19 May 2025: Articles 
Single-Incision Laparoscopic Cholecystectomy in Situs Inversus Totalis: A Case Report
Rare disease
Zhi Li ABCDEF 1, Yonghao Ouyang BDF 1, Kai DingDOI: 10.12659/AJCR.946523
Am J Case Rep 2025; 26:e946523






Abstract
BACKGROUND: Situs inversus totalis (SIT) is a rare developmental anomaly. For many years, laparoscopic cholecystectomy has been a well-established and effective treatment for patients with cholecystolithiasis. However, when it comes to SIT patients with cholecystolithiasis, this surgery presents unique challenges. Due to its complete mirror inversion of viscera, it is uncomfortable to carry out standard laparoscopic cholecystectomy for some surgeons. Single-incision laparoscopic cholecystectomy (SILC) offers a minimally invasive alternative to traditional laparoscopic cholecystectomy, potentially enhancing aesthetic outcomes and minimizing postoperative discomfort.
CASE REPORT: A 67-year-old woman was admitted to the hospital due to abdominal pain. After admission, she completed a chest X-ray, electrocardiogram, B-ultrasound, and magnetic resonance cholangiopancreatography. Imaging examination revealed SIT and cholecystolithiasis. The laboratory examination results were normal. All contraindications to surgery were ruled out, and then SILC was performed under general anesthesia on January 22, 2024. The surgeon and assistant stood on the right side of the patient, and the abdominal SILC port with 3 operation channels was placed through a 2-cm traumatic incision. We used electric hooks and separating forceps to dissect the Calot triangle and gallbladder of the patient, and the gallbladder was successfully removed. The patient recovered well after the surgery.
CONCLUSIONS: For SIT patients with cholecystolithiasis, SILC is a safe and effective minimally invasive treatment option which has fewer surgical incisions and less postoperative pain. However, it demands experienced SILC surgeons, thorough preoperative examinations, and close attention to incision conditions after surgery.
Keywords: Cholelithiasis, Laparoscopy, Situs Inversus, Humans, Female, Aged, Cholecystectomy, Laparoscopic, Cholecystolithiasis
Introduction
Situs inversus totalis (SIT) is a rare developmental condition. It can be identified by the symmetrical reversal of organs in both the thorax and abdomen. This represents a comprehensive failure in the typical lateral orientation, leading to an array of laterality issues due to the absence of normal left-right asymmetry [1]. Interestingly, a study has uncovered that SIT may be associated with malignant ovarian germ cell tumors [2]. Furthermore, it might be accompanied by various other notable congenital abnormalities, including kidney dysplasia, pancreatic fibrosis, abnormal intrahepatic bile duct development and others [3]. Such rare cases typically present challenges during diagnosis and treatment, for doctors. Even the most experienced medical professionals, such as gastroenterologists, radiologists, and surgeons, may encounter these cases only a few times throughout their careers [4,5].
Cholecystectomy is the best choice for treating cholecystolithiasis. Compared with conventional laparotomy, laparoscopic cholecystectomy is favored for its minimally invasive, less painful, and faster recovery characteristics. Previous studies have shown that laparoscopic cholecystectomy is safe and effective for patients with cholecystolithiasis and SIT [6,7]. In recent years, with the continuous advancement of laparoscopic technology and the improvement of surgical skills, single-incision laparoscopic cholecystectomy (SILC) has gradually become popular. SILC not only inherits the advantages of laparoscopic cholecystectomy, but also excels in incision aesthetics and postoperative pain management [8,9].
Cases of SIT patients with cholecystolithiasis are extremely rare. Our primary objective was to present this extraordinary case and share the results as well as our experiences regarding the surgical technique employed. Moreover, we aimed to further reduce postoperative pain, enhance the aesthetic appearance of the incision, and verify the clinical application value of SILC in SIT patients with cholecystolithiasis. With the patient’s consent obtained, SILC was thus utilized to treat this particular patient.
