18 June 2025: Articles 
Impact of Hypoglossal Nerve Stimulation on Nocturnal Asystole in a Patient with Severe Obstructive Sleep Apnea: A Case Report
Unusual or unexpected effect of treatment
Richard E. Byrne ABCDEF 1*, Candace Miyaki ABCDEF 2DOI: 10.12659/AJCR.947160
Am J Case Rep 2025; 26:e947160






Abstract
BACKGROUND: Obstructive sleep apnea (OSA) is a highly prevalent condition associated with several cardiovascular diseases, and positive airway pressure (PAP) therapy is considered the standard treatment. In patients with OSA and nocturnal bradyarrhythmias, treatment with PAP therapy improves nocturnal bradyarrhythmias and is the basis for recommending OSA screening in patients with asymptomatic nocturnal bradyarrhythmia. As many patients do not tolerate PAP therapy, alternative treatment options like hypoglossal nerve stimulation (HNS) have been developed. Less is known regarding whether HNS therapy improves nocturnal bradyarrhythmia to a similar extent as PAP therapy. Our case highlights the unexpected return of nocturnal asystole in a patient who switched from PAP therapy to HNS therapy.
CASE REPORT: We report a case of a 77-year-old man with severe obstructive sleep apnea and nocturnal asystole treated with PAP therapy. Due to dissatisfaction with PAP therapy, he switched to HNS therapy. Upon discontinuing PAP therapy and during the self-titration phase of HNS therapy, the nocturnal asystole events returned unexpectedly despite symptomatic benefit from HNS therapy. Given the patient’s concerns regarding the return of nocturnal asystole, he resumed PAP therapy and discontinued HNS therapy, which resolved the bradyarrhythmia.
CONCLUSIONS: The self-titration phase of HNS therapy can precipitate the return of comorbid conditions, like bradyarrhythmias, which can lead to patients abandoning therapy. Patients considering switching from PAP therapy to HNS therapy should be counseled that this can occur. Research evaluating the effects of HNS therapy on outcomes like nocturnal bradyarrhythmias using implanted loop recorders is warranted.
Keywords: Hypoglossal Nerve, Continuous Positive Airway Pressure, Arrhythmias, Cardiac, Apnea, Humans, Male, Aged, Sleep apnea, obstructive, Heart Arrest, Electric Stimulation Therapy, Bradycardia
Introduction
Obstructive sleep apnea (OSA) is a common condition in which the upper airway repeatedly collapses during sleep [1]. It is highly prevalent, affecting 13–33% of men and 6–19% of women [1]. It has been associated with numerous comorbid conditions, including obesity, coronary artery disease, hypertension, arrhythmia, heart failure, stroke, pulmonary hypertension, and insulin resistance [1]. OSA is diagnosed by performing a sleep study to measure the apnea hypopnea index (AHI). The standard treatment for OSA is positive airway pressure (PAP), including continuous positive airway pressure (CPAP) and bilevel positive airway pressure (BPAP), which prevents upper airway collapse by acting as a pneumatic splint [1]. Alternative treatments like hypoglossal nerve stimulation (HNS) can be considered when patients have difficulty adhering to PAP therapy [1]. HNS therapy requires surgically implanting a stimulation cuff around the hypoglossal nerve under the chin, a pulse generator in the chest, and a respiratory sensing lead in the chest [2]. It improves upper airway patency and treats OSA by anteriorly protruding the tongue during inspiration [2]. Approximately 4 weeks after surgical implantation, the device is activated, and patients are instructed on how to turn on the device using a remote control [3]. The goal when first starting HNS therapy is to acclimate to therapy, even if the stimulation levels are subtherapeutic [3]. The patient gradually increases stimulation levels on their own to improve sleep apnea symptoms. If patients are tolerating and benefiting from HNS therapy, an HNS titration sleep study is performed approximately 12 weeks after activation, which provides objective AHI data at different stimulation levels [3].
Nocturnal bradyarrhythmias have been associated with OSA and include sinus bradycardia, sinus arrest, AV block, and asystole [4]. Sinus bradycardia in sleep is defined as a sustained (>30 seconds) sinus heart rate less than 40 beats per minute, and asystole is defined as cardiac pauses during sleep >3 seconds [5]. If a patient is symptomatic from nocturnal bradyarrhythmia, permanent pacemaker implantation can be considered after reversible causes have been evaluated and treated. However, patients are frequently asymptomatic, given the occurrence in sleep, so permanent pacemaker implantation is not usually indicated [4]. Evaluation for OSA is recommended in patients with asymptomatic nocturnal bradyarrhythmias because treatment of sleep apnea with PAP can effectively improve nocturnal bradyarrhythmias, even without permanent pacemaker implantation [4]. Because many patients have difficulty achieving adequate usage with PAP therapy, HNS has been developed as an alternative treatment option. Investigation of efficacy has focused on patient symptoms and sleep apnea metrics. Some reports show greater AHI reduction with PAP therapy but lower post-treatment Epworth Sleepiness Scale scores with HNS therapy [6]. Investigations of other sleep apnea consequences are ongoing. A notable component of HNS is the self-titration process following activation, whereby the patient gradually increases stimulation amplitude to improve sleep apnea symptoms and sleep apnea severity, with an eventual HNS titration polysomnogram, which does not occur until at least 3 months after activation [3].
