21 January 2025: Articles 
Resistant Renovascular Hypertension in Youth: Fibromuscular Dysplasia or Takayasu Arteritis?
Unusual clinical course, Challenging differential diagnosis, Educational Purpose (only if useful for a systematic review or synthesis)
Aneta MichalczewskaDOI: 10.12659/AJCR.945673
Am J Case Rep 2025; 26:e945673






Abstract
BACKGROUND: Arterial hypertension in pediatric patients often presents complex diagnostic and therapeutic challenges. The diagnosis of hypertension in children is based on different guidelines than in adults, with arterial hypertension in children defined as systolic and/or diastolic blood pressure values at or above the 95th percentile for age, sex, and height. Unlike adult populations, it is predominantly secondary in etiology, with conditions such as renovascular hypertension as common causes. Fibromuscular dysplasia and Takayasu arteritis are frequent underlying causes of renal artery stenosis associated with this patient population.
CASE REPORT: This case report details the successful management of a 15-year-old girl with severe symptomatic hypertension. Plasma renin and aldosterone concentration analysis, Doppler ultrasonography, and angiography were crucial in assessing the severity and nature of the renal stenosis, leading to a diagnosis of renovascular hypertension associated with fibromuscular dysplasia. The patient underwent 2 successful percutaneous transluminal renal angioplasties, achieving blood pressure control without the need for long-term pharmacological therapy.
CONCLUSIONS: In children with elevated blood pressure, secondary hypertension should always be considered and investigated. The diagnosis of renal artery stenosis necessitates a multidisciplinary approach, combining laboratory tests and invasive and non-invasive imaging techniques. Ultrasound is often insufficient for comprehensive and detailed imaging of the renal arteries, being susceptible to error. Careful and comprehensive management of similar cases in specialized centers is essential for ensuring optimal patient care.
Keywords: Hypertension, Renovascular, Hyperaldosteronism, Fibromuscular Dysplasia, Angioplasty, Balloon
Introduction
Renovascular hypertension (RVH) is an important cause of secondary hypertension in children, accounting for approximately 10% of cases [1,2]. It is characterized by elevated blood pressure, typically as a result of renal artery stenosis. Renovascular hypertension and renal artery stenosis in children, unlike in adults, usually are caused by congenital blood vessel malformations and abnormalities, as well as inflammatory causes, with other non-inflammatory processes being less common [3]. However, during adolescence, the proportion of cases of this generally rare disease changes and becomes more similar to that in adults. The obstruction leads to reduced renal perfusion, initiating a cascade of responses, including activation of the renin-angiotensin-aldosterone system (RAAS). The excessive activation of RAAS creates an increase in the production of aldosterone, which plays a crucial role not only in sodium retention and volume expansion but also in enhancing sympathetic outflow and thus exacerbating hypertension [4,5].
Patients with RVH typically present with resistant hypertension, defined as blood pressure that remains above the target despite the concurrent use of at least 3 antihypertensive agents of different classes at maximally tolerated doses, necessitating a tailored approach [6]. Diagnosing renovascular hypertension in children is often significantly delayed due to infrequent blood pressure monitoring and the common assumption that elevated readings are inaccurate rather than being signs of underlying pathology [3]. The diagnosis is further complicated by the nonspecific nature of findings and the variability of clinical manifestations.
Given the significant risk of complications associated with unrecognized renovascular hypertension, as well as secondary hyperaldosteronism, understanding the nuances of those conditions is crucial. In this case report we present the diagnostic journey and therapeutic management of a patient presenting with these interlinked pathologies, highlighting the challenges and strategies in achieving optimal blood pressure control and mitigating the risk of complications. We stress the necessity for heightened clinical vigilance and appropriate diagnosis and management of secondary hypertension.
Case Report
A 15-year-old girl with a 2-year history of headaches, presented a recent episode of nausea and vomiting lasting several days. Her blood pressure was taken and was up to 170/120 mmHg, and she was admitted to the hospital. She has a history of regular follow-ups with an endocrinologist due to benign thyroid nodules and suspicion of post-contrast-induced thyroiditis and was euthyroid at presentation. Apart from that, her medical history was unremarkable, with no indications of other medical conditions or signs suggestive of syndromic or autoimmune diseases.
She was a child from a second uncomplicated pregnancy, a second spontaneous delivery at the 38th week of gestation, with a birth weight of 3500 g. Her development was normal and her puberty status according to the Tanner scale was P5 M5. Her mother was normotensive but had papillary thyroid cancer detected at age 35 and treated with a total thyroidectomy, and also had recurrent hemorrhagic cystitis. Her father has been overweight and hypertensive since the age of about 40, and her older sister had thyroid nodules.
