14 May 2025: Case Reports 
Novel Approach to Retro-Odontoid Pseudotumor Resection without Atlantoaxial Dislocation
Challenging differential diagnosis, Unusual setting of medical care, Rare disease
Jia Shao ABCDEFG 1, Yan Zheng Gao ABCDF 1*, Kun Gao ABCD 1, Ke Zheng Mao BDF 1, Xiu Ru Zhang BCD 1DOI: 10.12659/AJCR.946611
Am J Case Rep 2025; 26:e946611






Abstract
BACKGROUND: Retro-odontoid pseudotumor is a fibrous or pannus mass behind the odontoid process, mainly caused by atlantoaxial instability, degeneration, or abnormal deposits behind the dens. Most scholars agree immobilization of the upper cervical spine can solve this problem; the mass can absorb spontaneously. However, retro-odontoid pseudotumor cases without atlantoaxial instability are limited, and it remains controversial whether the mass should be removed.
CASE REPORT: A 67-year-old man had intermittent neck pain for 10 years and numbness and weakness of the extremities for 1 month. Primary diagnosis was intra-spinal neoplasm (C1), cervical spondylotic myelopathy, and subaxial cervical stenosis. After C3-C7 laminoplasty, we removed the posterior arch of the atlas, and the mass was resected via the lateral side of the spinal cord using a curette and clamp, followed by C1-C2 fixation and bilateral lateral atlantoaxial joint fusion in single stage. The intra-spinal neoplasm was debunked, and a diagnosis of a retro-odontoid pseudotumor was made based on pathology. Postoperative radiography showed sufficient decompression of C3-C7 and sufficient grafted bone in the lateral atlantoaxial joints. The pseudotumor was completely resected, and no compression was seen on MRI. The symptoms resolved immediately after the procedure. The Japanese Orthopaedic Association score was 16, and 1-year follow-up showed no tumor recurrence.
CONCLUSIONS: The retro-odontoid pseudotumor should be removed if there is obvious compression of the spinal cord. Lateral atlantoaxial joint bone grafting is recommended because of the removal of the grafting bed (posterior C1 arch) for posterior fusion. C1-C2 fixation and fusion could reserve the motion of C0-C1.
Keywords: Atlanto-Axial Joint, Hypertrophy, inflammation, Osteoarthritis, Spine, Osteotomy, Humans, Male, Aged, Odontoid Process, Spinal Fusion, Cervical Vertebrae, Granuloma, Plasma Cell, Decompression, Surgical, Magnetic Resonance Imaging
Introduction
Retro-odontoid pseudotumor (ROP) is a fibrous or pannus mass behind the odontoid process, which was first reported by Castor in 1983 based on computed tomography (CT) [1], and by Sze in 1986 based on magnetic resonance imaging (MRI) [2]. Pseudotumors have several pathological types, including rheumatoid pannus, granulation tissue, synovial cyst, migrated intervertebral disc, hypertrophic transverse ligament, amyloid protein deposit, and pseudogout [3–7]. Most scholars agree that immobilization of the upper cervical spine can solve this problem, with the mass absorbing spontaneously [8–11]. However, it remains controversial whether the mass should be removed. The data on ROP cases without atlantoaxial instability is limited, and most studies emphasize posterior fixation for ROP regression [12–14]. However, the present report demonstrates that surgical resection, even in cases without instability, can rapidly relieve spinal cord compression and optimize neurological recovery. The use of lateral atlantoaxial joint grafting to compensate for the removal of the posterior arch can serve as an alternative approach that is rarely discussed in the literature.
Case Report
The patient was a 67-year-old man with intermittent neck pain for 10 years and numbness and weakness of the extremities for 1 month. He had no contributory past history of hypertension, diabetes mellitus, coronary heart disease, or malignant tumor. On examination, superficial sensation decreased below the T4 level, and the muscle strength of the extremities was grade IV. Tendon reflexes were hyperactive, and bilateral Hoffman and Babinski signs were positive. The Japanese Orthopaedic Association (JOA) score was 11, while the visual analog scale (VAS) score of the neck was 4. Dynamic radiography showed no instability of the C-spine. CT sagittal reconstruction revealed cervical degeneration and multiple cysts in the upper C-spine, and the anterior atlanto-dental interval was 1.1 mm. Subaxial cervical stenosis was diagnosed based on the Pavlov ratio in C3–C7 (0.60, 0.53, 0.53, 0.58, and 0.61, respectively), and a giant mass was noticed behind the dens. The mass was hypointense on T1- and T2-weighted MRI, and only the edge was enhanced on contrast-enhanced MRI. The size of the mass was 8.64×20.39 mm in sagittal view of T1-weighted MRI, and the width of the mass was 15.78 mm in transverse view. Erythrocyte sedimentation rate and C-reactive protein levels were in the reference range, and rheumatoid factor and T-Spot tests were negative. Our primary diagnoses were intra-spinal neoplasm (C1), cervical spondylotic myelopathy, and subaxial cervical stenosis (Figure 1).
