31 August 2024: Articles 
Chronic Myeloid Leukemia with a Rare Philadelphia Chromosome Variant Involving Chromosome 16
Challenging differential diagnosis, Diagnostic / therapeutic accidents, Unusual setting of medical care, Adverse events of drug therapy, Rare coexistence of disease or pathology
Salem M. Bahashwan12ABDEF*DOI: 10.12659/AJCR.944641
Am J Case Rep 2024; 25:e944641






Abstract
BACKGROUND: Chronic myeloid leukemia (CML) is a myeloproliferative disorder characterized by the presence of the Philadelphia (Ph) chromosome, which results from the fusion of the translocation of the ABL1 gene from chromosome 9 to the BCR gene located in chromosome 22, forming the BCR-ABL gene on chromosome number 22, which accounts for approximately 95% of CML cases. Complex translocation involving other chromosomes can occur.
CASE REPORT: We present a rare case of CML with a variant Ph chromosome, in which chromosome 16 was involved with the usual translocation. A 34-year-old woman presented with a history of left upper quadrant pain and excessive sweating, with no hepatosplenomegaly on examination. She was found to have leukocytosis, with elevated neutrophils (34 000/mm³), basophils (1460/mm³), and eosinophils (2650/mm³). Karyotyping showed a translocation (16;22) (q24,q11.2), and FISH analysis showed BCR-ABL fusion as a result of (9,22) translocation, with a third chromosome (chromosome 16) involved and fused with chromosome 22, with a different breakpoint, which has never been reported in the literature, affecting the long arm of chromosome 16. The patient was treated with a first-generation tyrosine kinase inhibitor (imatinib) and achieved a deep molecular remission. The repeated FISH analysis confirmed the disappearance of both translocations (9,22) and (16,22).
CONCLUSIONS: The impact of the additional chromosomal aberration in CML is widely heterogeneous, and the outcome is dependent on multiple factors. Larger studies are needed to clarify the outcome in CML with variant Ph chromosomes, as most of the available data come from reported cases.
Keywords: imatinib mesylate, Karyotyping, Leukemia, Myelogenous, Chronic, BCR-ABL Positive, Philadelphia Chromosome, Humans, Female, adult, Translocation, Genetic, Chromosomes, Human, Pair 16, Fusion Proteins, bcr-abl
Introduction
Chronic myeloid leukemia (CML) is a myeloproliferative disorder characterized by the presence of the Philadelphia (Ph) chromosome, which results from the fusion of the translocation of the ABL1 gene from chromosome 9 to the BCR gene located in chromosome 22, resulting in the BCR-ABL gene on chromosome number 22 [1]. This reciprocal t(9;22) accounts for around 95% of CML cases. In a minority of cases, complex translocation involving other chromosomes in addition to chromosomes 9 and 22 can occur [2,3].
Two previous cases of CML with variant Ph chromosome in which chromosome 16 was involved were reported, and the short arm of chromosome 16 was affected in both cases (16 p13) [4,5].
Here, we report and discuss a rare case of CML with a variant of the Ph chromosome, in which chromosome 16 was involved with the usual translocation of chromosomes 9 and 22. This is the first case in which the breakpoint on chromo-some 16 is different and the long arm of chromosome 16 is affected (16 q24).
Case Report
A 34-year-old woman, known to have hypertension, presented in 2019 with a history of progressive left upper quadrant abdominal pain over a couple of days and with a long-term history of excessive sweating over the last year. There was no history of fever or weight loss, or other remarkable concerns.
On physical examination, tenderness without rigidity was found over the left upper quadrant area, with no palpable hepatomegaly or splenomegaly. Physical examinations of the central nervous system, respiratory system, and cardiovascular system were normal.
Abdominal ultrasound was done and showed no hepatosplenomegaly, with no focal lesions.
The cause of this left upper quadrant pain was unidentified by physical examination and imaging.