Case Report
SURGICAL APPROACH:
After excluding the contraindications for surgery and signing the informed consent, the patient underwent SILC under general anesthesia on January 22, 2024. The patient was placed in the supine position. The surgeon and assistant stood on the right side of the patient, cut about 2 cm horizontally from the umbilicus, went into the abdomen layer by layer, and placed single-incision laparoscopic instruments. After creation of a successful pneumoperitoneum, the laparoscope was placed into the abdomen. During the operation, it was confirmed that the gallbladder was located at the lower edge of the left liver. There were adhesions between the gallbladder and surrounding tissues. The gallbladder serosa was opened with an electric hook, the Calot triangle was carefully dissected, and the gallbladder duct and gallbladder artery were separated. The cystic duct and the cystic artery were clipped with Hem-o-lok clips and cut independently. The electric hook peeled the gallbladder, in an anterograde direction, from the Calot triangle to the bottom of the gallbladder. During the operation, some tissues were more inflammatory and adherent, and then we peeled it, in a retrograde direction, from the bottom of the gallbladder to the Calot triangle. After gallbladder resection, the electric hook was used to complete hemostasis. Finally, the gallbladder and instruments were removed, and the abdominal wall incision was sutured. The intraoperative bleeding was about 5 mL. On January 22, 2024, postoperative pathology suggested that the gallbladder stones were accompanied by chronic cholecystitis. The size of the gallbladder was 5.5×3.5×0.6 cm, and the thickness of the gallbladder wall was 0.2 cm (Figure 5A, 5B).
Discussion
SIT is a rare embryonic deformity, in which organs shift from their normal positions to the opposite side of the body. Its incidence is approximately 1 in 10 000. Moreover, it may be accompanied by other significant congenital abnormalities, such as kidney dysplasia, pancreatic fibrosis, and others [3].
For many years, laparoscopic cholecystectomy has been a well-established and effective treatment for patients with cholecystolithiasis. However, when it comes to patients with SIT and cholecystolithiasis, this surgery presents unique challenges. When diagnosing patients with cholecystolithiasis and SIT, a detailed history inquiry and physical examination are of utmost importance. Special attention should be paid to the patient’s physical characteristics and family history to rule out other diseases that might lead to abnormal organ locations. Additionally, imaging examinations play a crucial role in diagnosing SIT. Ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) can assist doctors in clarifying the location and morphology of the gallbladder as well as the surrounding organs. These examinations can also determine whether the patient has SIT or partial situs inversus, thereby facilitating the formulation of an appropriate surgical plan. In this case, we conducted abdominal B-ultrasound, cardiac ultrasound, chest X-ray, electrocardiogram, and MRCP prior to the operation. These tests confirmed that the patient had SIT rather than partial situs inversus or a simple left-sided gallbladder.
Campo reported the first case of laparoscopic cholecystectomy in a patient with SIT in 1991 [10]. Subsequently, several case reports introduced a variety of technical means, such as comprehensive preoperative examination, single-incision surgery, mirror port placement, and referral of cases to left-handed surgeons. Chaouch and other studies [11] have found that for laparoscopic cholecystectomy in SIT patients, there are various surgical techniques, but a lack of standards. “American mirror technology” and “French mirror technology” are common. Right-handed doctors find it difficult to operate on these patients, and special attention is needed to the position of the trocar and the position of the surgeon. Future robotics technology may reduce difficulties. Enciu [12] conducted a meta-analysis of relevant reports in recent years, and they found that although laparoscopic cholecystectomy in SIT is uncomfortable for right-handed surgeons, it is safe and remains the gold standard. Surgeons should prepare in advance for the unfamiliar aspects. Although preoperative imaging and a left-handed surgeon are beneficial in terms of surgery length, when these are not available, surgeons should focus on achieving the most comfortable setting based on their experience and tailor their approach to the patient.
For patients with SIT, whether to choose SILC requires careful consideration of the patient’s specific condition and the doctor’s SILC surgical experience. For the patient reported in this case, the cystic duct and gallbladder dissection in this patient had to be performed in a “mirror image” manner, opposite to normal. In up to 25% of patients, biliary tract abnormalities are present. Considering that the incidence of these abnormalities is similar to that of the normal population, we excluded the patient’s possible biliary tract abnormalities by MRCP before surgery to avoid accidental injury to the patient during surgery. Considering the minimization of the patient’s abdominal incision and the safety of the patient, we chose to perform the SILC.
For patients with SIT, compared with patients undergoing laparoscopic cholecystectomy, SILC has a better incision cosmetic effect. SILC has only 1 incision, and the incision through the umbilical area can achieve nearly scar-free healing by using umbilical folds to cover the surgical scar. In addition to these benefits, the average length of hospital stay and quality of life after the surgery are equivalent to those for patients undergoing laparoscopic cholecystectomy. Moreover, patients undergoing SILC need fewer analgesic drugs to attain a satisfactory analgesic effect [13–15].
