risk of recurrence after surgery.
Because the abdominal pain and distension progressively worsened, laparoscopic exploration was performed under general anesthesia after fully communicating the surgical risks with the patient and his family. Intraoperative exploration revealed that the lesion was located in the small intestine, 120 cm from the ileocecal junction, with a narrow lumen, falling into the pelvic cavity, and severely adherent to the surrounding tissue (Figure 1D). It was difficult to complete laparoscopically and was changed to open surgery for safety reasons. After careful release of adhesions, the strictured lesion along with the surrounding normal bowel was removed about 12 cm and an end-to-side anastomosis of the small bowel was performed. The entire procedure lasted 3 hours 10 minutes, with intra-operative bleeding of about 100 ml, and the patient was discharged uneventfully 7 days after surgery.
Postoperative pathological examinations, including HE and Masson staining, are shown in Figure 2. Immunohistochemistry: CK (pan) (+), Syn (partial +), CgA (partial +), S100 (+), Dog-1 (−), Ki-67 (+, about 40%).
Follow-up: After the surgery, the patient refused to take glucocorticoids orally due to concerns about dependence, and did not receive treatment with other medications. The follow-up tests included abdominal physical examination, abdominal ultrasound, blood routine, liver function, renal function, albumin, electrolytes, and C-reactive protein. The follow-up frequency was postoperative 2 weeks, 1 month, 3 months and 6 months. Six months after the operation, the patient had good appetite, normal eating, no nausea or vomiting, was without abdominal pain or abdominal distension or other discomfort, and his hemoglobin and albumin levels had returned to normal.
Discussion
We present a case of a 62-year-old man who presented with symptoms of abdominal pain and distension accompanied by bilateral lower-extremity edema for 2 months, who later received a diagnosis of CMUSE after a series of medical examinations. CMUSE is one of the most difficult digestive system diseases to diagnose in time, and the lesions are usually located in the small intestine, which is rare in clinical work. The diagnosis of CMUSE needs to be combined with medical history and medical tests. Finally, surgery may be required in patients with CMUSE-induced intestinal stenosis.
Serum ferritin is an important form of iron storage and reflects the iron stores of the body. Our patient had gastrointestinal blood loss, while serum ferritin levels did not decrease, but increased slightly. We speculate that this may be related to inflammatory disease, as both ESR and HS-CRP were elevated, suggesting a high level of inflammation. Serum ferritin is a nonspecific marker that increases in response to infection, inflammation, and stress, and is associated with inflammatory and cardiovascular diseases [11]. Recognizing iron deficiency accompanying anemia in chronic disease can be difficult because serum ferritin levels are usually normal or elevated due to circulating inflammatory cytokines.
Diseases with similar symptoms to CMUSE include Crohn’s disease, NSAID-associated enteropathy, and intestinal tuberculosis. Crohn’s disease is a chronic inflammatory granulomatous disease with longitudinal ulceration and cobblestone-like appearance of the diseased mucosa, involving the entire thickness of the intestine, and may have extraintestinal manifestations such as cutaneous erythema nodosum, arthritis, and eye disease [12]. Unlike Crohn’s disease, CMUSE presents as the short annular ulcerations limited to the small intestine and lacks systemic inflammation and fistula/fissure formation. It features nonspecific inflammatory infiltration, lesions limited to the mucosa and submucosa without transmural extension, and the absence of typical extraintestinal manifestations associated with Crohn’s disease [13,14]. Hence, it can be differentiated from Crohn’s disease by enteroscopy and clinical presentation. Similar to CMUSE, the endoscopic appearance of NSAID-induced lesions presents as superficial ulcers and multiple short strictures of the small intestine, while NSAID-induced injury also occurs in the stomach and the colon [15]. The best discriminating method is the history of NSAID use and gradual spontaneous recovery after discontinuation. In this case, the patient did not have a history of taking NSAID-related drugs, so the diagnosis of NSAID-associated enteropathy was not considered. Intestinal tuberculosis has systemic symptoms such as fatigue and night sweats, the lesions are mostly in the ileocecal junction and terminal ileum, and the lesions show annular ulcers, while caseating granulomas and Mycobacterium tuberculosis can be detected by enteroscopic biopsy [16]. Our patient had no history of tuberculosis, no tuberculosis lesions on chest CT, and no symptoms of low-grade fever or night sweats; hence, intestinal tuberculosis could be excluded.