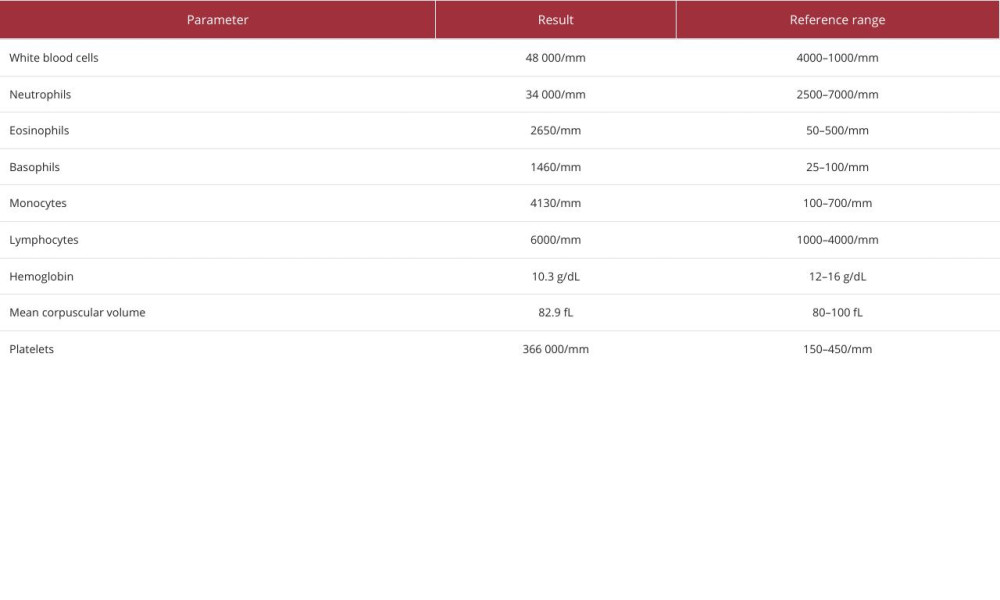
The laboratory examination (Table 1) showed a white blood cell count of 48 000/mm3 (reference range: 4000–1000/mm3), with elevated neutrophil count of 34 000/mm3, basophil count of 1460/mm3, eosinophil count of 2650/mm3, and monocyte count of 4130/mm3. The lymphocyte count was 6000/mm³, hemoglobin level was 10.3 g/dL, mean corpuscular volume was 82.9, and platelet count was 366 000/mm3. Peripheral blood film showed only left shifting with no abnormal cells. There was no family history of hematological malignancy or similar clinical picture.
We used the European Treatment and Outcome Study (EUTOS) score as a risk stratification score, which is calculated based on the percentage of basophils in the peripheral blood and the spleen size below the costal margin in centimeters. The patient had an EUTOS score of 21, which considered as low risk of not achieving a complete cytogenetic remission by 18 months after treatment initiation [6].
Bone marrow aspiration and biopsy showed hypercellular marrow with less than 5% of blast cells and marked granulocytic hyperplasia with variable stages of maturation (Figure 1). Megakaryocytes were significantly increased, and reticulin fibrosis was mildly increased. Findings were consistent with CML in the chronic phase.
Karyotyping from bone marrow was sent and showed a female karyotype with translocation between the long arm of chromosome 16 at a breakpoint q24 and chromosome 22 at a breakpoint q11.2 (46, XX, t (16;22) (q24; q11.2) [20]) (Figure 2).
Fluorescence in situ hybridization (FISH) analysis was done and showed atypical BCR-ABL fusion of 90% of the cells. The ABL gene showed 3 signals: 2 of them were normal and the third was fused with the BCR gene. On the BCR gene, which is located on chromosome 22, three signals were observed. One signal was normal, one was fused with the BCR gene, and the other was translocated to chromosome 16 (Figure 3).
Qualitative real-time PCR was performed on the ration BCRABL/ABL and was 3.7%.
The patient was started on the first-generation tyrosine kinase inhibitor (TKI) imatinib mesylate at a dose of 400 mg daily. The treatment was well tolerated, and the patient achieved a complete hematological remission by 3 months after the initiation of imatinib. By 6 months, karyotyping and FISH analysis from peripheral blood were normal, and the patient achieved a major molecular response by 12 months, when quantitative PCR showed undetectable BCR-ABL translocation. The patient continued to have a major molecular response 5 years after treatment initiation.