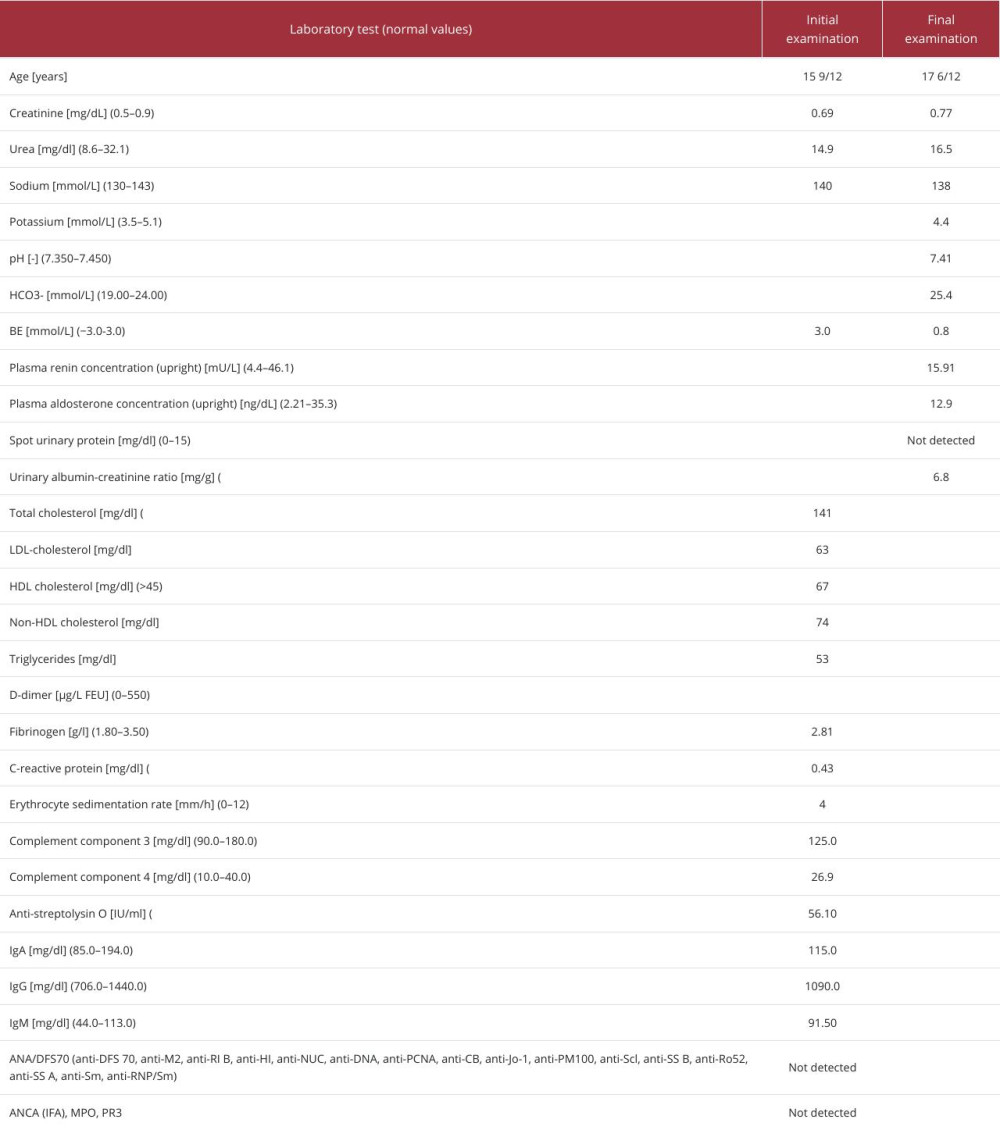
On admission, she was in good general condition. A physical examination showed no significant abnormalities, her height was 169 cm, and her weight was 57.5 kg. Her initial blood pressure was 170/120 mmHg. An assessment of hypertensive organ damage was conducted according to the European Society of Hypertension guidelines [7]. The laboratory evaluation revealed normal kidney function, normal serum sodium concentration, hypokalemia, metabolic alkalosis, and mild proteinuria. Inflammatory parameters were unremarkable (Table 1). Additionally, ophthalmoscopic examination showed myopia, with fundoscopy consistent with elevated blood pressure. Echocardiography showed no left ventricular hypertrophy, with left ventricular mass indexation of 27.7 g/m2 [7].