Surgery was indicated due to compression of the spinal cord, and after C3–C7 laminoplasty, the posterior arch of the atlas was removed in a posterior midline approach with the prone position. The left side of the C2 nerve root was removed to expose the mass, and it was resected via the lateral side of the spinal cord using a curette and clamp. Atlantoaxial fixation was completed using atlas lateral mass screw, axial pedicle screw, and rod, based on the Goel-Harms technique, which has been widely used for C1–C2 fixation, with an excellent biomechanical property. The bilateral lateral atlantoaxial joint surfaces were decorticated and autografted using a granularized iliac crest bone (Figures 2,3). The frozen section result did not reveal any malignancy, and routine histopathology revealed a homogeneous cartilage-like matrix. Intraspinal neoplasm was debunked, and a diagnosis of ROP was made.
Postoperative radiography showed no change of the atlanto-dental interval and sufficient decompression of C3–C7, with the postoperative Pavlov ratio increasing to 0.85, 0.80, 0.84, 0.82, and 0.86, respectively, and CT showed sufficient grafted bone in the lateral atlantoaxial joints. Postoperative MRI showed complete resection of the pseudotumor (Figure 2). The symptoms resolved immediately after the procedure. The JOA score was 16, while the VAS score of neck decreased to 1, and there was no tumor recurrence at the 1-year follow-up.
Discussion
There are 3 types of ROP: type I is caused by C1–C2 instability, such as in os odontoideum, rheumatoid arthritis, and basilar invagination; type II is without C1–C2 instability, and it can be caused by abnormal stress in the transverse ligament, such as in degeneration or disseminated idiopathic skeletal hyperostosis of the upper C-spine; and type III is caused by abnormal deposits behind the dens [15–17].
The surgical treatment of ROP has not been standardized, and whether the ROP should be removed is still controversial. Venteicher et al reported an endoscopic endonasal transodontoid approach to remove the pseudotumor, followed by posterior fixation [18]. Schomacher et al reported a posterior transdural approach for removing the mass, followed by C0–C2 fixation [19]. Naito et al removed cystic pseudotumors using a high cervical lateral approach [20]. Some authors have treated ROPs without removing the mass. Kakutani et al removed the posterior arch of C1 to treat ROP without atlantoaxial instability [21]. Certo et al [22] and Chikuda et al [23] reported the absorption of the mass after C1–C2 or C0–C2 fixation. We reviewed most of the reports on ROP. Most of the masses were removed by neurosurgeons, and most of them did not complete fixation. However, in cases in which the masses were not removed, most of the authors were from orthopedic surgery, and they completed fixation [24,25]. Details of previous reports are listed in Table 1.
The mass can regress over time after fixation, but the timing of regression is still uncertain. Also, prior to its absorption, it continuously compresses the spinal cord, and the recovery rate is inconsistent. Park et al reported a study of 38 cases of ROP, which is the largest case series reported to date. None of the cases underwent resection of the pseudotumor. Although all pseudotumors regressed in size during follow-up, in terms of the recovery rate of the JOA score, the excellent group accounted for 28.1%, the good group accounted for 12.5%, and the excellent-good rate was only 40.6% [10]. While posterior fixation alone can lead to pseudotumor regression, residual spinal cord compression caused by a giant mass could delay neurological recovery. We therefore recommend C1 laminectomy and removal of the pseudotumor followed by C1–C2 instrumentation, if there is obvious compression of the spinal cord. Because the posterior arch of C1, which is commonly used for grafting bed, was removed, lateral atlantoaxial joint bone grafting was a better choice.
This case demonstrates that direct resection, combined with stabilization, offers immediate decompression benefits. The novel use of lateral atlantoaxial joint grafting also preserves C0–C1 motion, a significant advantage over traditional techniques.