However, SILC also has some disadvantages. Intraoperative complications of SILC mainly include biliary tract injury, intraoperative bleeding, gastrointestinal tract injury, and others. Postoperative complications mainly include incision infection, incisional hernia, bile leakage, abdominal cavity bleeding, subphrenic effusion, pleural effusion, pulmonary infection, and others. Some patients may experience delayed bile leakage and abdominal cavity bleeding 1 week after the operation. Most of the complications of SILC are similar to those of laparoscopic cholecystectomy, but the incidence rates of incision infection and incisional hernia may be higher than those of laparoscopic cholecystectomy [15–18].
Conclusions
For SIT patients suffering from cholecystolithiasis, SILC has several advantages, such as fewer surgical incisions, less postoperative pain, and increased ease of postoperative recovery. It is crucial to note that a detailed history inquiry, physical examination, and meticulous preoperative examinations are necessary to exclude possible variations in blood vessels and bile ducts. Moreover, SILC procedures for SIT patients should be performed by experienced surgeons. Additionally, in the postoperative period, close attention needs to be paid to whether there are any signs of infection or herniation at the patient’s incision. In conclusion, this particular case illustrates that SILC is a safe and effective minimally invasive treatment option for SIT patients with cholecystolithiasis.
Figures
 Figure 1. (A–C) Cardiac ultrasound (January 16, 2024) suggested SIT, aortic arteriosclerosis, mild mitral and aortic valve calcification, left ventricular hypodiastolic function, and mild mitral regurgitation.
Figure 1. (A–C) Cardiac ultrasound (January 16, 2024) suggested SIT, aortic arteriosclerosis, mild mitral and aortic valve calcification, left ventricular hypodiastolic function, and mild mitral regurgitation.  Figure 2. (A, B) Abdominal ultrasound performed on January 16, 2024, revealed thickening and irregularity of the gallbladder wall, and multiple strongly echogenic masses were seen in the lumen with posterior acoustic shadows, the larger of which had a long diameter of about 15 mm. The internal diameter of the common bile duct was about 4 mm, and SIT was apparent.
Figure 2. (A, B) Abdominal ultrasound performed on January 16, 2024, revealed thickening and irregularity of the gallbladder wall, and multiple strongly echogenic masses were seen in the lumen with posterior acoustic shadows, the larger of which had a long diameter of about 15 mm. The internal diameter of the common bile duct was about 4 mm, and SIT was apparent. 