The patient was initially treated with a combination of amlodipine (10 mg/24 h) and doxazosin (4 mg/24 h) for blood pressure control and potassium supplementation (up to 72 mmol/24 h). Due to persistent hypertension, metoprolol (50 mg/24 h) was added.
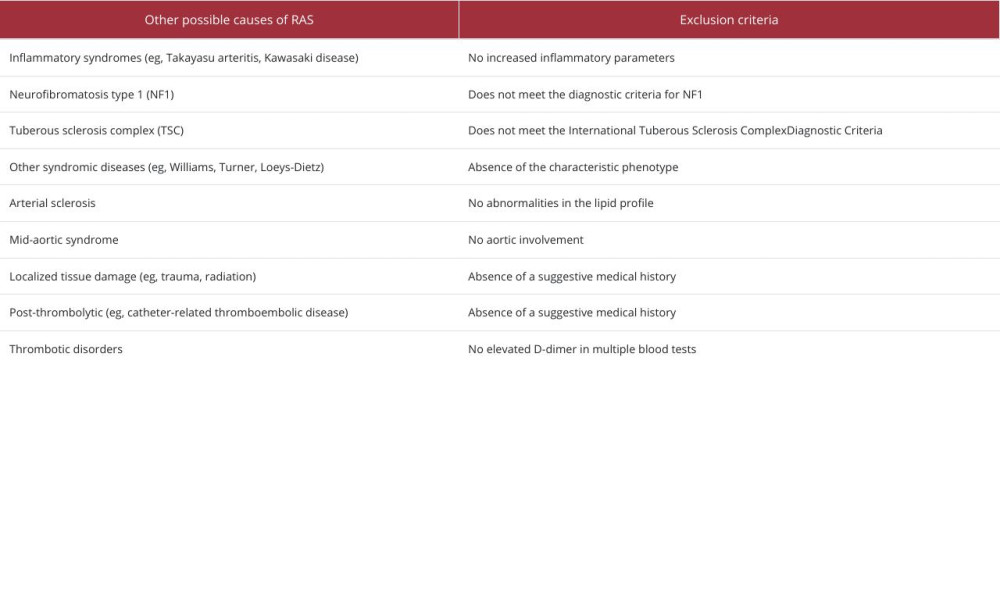
Hormonal testing was performed to investigate the etiology of hypertension and hypokalemia, demonstrating significantly elevated aldosterone and plasma renin concentrations (Table 1). Doppler ultrasound visualized typical vascularization of the left kidney with a single renal artery. The right kidney exhibited a dual blood supply with an accessory artery supplying the lower pole. The morphology of the renal arteries at their origin from the aorta and intrarenal blood flow was within normal limits. CT angiography identified a size asymmetry between the kidneys (right kidney: 100 mm, left kidney: 120 mm) and stenosis of the right renal artery (86% of the cross-sectional lumen calculated relative to the vessel proximally), suggestive of fibromuscular dysplasia (FMD). The radiological imaging was not sufficient to distinguish the underlying cause of the stenosis, but the diagnosis of FMD was reinforced by the exclusion of other potential underlying causes of RAS (Table 2). Renal scintigraphy demonstrated a smaller right kidney, with reduced secretory function. The right kidney’s effective renal plasma flow (ERPF) was markedly reduced at 36%.
Following a multidisciplinary consultation involving radiology and nephrology, the patient’s clinical presentation (including fibromuscular dysplasia, right renal artery stenosis, symptomatic hypertension, and hypokalemia) was determined to be most consistent with a diagnosis necessitating renal angioplasty.
Digital subtraction angiography (DSA) identified a critical stenosis of the right renal artery at its ostium and an arteriovenous fistula (AVF) in the region of the lower pole of the kidney supplied by this vessel. The AVF was occluded from the venous side using 3 platinum coils. The main renal artery trunk and the branch supplying the lower pole remained patent. Balloon angioplasty was performed using two 2×60 mm and 3×20 mm high-pressure balloons. Very good morphological and hemodynamic results were obtained in the stenotic artery (Figure 1).
Following the intervention, the dosage of antihypertensive medications and potassium supplementation was successfully reduced to amlodipine (7.5 mg/24 h) and potassium supplementation (up to 18 mmol/24 h). This resulted in the gradual normalization of acid-base balance, with the maintenance of potassium levels within the normal range on supplementation, and sustained satisfactory blood pressure control.