To the best of our knowledge, this is the first report of posterior removal and C1–C2 fixation for the treatment of an ROP without atlantoaxial dislocation. This procedure could release the compression of the spinal cord and reserve the motion of C0–C1, compared with previous reports. Our limitation was that one side of the C2 nerve root was not removed, causing numbness or occipital neuralgia; however, this sequela could be relieved spontaneously or by giving greater occipital nerve block.
Conclusions
The ROP should be removed if there is obvious compression of the spinal cord. Lateral atlantoaxial joint bone grafting is recommended because of the removal of the grafting bed (posterior C1 arch) for posterior fusion. C1–C2 fixation and fusion could reserve the motion of C0–C1. This technique can serve as a valuable alternative approach for similar cases of ROP without instability, providing effective decompression and motion preservation.
Figures
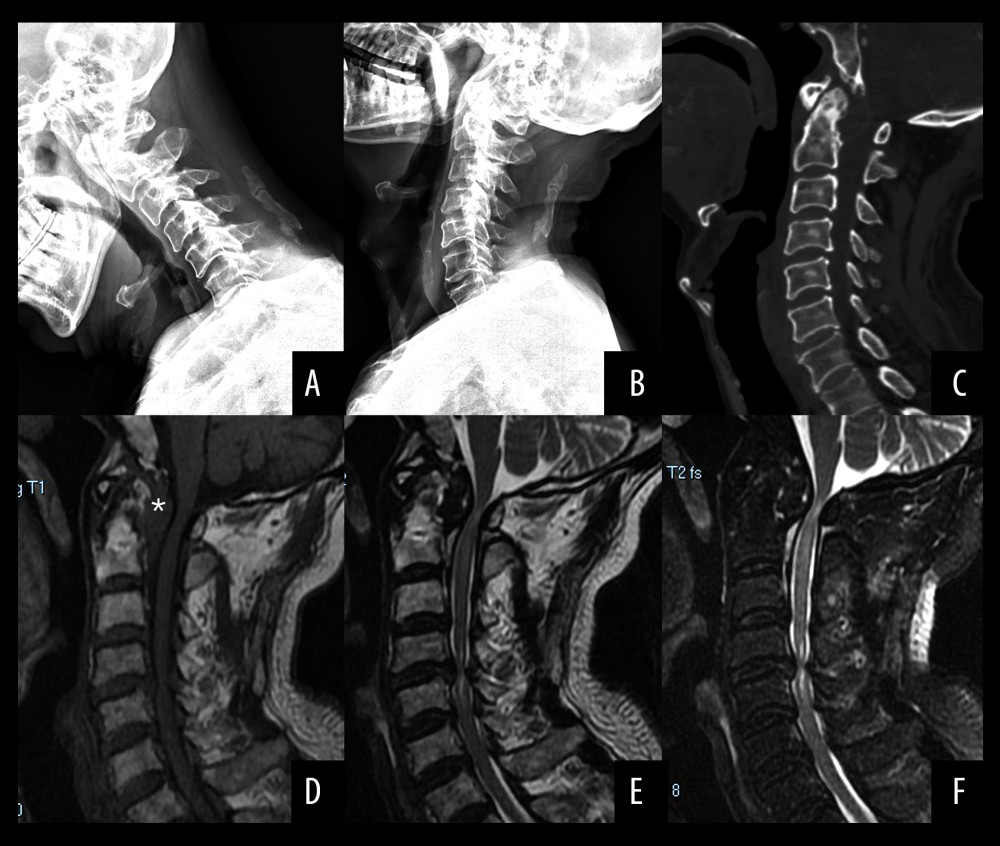 Figure 1. (A, B) Hyper flexion and extension radiographs showed no instability of C1–C2. (C) Sagittal reconstructive computed tomography scan of the cervical spine showed cervical degeneration and multiple cysts in the upper cervical spine. A subaxial cervical stenosis was diagnosed based on the Pavlov ratio in C3–C7. (D, E) A huge mass was noted posterior to the dens. The mass was hypointense on T1- and T2-weighted magnetic resonance imaging (MRI). (F) Only the rim of the pseudotumor was enhanced on T2-weighted contrast-enhanced MRI.