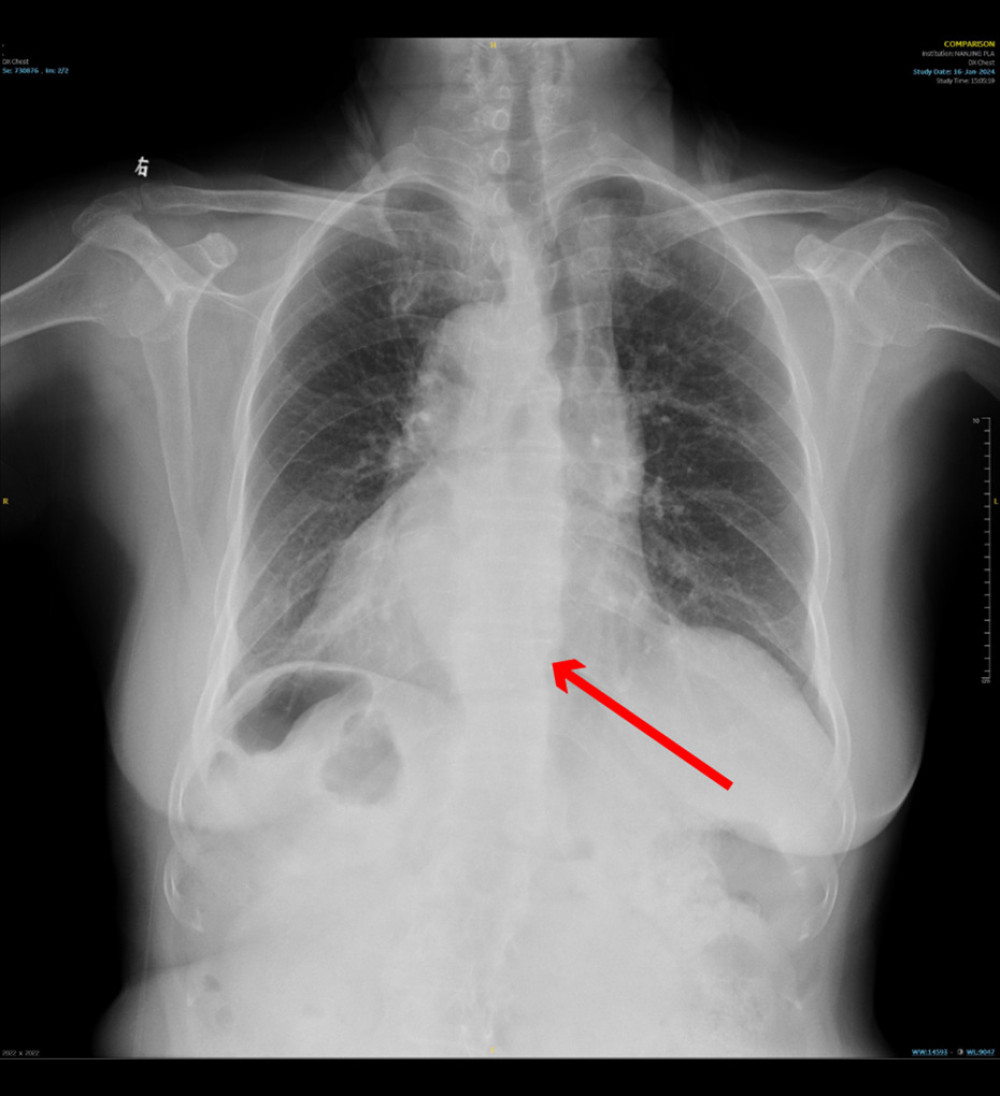 Figure 3. Chest X-ray (January 16, 2024) performed at Jinling Hospital, which is affiliated with Nanjing University, indicated dextrocardia. (The red arrow in the picture refers to the patient’s heart).
Figure 3. Chest X-ray (January 16, 2024) performed at Jinling Hospital, which is affiliated with Nanjing University, indicated dextrocardia. (The red arrow in the picture refers to the patient’s heart). 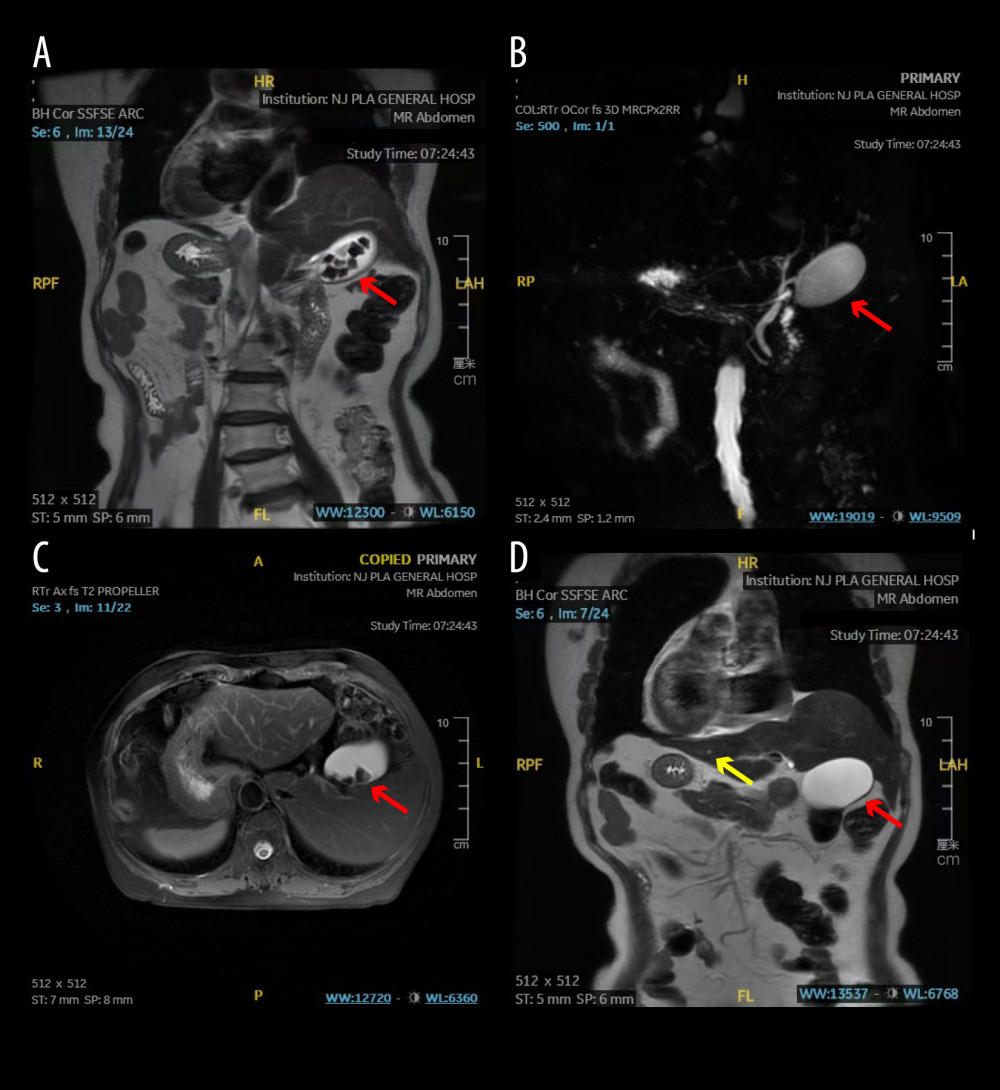 Figure 4. (A–D) MRCP (January 18, 2024) suggested SIT, cholecystolithiasis (the red arrows indicate the patient’s gallbladder), and a 3-mm small hepatic cyst in the right lobe of the liver. (The yellow arrow in Figure D indicates the patient’s hepatic cyst).
Figure 4. (A–D) MRCP (January 18, 2024) suggested SIT, cholecystolithiasis (the red arrows indicate the patient’s gallbladder), and a 3-mm small hepatic cyst in the right lobe of the liver. (The yellow arrow in Figure D indicates the patient’s hepatic cyst). 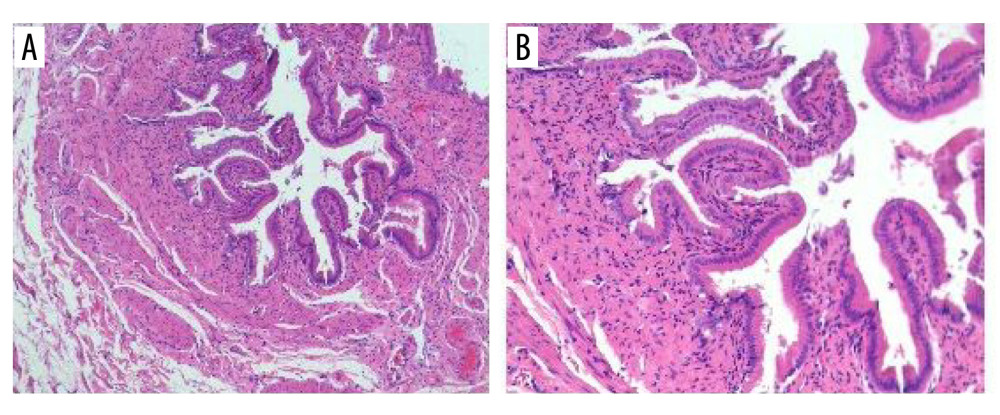 Figure 5. (A, B) Postoperative pathology (January 22, 2024) suggested that the gallbladder stones were accompanied by chronic cholecystitis. The size of the gallbladder was 5.5×3.5×0.6 cm, and the thickness of the gallbladder wall was 0.2 cm.