One year after angioplasty, the patient’s blood pressure remained well-controlled. However, follow-up Doppler ultrasound revealed concerning findings: hemodynamically significant stenosis of the middle-distal segment of the right renal artery with reduced renal resistive index (RI) and possible stenosis of the left renal artery, increased acceleration time in the segmental arterioles, and a “tardus parvus” flow pattern. In the follow-up renal scintigraphy, compared to the previous examination, the secretory and excretory functions of the left kidney were similar, and the secretory and excretory functions of the right kidney had improved. ERPF of the kidneys was measured – the left kidney was 59%, and the right kidney was 41%.
A multidisciplinary team of nephrologists and radiologists recommended repeated renal angiography. Bilateral DSA of the renal arteries revealed significant stenosis of the right renal artery at the level of the first segment, while the left renal artery showed no signs of stenosis. A 2-session percutaneous transluminal renal angioplasty (PTRA) was performed using a combination of 3×40 mm and 5×20 mm balloons, achieving excellent morphological and hemodynamic results (Figure 2).
Given the repeat renal artery balloon angioplasty, it was necessary to consider anticoagulant treatment. Following consultations with centers highly specialized in RAS, including Great Ormond Street Hospital in London and Cardinal Stefan Wyszynski Institute of Cardiology in Warsaw, it was decided to initiate the regimen of acetylsalicylic acid (aspirin) for 6 months for extended thromboembolic prophylaxis, in addition to the postoperative prophylaxis with unfractionated heparin.
Despite a mid-distal segment stenosis to a diameter of approximately 1.2 mm at the narrowest point identified by Doppler ultrasound in the right renal artery, both kidneys maintained normal renal resistive index (RI) values. No signs of stenosis were detected in the left renal artery. The patient is currently not on any antihypertensive medications. Laboratory tests showed renin and aldosterone within the reference range and no proteinuria (Table 1). Follow-up funduscopic examination results were within the normal range, without hypertensive angiopathy.
Evaluation for extra-renal FMD, specifically craniocervical arteries, aorta, and mesenteric and coronary arteries (the echocardiography result did not suggest, and catheter-based angiography of coronary arteries was not performed), revealed no abnormalities, suggesting a unifocal type of the disease. The patient attends regular follow-up visits in the department.
Discussion
This case shows a successful endovascular intervention for a teenage patient with resistant arterial hypertension. Secondary hypertension should always be considered in a child with hypertension; therefore, possible secondary causes must be definitely excluded [7,8]. Arterial hypertension is defined as systolic and/or diastolic blood pressure that is ≥95th percentile for age, sex, and height. Crucially, target blood pressure in children is lower than in adults; therefore, it is essential not to use the universal adult target values for assessing children. RVH in pediatric populations poses unique diagnostic and therapeutic challenges that extend beyond the primary identification of elevated blood pressure.
The diagnostic evaluation of suspected RVH, as illustrated in this case, underscores the importance of employing a wide variety of diagnostic methods. Plasma renin activity is considered one of the crucial screening tests for RVH, with a sensitivity of 80–89% [9,10]. For our patient, the hormonal assays proved instrumental in the initial diagnostics, being able to reveal elevated aldosterone and plasma renin activity. That indicated hyperactivation of the RAAS suggested RVH as a potential underlying cause of hypertension. Ultrasound, while a valuable diagnostic tool, can have limitations in detecting certain types of renal artery stenosis, as demonstrated in this case. The diagnostic process subsequently incorporated Doppler ultrasound, an essential tool for assessing the function and condition of the renal arteries and intrarenal vessels. Crucially, our patient, initially failed to reveal any indications of RVH, which is reflective of its reported sensitivity of only 73–85% [11]. Detailed anatomical visualization was made possible through computed tomography angiography (CTA), which provided more accurate information about the stenosis of the renal artery. Digital subtraction angiography (DSA) was employed as the criterion standard for diagnosing RVH. The diagnostic phase, crucial for accurately identifying and evaluating RVH, is essential for the effectiveness of subsequent therapy.
Takayasu arteritis, the second most common cause of RVH in children, should be considered in all cases of suspected RAS. In our patient, the differential diagnosis was supported by unremarkable inflammatory parameters, as shown in Table 1. In such cases, laboratory evaluation can be instrumental in differentiating between potential causes like Takayasu arteritis and RAS, or even in identifying other, rare clinical conditions.