Figure 1. (A, B) Hyper flexion and extension radiographs showed no instability of C1–C2. (C) Sagittal reconstructive computed tomography scan of the cervical spine showed cervical degeneration and multiple cysts in the upper cervical spine. A subaxial cervical stenosis was diagnosed based on the Pavlov ratio in C3–C7. (D, E) A huge mass was noted posterior to the dens. The mass was hypointense on T1- and T2-weighted magnetic resonance imaging (MRI). (F) Only the rim of the pseudotumor was enhanced on T2-weighted contrast-enhanced MRI. 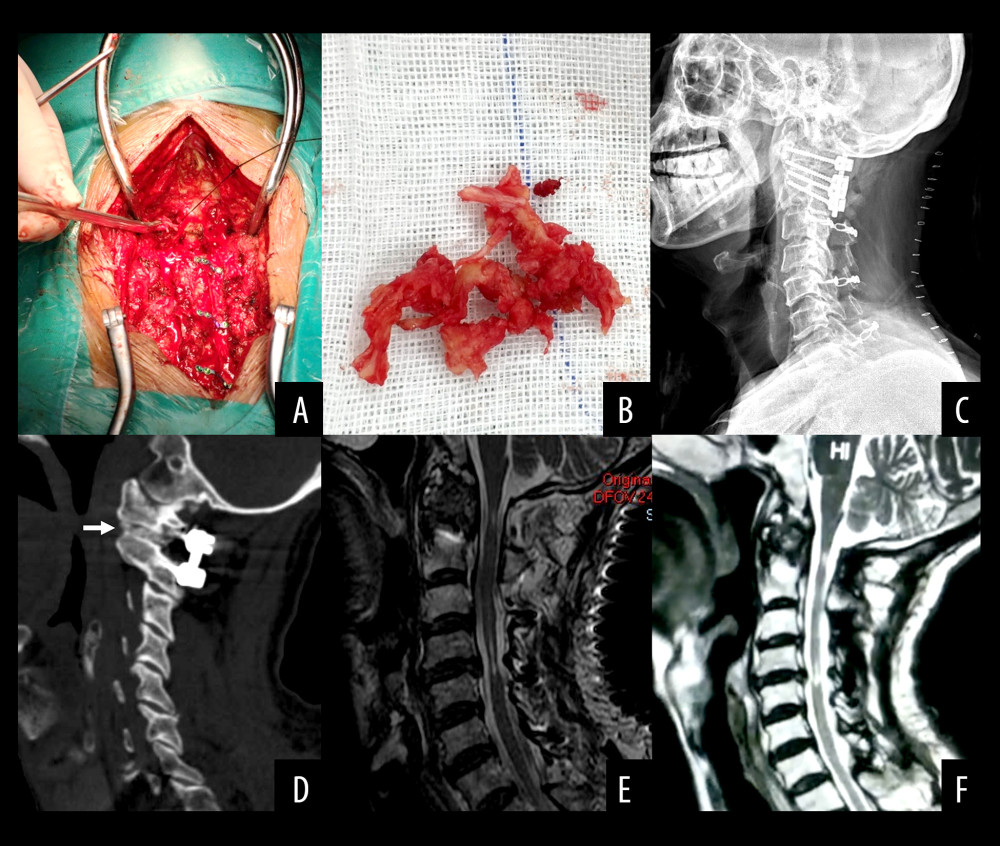 Figure 2. (A, B) The mass was resected via the lateral side of the spinal cord using a curette and clamp. The removed mass was composed of cartilaginous tissue. (C) Postoperative X-ray shows C1 lateral mass screw, C2 pedicle screw and rod fixation, and C3–C7 laminoplasty with centerpiece fixation. (D) Postoperative sagittal reconstructive computed tomography scan shows the bone graft in the lateral atlantoaxial joint. (E) Postoperative T2-weighted magnetic resonance imaging (MRI) shows complete resection of the pseudotumor and no compression of the spinal cord. (F) No tumor recurrence is shown at 1-year follow-up T2-weighted MRI.