Consent was taken from the patient to publish this case.
Discussion
This case represents and describes a rare case of CML with a variant Ph chromosome translocation involving chromo-some 16. The breakpoint observed in this case affected the long arm of chromosome 16, which has never been reported in the literature.
Additional chromosomal abnormalities are found in less than 5% of the newly diagnosed cases of CML with variant Ph chromosome, and the risk of getting an additional chromosomal abnormality during the course of the disease rises and can reach to approximately 80% in the blast crisis phase [7,8].
The impact of the additional chromosomal abnormalities in CML cases with variant Ph chromosome is not well recognized and could be dependent on multiple factors, such as the type of the chromosomal abnormality and the time of the appearance of this abnormality. Additional chromosomal abnormalities developed during the course of the disease are thought to be associated with a worse outcome [7–10].
Different prognostic scores are used for assessing the risk of progression and survival in CML, and the most recent and accurate method is the EUTOS score, which was developed after the era of TKI and showed higher accuracy in predicting survival in a real world clinical setting, as other scores were developed before the era of TKI [11].
The accuracy of diagnosis in CML has significantly improved in the past decade, and FISH has played an important role in the detection of the chromosomal rearrangement and can sometimes detect chromosomal rearrangement not seen or detected by karyotyping, especially if the number of metaphase is insufficient in karyotyping [12,13].
Limited evidence is available in the literature regarding the efficacy of the first generation TKI on CML with variant Ph chromosome. Some investigations showed a lower response rate to imatinib [9,14]. Other studies showed a similar outcome in those with variant Ph chromosome treated with imatinib as in those with standard translocation. Based on the available evidence in the literature [15,16], the European Leukemia Net classified the presence of an additional chromosomal abnormalities at the time of diagnosis as a warning sign [17]. The appearance of the additional chromosomal abnormalities during the course of the treatment is related to the development of imatinib resistance and failure and is associated with a poor outcome [18].
A large observational study including 1151 patients with CML showed that, for those patients with variant Ph chromosome with an additional minor route chromosomal aberration, the chromosomal abnormalities could disappear with imatinib [7], which was concurrent with the present reported case.
Over the last decade, second- and third-generation TKIs were introduced and showed great efficacy in treating CML, especially in those patients with resistance or intolerance to prior TKIs. They were then incorporated in the recommendation as a first-line treatment for the group of patients with high-risk disease progression and transformation, including those with additional chromosomal aberration [19].
Newly emerged and approved treatment by the FDA to treat relapsed and resistant cases of CML with asciminib could be a good alternative to the TKIs, as it acts differently as an allosteric inhibitor of BCR-ABL1 kinase; however, trials are needed to prove the efficacy [20].
Conclusions
The impact of the additional chromosomal aberration in CML is widely heterogeneous, and the outcome is dependent on multiple factors. Multiple studies have been conducted and describe some of the additional chromosomal aberration associated with CML, such as t(1;9;22;16)(q32;q34.1;q11.2;p13), t(9;22;1;13)(q34.1;q11.2;p12;q34), t(9;22;4)(q34.1;q11.2;p16), and t(9;22;7)(q34.1;q11.2;p22). The outcomes of these studies were either similar to CML with the Ph chromosome with no other additional chromosomal aberration or were associated with a poor outcome [21,22]. Additional research is needed to clarify the outcome in CML with variant Ph chromosomes, as most of the data come from reported cases.