The arteriovenous fistula (AVF) identified in our patient could also be considered a potential underlying cause of renal artery disease associated with renovascular hypertension. Patients with arteriovenous fistulae develop hypertension due to the formation of a shunt, resulting in local kidney ischemia. AVF can be congenital, but it often arises from percutaneous renal biopsy, penetrating trauma, surgery, malignancy, or inflammation. In our patient, AVF was likely associated with renal FMD, which is a potential cause [7].
The comprehensive clinical presentation, radiological findings, and differential diagnostic considerations outlined in Table 2 facilitated the diagnosis of a unifocal form of FMD in our patient. This form is more prevalent in pediatric patients and is often associated with more severe hypertension at a younger age [12].
Pharmacological treatment is mostly used for the initial stabilization of blood pressure, which in children is often elevated despite the use of multiple antihypertensive drugs [3,13]. Crucially, in patients with suspected bilateral RVH, medications that block the RAAS, such as angiotensin-converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs), are contraindicated due to the risk of severe acute renal failure.
They are effective in unilateral renal artery stenosis but can result in impaired function of the ischemic kidney [3,13].
Invasive treatment for renovascular hypertension in the course of FMD is recommended for all patients, especially those who do not achieve blood pressure control with antihypertensive drugs, have significant adverse effects from this treatment, or have impaired kidney function or ischemic nephropathy [3,15]. Percutaneous transluminal renal angioplasty (PTRA) is the preferred treatment for children with FMD [15,16]. This procedure offers benefits like restoration and preservation of renal perfusion, and polypharmacy reduction. However, restenosis occurs in 27–33% of cases, and branch lesions may require repeat PTRA [17,18], as observed in this case. Stenting is an alternative approach, but it has limitations. Stents themselves can become sites of narrowing as the child grows, long-term outcomes are uncertain, and restenosis rates are higher compared to repeat angioplasty [17,19]. Generally, repeat angioplasty is preferred, as it allows the vessels to naturally remodel to a larger size. However, stents may be useful in specific situations, such as severe or recurrent narrowing, iatrogenic dissections, or vessels that show significant elastic recoil or restenosis after angioplasty. Open surgical revascularization may be a definitive treatment option for patients with renovascular hypertension who are not candidates for minimally invasive approaches.
There is currently no established consensus on the use of anticoagulant therapy in pediatric patients undergoing renal artery angioplasty. In adults, the Polish Society of Hypertension guidelines, as well as recommendations from other international experts, advise prophylactic administration of low-molecular-weight heparin for 1–7 days following PTRA in all cases and continuation of aspirin therapy at a dose of 1 mg/kg body weight/day for an additional 3–6 months [18]. Our center’s experience, informed by available data, supports an individualized and evidence-based treatment approach, carefully considering potential benefits and risks. International Consensus on FMD recommends the use of aspirin in all patients if there are no other medical contraindications. In different centers, various anticoagulation regimens are implemented [21–24].
Percutaneous transluminal renal angioplasty, including a repeat procedure, achieved excellent results in this pediatric patient. Our patient currently has good overall health, with normalized blood pressure and no signs of secondary hyperaldosteronism. Consequently, antihypertensive medications and potassium supplementation are no longer required. We advocate for a multidisciplinary approach in managing similar cases, as collaboration across various medical specialties is essential for comprehensive and effective diagnosis and treatment.
Conclusions
In hypertensive children, especially those who are very young or non-obese, secondary arterial hypertension should always be considered and investigated. Furthermore, appropriate child-specific blood pressure standards should be employed in the evaluation. Diagnosis of RAS in children requires a multimodal approach, frequently utilizing a combination of invasive and non-invasive techniques. FMD, particularly in unifocal form, requires a thorough diagnostic process and the exclusion of other causes of renal artery stenosis in children, including Takayasu arteritis. The significance of plasma renin and aldosterone concentration analysis and non-invasive imaging studies for initial screening cannot be understated. However, non-invasive imaging, such as Doppler ultrasound, could fail to detect lesions, and renal arteriography may be necessary for definitive diagnosis. PTRA should be regarded as the preferred treatment modality in pediatric patients, although multiple procedures are often necessary. Individualized anticoagulation strategies should always be considered for patients undergoing multiple procedures.