Figure 2. (A, B) The mass was resected via the lateral side of the spinal cord using a curette and clamp. The removed mass was composed of cartilaginous tissue. (C) Postoperative X-ray shows C1 lateral mass screw, C2 pedicle screw and rod fixation, and C3–C7 laminoplasty with centerpiece fixation. (D) Postoperative sagittal reconstructive computed tomography scan shows the bone graft in the lateral atlantoaxial joint. (E) Postoperative T2-weighted magnetic resonance imaging (MRI) shows complete resection of the pseudotumor and no compression of the spinal cord. (F) No tumor recurrence is shown at 1-year follow-up T2-weighted MRI. 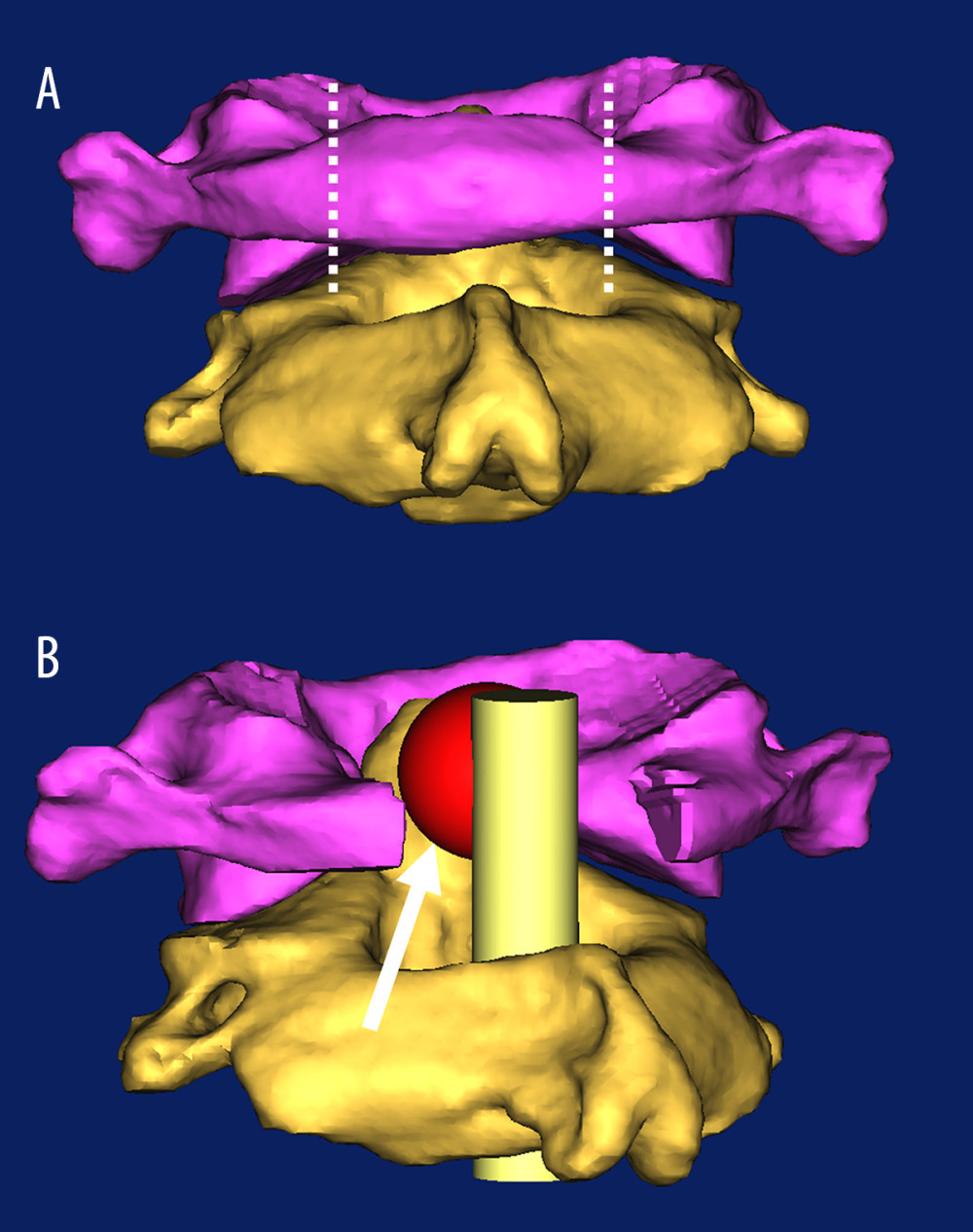 Figure 3. Schematic diagram for removal of the mass behind the dens. (A) The posterior view of the atlas and axis. The purple bone is the atlas, and the yellow bone is the axis. The area between the 2 white dotted lines represents the scope of the atlas laminectomy. (B) An oblique view of the atlas and axis after atlas laminectomy. The red sphere represents the retro-odontoid pseudotumor, the yellow cylinder represents the spinal cord, and the white arrow indicates the operative pathway.