T-SPOT.TB is a new-generation immunological diagnostic technique for detection of tuberculosis infection [17]. It is a T-cell-based interferon-gamma release assay (IGRA) developed in recent years.
The diagnosis of CMUSE should be based on clinical manifestation, typical endoscopic and radiological features, and histopathological examination, combined with exclusion diagnosis. Genetic analysis is helpful in the diagnosis of CMUSE, and future studies may clarify the relationship between CMUSE and CEAS [13]. Some studies have found that SLCO2A1 mutations exist in some patients with ulcerative small-intestinal strictures, so it is also known as chronic enteropathy associated with the SLCO2A1 gene (CEAS), but this description generally appears in Japan, and the relationship between CEAS and CMUSE has not been determined [18]. In addition, in European siblings with severe CMUSE, deletion of the PLA2G4A gene resulting in deletion of the C-terminal 43 amino acids of cytosolic phospholipase A2-α (cPLA2α) was found to cause impaired platelet aggregation [19]. However, PLA2G4A mutations were not identified in any of the patients diagnosed with CMUSE based on clinical and endoscopic examinations, while screening for SLCO2A1 mutations might play an essential role in the diagnosis of CMUSE [20]. Therefore, CMUSE may be an important cause of small-intestinal stenosis, with a lack of specificity in diagnosis and more reliance on clinical experience and pathological examination, while genetic testing is an important reference for diagnosing CMUSE.
Because of the rarity of CMUSE, current treatments for CMUSE are based on case reports or case series, and no prospective controlled trials have elucidated the optimal treatment strategy. We reviewed the treatment experience of more than 20 cases reported in series. A French survey showed a 70% recurrence rate of symptoms after surgery, and steroid therapy was effective, but dependence easily developed [14]. A study from Korea showed a corticosteroid response rate of only 25%, 69.2% of patients recovered completely after surgery, and only 7.7% of patients required reoperation [13]. A single-center retrospective study in China (37 years, 25 cases) showed that the treatment improvement rate was only 56%; patients who underwent surgery had relieved obstruction and bleeding symptoms, but the postoperative recurrence rate was high (76.9%). The clinical benefit rate of standard systemic glucocorticoid therapy was 44.4%; the clinical improvement rate of mesalazine therapy was 28.6%; and the clinical remission rates of azathioprine, methotrexate, and thalidomide therapy were 20%, 25%, and 45.5%, respectively [20]. Furthermore, it has been reported that infliximab (TNF-α antagonist) showed efficacy in a few cases and improved clinical symptoms in steroid-refractory patients with CMUSE [21]. In addition, endoscopic balloon dilatation is an effective method that can be considered for patients with narrow lumens [10,14]. Surgical treatment with segmental resection of the small intestine is the last choice for gastrointestinal bleeding, stenosis, and obstruction caused by CMUSE, but excessive small-intestine resection should be avoided [10]. There is still some risk of recurrence after surgery. Although some drugs such as glucocorticoids can be used as postoperative maintenance treatment options, the effect is limited. To improve the therapeutic effect, further studies on effective treatments are needed.
This case report has the following limitations: (1) lack of long-term follow-up, with a follow-up period of only 6 months, and inability to determine the long-term condition of the patient and whether there was recurrence; (2) failure to detect SLCO2A1 mutations, somewhat reducing the accuracy of CMUSE diagnosis, although genetic testing is not a necessary condition for diagnosis.
Conclusions
Due to the lack of specific clinical symptoms and the difficult accessibility of the small intestine, the diagnosis of CMUSE remains challenging, accompanied by misdiagnosis and delayed diagnosis. Accurate diagnosis requires a clinical history, imaging, digestive endoscopy, pathology, and exclusion of other diseases. Moreover, CMUSE lacks effective treatment methods and is prone to recurrence. For CMUSE-induced intestinal stenosis, the current treatment methods include drug therapy, endoscopic balloon dilatation, and surgery.