Figures
References:
1.. Guzman-Limon M, Samuels J, Pediatric hypertension: Pediatr Clin North Am, 2019; 66(1); 45-57
2.. Wyszyńska T, Cichocka E, Wieteska-Klimczak A, A single pediatric center experience with 1025 children with hypertension: Acta Paediatr, 1992; 81(3); 244-46
3.. Tullus K, Brennan E, Hamilton G, Renovascular hypertension in children: Lancet, 2008; 371(9622); 1453-63
4.. Rossi GP, Bisogni V, Rossitto G, Practice recommendations for diagnosis and treatment of the most common forms of secondary hypertension: High Blood Press Cardiovasc Prev, 2020; 27(6); 547-60
5.. Patel S, Rauf A, Khan H, Abu-Izneid T, Renin-angiotensin-aldosterone (RAAS): The ubiquitous system for homeostasis and pathologies: Biomed Pharmacother, 2017; 94; 317-25
6.. Judd E, Calhoun DA, Apparent and true resistant hypertension: Definition, prevalence and outcomes: J Hum Hypertens, 2014; 28(8); 463-68
7.. Lurbe E, Agabiti-Rosei E, Cruickshank JK, 2016 European Society of Hypertension guidelines for the management of high blood pressure in children and adolescents: J Hypertens, 2016; 34(10); 1887-920
8.. Persu A, Canning C, Prejbisz A, Beyond atherosclerosis and fibromuscular dysplasia: Rare causes of renovascular hypertension: Hypertension, 2021; 78(4); 898-911
9.. Saida K, Kamei K, Hamada R, A simple, refined approach to diagnosing renovascular hypertension in children: A 10-year study: Pediatr Int, 2020; 62(8); 937-43
10.. Kutkuhn B, Kaup FG, Torsello G, Grabensee B, [Captopril-stimulated plasma renin activity in the diagnosis of renovascular hypertension.]: Dtsch Med Wochenschr, 2008; 113(18); 719-24 [in German]
11.. Tullus K, Roebuck DJ, McLaren CA, Marks SD, Imaging in the evaluation of renovascular disease: Pediatr Nephrol, 2010; 25(6); 1049-56
12.. Savard S, Steichen O, Azarine A, Association between 2 angiographic subtypes of renal artery fibromuscular dysplasia and clinical characteristics: Circulation, 2012; 126(25); 3062-69
13.. Lobeck IN, Alhajjat AM, Dupree P, The management of pediatric renovascular hypertension: A single center experience and review of the literature: J Pediatr Surg, 2018; 53(9); 1825-31
14.. Meyers KE, Cahill AM, Sethna C, Interventions for pediatric renovascular hypertension: Curr Hypertens Rep, 2014; 16(4); 422
15.. Gottsater A, Lindblad B, Optimal management of renal artery fibromuscular dysplasia: Ther Clin Risk Manag, 2014; 10; 583-95
16.. Patel PA, Cahill AM, Renovascular hypertension in children: CVIR Endovasc, 2021; 4(1); 10
17.. Shroff R, Roebuck DJ, Gordon I, Angioplasty for renovascular hypertension in children: 20-year experience: Pediatrics, 2006; 118(1); 268-75
18.. Courtel JV, Soto B, Niaudet P, Percutaneous transluminal angioplasty of renal artery stenosis in children: Pediatr Radiol, 1998; 28(1); 59-63
19.. Kari JA, Roebuck DJ, McLaren CA, Angioplasty for renovascular hypertension in 78 children: Arch Dis Child, 2015; 100(5); 474-78
20.. Tykarski A, Filipiak KJ, Januszewicz A, Polish Hypertension Society guidelines for the management of arterial hypertension – 2019 [Internet]. Available from: www.ntwp.viamedica.pl
21.. Šimunić S, Winter-Fudurić I, Radanović B, Percutaneous transluminal renal angioplasty (PTRA) as a method of therapy for renovascular hypertension in children.: Eur J Radiol, 1990; 10(2); 143-46
22.. Bayrak H, Numan F, Cantasdemir M, Ban A, Percutaneous balloon angioplasty of renovascular hypertension in pediatric cases: Acta Chir Belg, 2008; 108(6); 708-14
23.. Chen Y, Dong H, Jiang X, Percutaneous transluminal angioplasty with selective stenting for the treatment of renal artery stenosis caused by fibromuscular dysplasia: 18 years’ experience from the China Center for Cardiovascular Disease: Catheter Cardiovas Interv, 2020; 95(Suppl. 1); 641-47
24.. Yang X, Li P, Zhang B, Outcomes of percutaneous transluminal renal angioplasty for pediatric renovascular hypertension: A 12-year retrospective single-center experience.: Transl Pediatr, 2023; 12(8); 1454-63
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133