Figure 3. Schematic diagram for removal of the mass behind the dens. (A) The posterior view of the atlas and axis. The purple bone is the atlas, and the yellow bone is the axis. The area between the 2 white dotted lines represents the scope of the atlas laminectomy. (B) An oblique view of the atlas and axis after atlas laminectomy. The red sphere represents the retro-odontoid pseudotumor, the yellow cylinder represents the spinal cord, and the white arrow indicates the operative pathway. 
References
1. Castor WR, Miller JD, Russell AS, Computed tomography of the craniocervical junction in rheumatoid arthritis: J Comput Assist Tomo, 1983; 7(1); 31-36
2. Sze G, Brant-Zawadzki MN, Wilson CR, Pseudotumor of the craniovertebral junction associated with chronic subluxation: MR imaging studies: Radiology, 1986; 161(2); 391-94
3. Rosenberg WS, Rosenberg AE, Poletti CE, Cervical disc herniation presenting as a mass lesion posterior to the odontoid process. Report of two cases: J Neurosurg, 1991; 75(6); 954-59
4. Kenez J, Turoczy L, Barsi P, Veres R, Retro-odontoid “ghost” pseudotumours in atlanto-axial instability caused by rheumatoid arthritis: Neuroradiology, 1993; 35(5); 367-69
5. Nishizawa S, Ryu H, Yokoyama T, Uemura K, Myelopathy caused by retro-odontoid disc hernia: Case report: Neurosurgery, 1996; 39(6); 1256-59
6. Jun BY, Yoon KJ, Crockard A, Retro-odontoid pseudotumor in diffuse idiopathic skeletal hyperostosis: Spine, 2002; 27(10); E266-70
7. Yonezawa I, Okuda T, Won J, Retrodental mass in rheumatoid arthritis: J Spinal Disord Tech, 2013; 26(2); E65-69
8. Nakazawa T, Inoue G, Imura T, Regression of retro-odontoid pseudotumor using external orthosis without atlantoaxial fusion: A case report: JBJS Case Connect, 2019; 9(3); e0329
9. Klas PG, Wilson J, Cusimano MD, Regression of degenerative retro-odontoid pseudotumour treated in a collar: Can J Neurol Sci, 2018; 45(5); 599-600
10. Park JH, Lee E, Lee JW, Postoperative regression of retro-odontoid pseudotumor after atlantoaxial posterior fixation: 11 years of experience in patients with atlantoaxial instability: Spine, 2017; 42(23); 1763-71
11. Shah A, Jain S, Kaswa A, Goel A, Immediate postoperative disappearance of retro-odontoid “pseudotumor”: World Neurosurg, 2016; 91; 419-23
12. Barbagallo GM, Certo F, Visocchi M, Disappearance of degenerative, non-inflammatory, retro-odontoid pseudotumor following posterior C1–C2 fixation: Case series and review of the literature: Eur Spine J, 2013; 22(Suppl 6); S879-88
13. Niwa R, Takai K, Taniguchi M, Nonrheumatoid retro-odontoid pseudotumors: Characteristics, surgical outcomes, and time-dependent regression after posterior fixation: Neurospine, 2021; 18(1); 177-87
14. Tanaka S, Nakada M, Hayashi Y, Retro-odontoid pseudotumor without atlantoaxial subluxation: J Clin Neurosci, 2010; 17(5); 649-52
15. Shi J, Ermann J, Weissman BN, Thinking beyond pannus: A review of retro-odontoid pseudotumor due to rheumatoid and non-rheumatoid etiologies: Skeletal Radiol, 2019; 48(10); 1511-23
16. Robles LA, Mundis GM, Retro-odontoid pseudotumor without radiologic atlantoaxial instability: A systematic review: World Neurosurg, 2019; 121; 100-10
17. Goel A, Retro-odontoid mass: An evidence of craniovertebral instability: J Craniovertebral Junction Spine, 2015; 6(1); 6-7
18. Venteicher AS, Goldschmidt E, Mcdowell MM, Endoscopic endonasal transodontoid approach for degenerative pseudotumor of the craniocervical junction: J Neurol Surg Part B, 2019; 80(Suppl 4); S368-69
19. Schomacher M, Jiang F, Alrjoub M, The posterior cervical transdural approach for retro-odontoid mass pseudotumor resection: Report of three cases and discussion of the current literature: Eur Spine J, 2020; 29(Suppl 2); 162-70