Figures
References:
1.. Moreels TG, Singh A, Updates on the diagnosis and management of cryptogenic multifocal ulcerative stenosing enteropathy (CMUSE) and non-steroidal enteropathy: Best Pract Res Clin Gastroenterol, 2023; 64–65; 101847
2.. McAlindon ME, Cryptogenic multifocal ulcerating stenosing enteritis and other under-recognised small bowel inflammatory enteropathies: Curr Opin Gastroenterol, 2022; 38(3); 279-84
3.. Lew C, Jain A, Chua J, Wong A, Cryptogenic multifocal ulcerous stenosing enteritis: A difficult diagnosis: ANZ J Surg, 2022; 92(9); 2373-75
4.. Perlemuter G, Chaussade S, Soubrane O, Multifocal stenosing ulcerations of the small intestine revealing vasculitis associated with C2 deficiency: Gastroenterology, 1996; 110(5); 1628-32
5.. Matsumoto T, Iida M, Matsui T, Yao T, Chronic nonspecific multiple ulcers of the small intestine: A proposal of the entity from Japanese gastroenterologists to Western enteroscopists: Gastrointest Endosc, 2007; 66(3 Suppl.); S99-107
6.. Hwang J, Kim JS, Kim AY, Cryptogenic multifocal ulcerous stenosing enteritis: Radiologic features and clinical behavior: World J Gastroenterol, 2017; 23(25); 4615-23
7.. Ramos GP, Bartlett DJ, Bledsoe AC, Cryptogenic multifocal ulcerous stenosing enteritis (CMUSE): A 20-year single-center clinical and radiologic experience: Abdom Radiol (NY), 2021; 46(8); 3798-809
8.. Belhassine M, Dragean C, Dano H, Moreels TG, Cryptogenic multifocal ulcerative stenosing enteritis (CMUSE) diagnosed by retrograde motorized spiral enteroscopy: Acta Gastroenterol Belg, 2022; 85(3); 527-30
9.. Ooms H, De Schepper HU, Moreels TG, Case series of cryptogenic multifocal ulcerating stenosing enteritis (CMUSE): Acta Gastroenterol Belg, 2017; 80(3); 361-64
10.. Kohoutova D, Bartova J, Tacheci I, Cryptogenic multifocal ulcerous stenosing enteritis: A review of the literature: Gastroenterol Res Pract, 2013; 2013; 918031
11.. Cullis JO, Fitzsimons EJ, Griffiths WJ, Investigation and management of a raised serum ferritin: Br J Haematol, 2018; 181(3); 331-40
12.. Dolinger M, Torres J, Vermeire S, Crohn’s disease: Lancet, 2024; 403(10432); 1177-91
13.. Chung SH, Park SU, Cheon JH, Clinical characteristics and treatment outcomes of cryptogenic multifocal ulcerous stenosing enteritis in Korea: Dig Dis Sci, 2015; 60(9); 2740-45
14.. Perlemuter G, Guillevin L, Legman P, Cryptogenetic multifocal ulcerous stenosing enteritis: An atypical type of vasculitis or a disease mimicking vasculitis: Gut, 2001; 48(3); 333-38
15.. Osman KT, Maselli DB, Mounajjed TM, Grotz TE, Can cryptogenic multifocal ulcerous stenosing enteritis (CMUSE) be diagnosed in a patient with non-steroidal anti-inflammatory drug exposure?: BMJ Case Rep, 2021; 14(2); e238160
16.. Limsrivilai J, Pausawasdi N, Intestinal tuberculosis or Crohn’s disease: A review of the diagnostic models designed to differentiate between these two gastrointestinal diseases: Intest Res, 2021; 19(1); 21-32
17.. Soysal A, Bakir M, T-SPOT.TB assay usage in adults and children: Expert Rev Mol Diagn, 2011; 11(6); 643-60
18.. Umeno J, Hisamatsu T, Esaki M, A hereditary enteropathy caused by mutations in the SLCO2A1 gene, encoding a prostaglandin transporter: PLoS Genet, 2015; 11(11); e1005581
19.. Brooke MA, Longhurst HJ, Plagnol V, Cryptogenic multifocal ulcerating stenosing enteritis associated with homozygous deletion mutations in cytosolic phospholipase A2-alpha: Gut, 2014; 63(1); 96-104
20.. Yan P, Li K, Cao Y, What is the appropriate treatment strategy for cryptogenic multifocal ulcerative stenosing enteritis? A single-center experience from China: Front Med (Lausanne), 2022; 9; 926800
21.. De Schepper H, Macken E, Van Marck V, Infliximab induces remission in cryptogenic multifocal ulcerous stenosing enteritis: first case: World J Gastroenterol, 2013; 19(10); 1661-64
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133