Figures
References:
1.. Morris CM, Chronic myeloid leukemia: Cytogenetic methods and applications for diagnosis and treatment: Methods Mol Biol, 2011; 730; 33-61
2.. Naumann S, Decker H-J, Genesis of variant philadelphia chromosome translocations in chronic myelocytic leukemia: Cancer Genet Cytogenet, 2003; 147(1); 18-22
3.. Asif M, Hussain A, Wali A, A rare case of three-way complex variant translocation in chronic myeloid leukemia t(6;9;22)(p21;q34;q11): A case report: Biomed Rep, 2017; 7(4); 377-79
4.. Shu Y, Yang W, Zhang X, Xu X, Recurrent chronic myeloid leukemia with t (9;22;16) (q34; q11; p13) treated by nilotinib: Medicine (Baltimore), 2018; 97(42); e12875
5.. Espinoza JPM, Cárdenas VJP, Jiménez EAV, A complex translocation (9;22;16)(q34;q11.2;p13) in chronic myelocytic leukemia: Cancer Genet Cytogenet, 2005; 157(2); 175-77
6.. Hasford J, Baccarani M, Hoffmann V, Predicting complete cytogenetic response and subsequent progression-free survival in 2060 patients with CML on imatinib treatment: the EUTOS score: Blood, 2011; 118(3); 686-92
7.. Fabarius A, Leitner A, Hochhaus A, Impact of additional cytogenetic aberrations at diagnosis on prognosis of CML: Long-term observation of 1151 patients from the randomized CML Study IV: Blood, 2011; 118(26); 6760-68
8.. Luatti S, Castagnetti F, Marzocchi G, A GIMEMA Working Party on CML analysis: Blood, 2012; 120(4); 761-67
9.. Lussana F, Intermesoli T, Stefanoni P, Rambaldi A, Mechanisms of resistance to targeted therapies in chronic myeloid leukemia: Handb Exp Pharmacol, 2018; 249; 231-50
10.. Bakshi SR, Patel BP, Brahmbhatt MM, Complex karyotype with a masked Philadelphia translocation and variant BCR-ABL fusion in CML: Cancer Genet Cytogenet, 2009; 189(2); 142-43
11.. Sato E, Iriyama N, Tokuhira M, The EUTOS long-term survival score predicts disease-specific mortality and molecular responses among patients with chronic myeloid leukemia in a practice-based cohort: Cancer Med, 2020; 9(23); 8931-39
12.. Amare P, Baisane C, Saikia T, Fluorescence in situ hybridization: Cancer Genet Cytogenet, 2001; 131(2); 125-34
13.. Rack KA, van den Berg E, Haferlach C, European recommendations and quality assurance for cytogenomic analysis of haematological neoplasms: Leukemia, 2019; 33(8); 1851-67
14.. El-Zimaity MMT, Kantarjian H, Talpaz M, Results of imatinib mesylate therapy in chronic myelogenous leukaemia with variant Philadelphia chromosome: Br J Haematol, 2004; 125(2); 187-95
15.. Marzocchi G, Castagnetti F, Luatti S, Variant Philadelphia translocations: Molecular-cytogenetic characterization and prognostic influence on frontline imatinib therapy, a GIMEMA Working Party on CML analysis: Blood, 2011; 117(25); 6793-800
16.. Kalmanti L, Saussele S, Lauseker M, Safety and efficacy of imatinib in CML over a period of 10 years: Data from the randomized CML-study IV: Leukemia, 2015; 29(5); 1123-32
17.. Hochhaus A, Baccarani M, Silver RT, European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia: Leukemia, 2020; 34(4); 966-84
18.. O’Brien SG, Guilhot F, Larson RA, Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia: N Engl J Med, 2003; 348(11); 994-1004
19.. Ishikawa M, Iriyama N, Tokuhira M, Potential role for second-generation tyrosine kinase inhibitors in patients with chronic myeloid leukemia harboring additional clonal chromosome abnormalities: A retrospective CML Cooperative Study Group analysis: Oncol Rep, 2019; 42(6); 2836-43
20.. Choi E-J, Asciminib: The first-in-class allosteric inhibitor of BCR: : ABL1 kinase: Blood Res, 2023; 58(S1); S29-S36
21.. Chauffaille M de LLF, Ameida AC, Martinez RM, Silva ASG, Frequency and diversity of variant Philadelphia chromosome in chronic myeloid leukemiapatients: Blood, 2011; 118(21); 4903
22.. Eyüpoğlu D, Bozkurt S, Haznedaroğlu İ, The impact of variant Philadelphia chromosome translocations on the clinical course of chronic myeloid leukemia: Turkish J Hematol, 2016; 33(1); 60-65
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133