Figure 5. (A, B) Postoperative pathology (January 22, 2024) suggested that the gallbladder stones were accompanied by chronic cholecystitis. The size of the gallbladder was 5.5×3.5×0.6 cm, and the thickness of the gallbladder wall was 0.2 cm. References
1. Peeters H, Devriendt K, Human laterality disorders: Eur J Med Genet, 2006; 49(5); 349-62
2. Hafez AS, Asar MM, Farid S, Laparoscopic retroperitoneal lymphadenectomy for ovarian mixed germ cell tumor in a patient with situs inversus totalis; Reporting the first case worldwide with literature review and in silico analysis: Pathol Res Pract, 2024; 256; 155228
3. Hiraoka K, Haratake J, Horie A, Miyagawa T, Bilateral renal dysplasia, pancreatic fibrosis, intrahepatic biliary dysgenesis, and situs inversus totalis in a boy: Hum Pathol, 1988; 19(7); 871-73
4. Blegen HM, Surgery in situs inversus: Ann Surg, 1949; 129(2); 244-59
5. Eitler K, Bibok A, Telkes G, Situs inversus totalis: A clinical review: Int J Gen Med, 2022; 15; 2437-49
6. He T, Zou J, Song H, Laparoscopic cholecystectomy in a patient with situs inversus totalis presenting with cholelithiasis: A case report: Front Surg, 2022; 9; 874494
7. Montalvo-Javé EE, Arroyo-Paredes PS, Corona-Torres MJ, Rodríguez-Báez A, Laparoscopic cholecystectomy in a patient with situs inversus totalis: Rev Gastroenterol Mex (Engl Ed), 2022; 87(4); 486-88
8. Jørgensen LN, Rosenberg J, Al-Tayar H, Assaadzadeh S, Randomized clinical trial of single- versus multi-incision laparoscopic cholecystectomy: Br J Surg, 2014; 101(4); 347-55
9. Wang D, Wang Y, Ji ZL, Laparoendoscopic single-site cholecystectomy versus conventional laparoscopic cholecystectomy: A systematic review of randomized controlled trials: ANZ J Surg, 2012; 82(5); 303-10
10. Campos L, Sipes E, Laparoscopic cholecystectomy in a 39-year-old female with situs inversus: J Laparoendosc Surg, 1991; 1(2); 123-25 discussion, 126
11. Chaouch MA, Jerraya H, Dougaz MW, A systematic review of laparoscopic cholecystectomy in situs inversus: J Invest Surg, 2021; 34(3); 324-33
12. Enciu O, Toma EA, Tulin A, Look beyond the mirror: laparoscopic cholecystectomy in situs inversus totalis – a systematic review and meta-analysis (and report of new technique): Diagnostics (Basel), 2022; 12(5); 1265
13. Arezzo A, Passera R, Bullano A, Multi-port versus single-port cholecystectomy: Results of a multi-centre, randomised controlled trial (MUSIC trial): Surg Endosc, 2017; 31(7); 2872-80
14. Guo W, Liu Y, Han W, Randomized trial of immediate postoperative pain following single-incision versus traditional laparoscopic cholecystectomy: Chin Med J (Engl), 2015; 128(24); 3310-16
15. Minimally Invasive Surgery Committee of the Chinese Research Hospital Association, Chinese expert consensus on single-incision laparoscopic cholecystectomy (2024 edition): J Clin Hepatol, 2024; 40(10); 1967-72
16. Haueter R, Schütz T, Raptis DA, Meta-analysis of single-port versus conventional laparoscopic cholecystectomy comparing body image and cosmesis: Br J Surg, 2017; 104(9); 1141-59
17. Ma J, Cassera MA, Spaun GO, S , Randomized controlled trial comparing single-port laparoscopic cholecystectomy and four-port laparoscopic cholecystectomy: Ann Surg, 2011; 254(1); 22-27
18. Merchant AM, Cook MW, White BC, Transumbilical Gelport access technique for performing single incision laparoscopic surgery (SILS): J Gastrointest Surg, 2009; 13(1); 159-62
Figures
Figure 1. (A–C) Cardiac ultrasound (January 16, 2024) suggested SIT, aortic arteriosclerosis, mild mitral and aortic valve calcification, left ventricular hypodiastolic function, and mild mitral regurgitation.Figure 2. (A, B) Abdominal ultrasound performed on January 16, 2024, revealed thickening and irregularity of the gallbladder wall, and multiple strongly echogenic masses were seen in the lumen with posterior acoustic shadows, the larger of which had a long diameter of about 15 mm. The internal diameter of the common bile duct was about 4 mm, and SIT was apparent.Figure 3. Chest X-ray (January 16, 2024) performed at Jinling Hospital, which is affiliated with Nanjing University, indicated dextrocardia. (The red arrow in the picture refers to the patient’s heart).Figure 4. (A–D) MRCP (January 18, 2024) suggested SIT, cholecystolithiasis (the red arrows indicate the patient’s gallbladder), and a 3-mm small hepatic cyst in the right lobe of the liver. (The yellow arrow in Figure D indicates the patient’s hepatic cyst).Figure 5. (A, B) Postoperative pathology (January 22, 2024) suggested that the gallbladder stones were accompanied by chronic cholecystitis. The size of the gallbladder was 5.5×3.5×0.6 cm, and the thickness of the gallbladder wall was 0.2 cm. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133