20. Naito K, Yamagata T, Kawahara S, High cervical lateral approach to safely remove the cystic retro-odontoid pseudotumor: Technical note: Neurol Med-Chir, 2019; 59(10); 392-97
21. Kakutani K, Doita M, Yoshikawa M, C1 laminectomy for retro-odontoid pseudotumor without atlantoaxial subluxation: Review of seven consecutive cases: Eur Spine J, 2013; 22(5); 1119-26
22. Certo F, Maione M, Visocchi M, Barbagallo G, Retro-odontoid degenerative pseudotumour causing spinal cord compression and myelopathy: Current evidence on the role of posterior C1–C2 fixation in treatment: Acta Neurochir Suppl, 2019; 125; 259-64
23. Chikuda H, Seichi A, Takeshita K, Radiographic analysis of the cervical spine in patients with retro-odontoid pseudotumors: Spine, 2009; 34(3); E110-14
24. Yurube T, Iguchi T, Kinoshita K, Upper cervical compression myelopathy caused by the retro-odontoid pseudotumor with degenerative osteoarthritis and calcium pyrophosphate dihydrate disease: A case report and literature review: Neurospine, 2021; 18(4); 903-13
25. Takahata M, Hyakkan R, Oshima S, Cervical myelopathy caused by non-rheumatic retro-odontoid pseudotumor: An investigation of underlying mechanisms and optimal surgical strategy: Glob Spine J, 2023; 13(7); 2053-62
26. Yamashita K, Aoki Y, Hiroshima K, Myelopathy due to hypoplasia of the atlas. A case report: Clin Orthop Relat R, 1997; 338(338); 90-93
27. Matsuno A, Nakashima M, Murakami M, Nagashima T, Microsurgical excision of a retro-odontoid disc hernia via a far-lateral approach: successful treatment of a rare cause of myelopathy: Case report: Neurosurgery, 2004; 54(4); 1015-18
28. Oohori Y, Seichi A, Kawaguchi H, Retroodontoid pseudotumor resected by a high cervical lateral approach in a rheumatoid arthritis patient: A case report: J Orthop Sci, 2004; 9(1); 90-93
29. Yamaguchi I, Shibuya S, Arima N, Remarkable reduction or disappearance of retroodontoid pseudotumors after occipitocervical fusion. Report of three cases: J Neurosurg Spine, 2006; 5(2); 156-60
30. Lagares A, Lagares A, Arrese I, Pannus resolution after occipitocervical fusion in a non-rheumatoid atlanto-axial instability: Eur Spine J, 2006; 15(3); 366-69
Figures
Figure 1. (A, B) Hyper flexion and extension radiographs showed no instability of C1–C2. (C) Sagittal reconstructive computed tomography scan of the cervical spine showed cervical degeneration and multiple cysts in the upper cervical spine. A subaxial cervical stenosis was diagnosed based on the Pavlov ratio in C3–C7. (D, E) A huge mass was noted posterior to the dens. The mass was hypointense on T1- and T2-weighted magnetic resonance imaging (MRI). (F) Only the rim of the pseudotumor was enhanced on T2-weighted contrast-enhanced MRI.Figure 2. (A, B) The mass was resected via the lateral side of the spinal cord using a curette and clamp. The removed mass was composed of cartilaginous tissue. (C) Postoperative X-ray shows C1 lateral mass screw, C2 pedicle screw and rod fixation, and C3–C7 laminoplasty with centerpiece fixation. (D) Postoperative sagittal reconstructive computed tomography scan shows the bone graft in the lateral atlantoaxial joint. (E) Postoperative T2-weighted magnetic resonance imaging (MRI) shows complete resection of the pseudotumor and no compression of the spinal cord. (F) No tumor recurrence is shown at 1-year follow-up T2-weighted MRI.Figure 3. Schematic diagram for removal of the mass behind the dens. (A) The posterior view of the atlas and axis. The purple bone is the atlas, and the yellow bone is the axis. The area between the 2 white dotted lines represents the scope of the atlas laminectomy. (B) An oblique view of the atlas and axis after atlas laminectomy. The red sphere represents the retro-odontoid pseudotumor, the yellow cylinder represents the spinal cord, and the white arrow indicates the operative pathway. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133