An implanted loop recorder is a subcutaneously implanted device capable of long-term ambulatory electrocardiogram monitoring [7]. The implanted loop recorder can be interrogated at varying intervals to review various electrocardiographic events. Implanted loop recorders have been utilized previously to evaluate CPAP therapy effects on bradycardia and cardiac pauses, and have shown near resolution of bradycardia and cardiac pauses after 8 weeks of CPAP treatment [7]. We did not find any published data regarding evaluating HNS therapy effects on nocturnal bradycardia and cardiac pauses using implanted loop recorders. To the best of our knowledge, this is the first case report on use of an implanted loop recorder data to monitor nocturnal asystole in a patient who switched from BPAP to HNS therapy, with subsequent increase in nocturnal asystole events, which then resolved upon discontinuing HNS therapy and restarting BPAP.
Case Report
A 77-year-old man diagnosed with severe obstructive sleep apnea (nocturnal polysomnogram performed approximately 1 year prior to HNS implantation showed an AHI 76.9/h, with central and mixed apnea indices 0/h) who had persistent difficulty tolerating BPAP therapy decided to pursue HNS therapy. His medical history was significant for obesity (body mass index 33.2), hypertension, and asymptomatic nocturnal asystole with an implanted loop recorder (Medtronic LINQ II). His upper airway exam was significant for a slight right nasal septum deviation, modified Mallampati class 3 airway, and tonsil grading of 1+. A recent transthoracic echocardiogram noted normal left ventricular ejection fraction, mild mitral regurgitation, and mild aortic insufficiency. A baseline electrocardiogram from the loop recorder is shown in Figure 1. He was started on BPAP approximately 8 months prior to HNS implantation, but only averaged 3 hours 36 minutes usage per night (in the 8 months leading up to implantation) with more interrupted sleep and persistent sleepiness (with an elevated Epworth Sleepiness Scale score of 19) while on BPAP therapy. He continued BPAP therapy despite his dissatisfaction due to the resolution of asystole events reported from his implanted loop recorder and reduction of AHI to less than 5/h. He desired alternative treatments for sleep apnea because of self-reported less sleep and poor sleep quality with PAP and underwent evaluation for HNS therapy. A drug-induced sleep endoscopy showed 75% anterior-posterior collapse at the level of the velum (there was no complete concentric collapse) and 75% obstruction at the level of the tongue base, which were amenable findings for HNS therapy. While his AHI was greater than 65/h, he was a candidate for HNS under the expanded US Food and Drug Administration indication [8]. He underwent HNS (Inspire Implantable Pulse Generator Model 3028) implantation with 2-incision technique and had an uneventful postoperative course. Activation was performed approximately 1 month after implantation. He was started on his functional threshold amplitude of 0.8 volts (V), electrode A, pulse width 90 μs, rate 33Hz, and was instructed to increase stimulation levels gradually as tolerated, with a goal of symptom improvement. Upon discontinuing BPAP and starting HNS therapy alone, he reported improvement in his sleep quality, which he attributed to no longer having to use BPAP therapy. Unfortunately, he began receiving frequent calls from the cardiology team regarding nocturnal asystole events at times as long as 8 seconds (Figure 2). This was unexpected, as his nocturnal asystole had been excellently controlled with PAP therapy, even with sub-optimal use. He was able to self-titrate the HNS amplitude to 1.4 V, at which point he had difficulty tolerating the stimulation and was still receiving calls about nocturnal asystole events. His average use of HNS therapy over 24 nights was 6 hours per night. Given his concerns regarding the nocturnal asystole, he then discontinued HNS therapy after 24 nights of amplitude self-titration and resumed BPAP therapy, which promptly resolved the nocturnal asystole events. He was able to try a different BPAP therapy interface, which resulted in less perceived air leak, less interrupted sleep, and improved nightly use (average use 4 hours 53 minutes per night in the 30 days after discontinuing HNS therapy and resuming BPAP). His Epworth Sleepiness Scale score on returning to BPAP alone was mildly improved (15) at follow-up, which occurred 2 months after activation. He declined the usual assessment of HNS therapy efficacy with an HNS titration, so the AHI while on HNS therapy is not available.
The frequency and timing of nocturnal asystole events greater than or equal to 5 seconds were compiled from his loop recorder. The asystole occurred almost exclusively during his usual sleeping hours. During BPAP therapy (for the 60 days before starting HNS therapy and for the 18 days after discontinuing HNS therapy), he had no asystole ≥5 seconds (Table 1). During the HNS therapy self-titration phase, while off BPAP, the mean number of asystole ≥5 seconds events per day was 0.79. The Mann-Whitney U test (SPSS version 29) was performed to compare the number of asystole events lasting 5 seconds or longer per day before HNS therapy on BPAP to during HNS therapy, and during HNS therapy to after stopping HNS therapy resuming BPAP. The data show a statistically significant lower frequency of asystole on BPAP therapy compared to HNS therapy.
Discussion
Our patient had nocturnal asystole returning during the HNS self-titration phase when switching from PAP therapy to HNS therapy, and we show that implanted loop recorders can provide actionable data when evaluating HNS therapy efficacy. An important consideration when counseling patients about discontinuing PAP therapy in favor of HNS therapy is that previously controlled comorbid conditions (in our patient, nocturnal asystole) can worsen during the self-titration phase of HNS therapy. This may occur because the self-titration phase starts at a low stimulation setting to allow the patient to acclimate to HNS therapy, which may not adequately treat the OSA. It can take several months for a patient to achieve an effective stimulation setting, and the timeframe can vary significantly depending on patient tolerance of the stimulation [3]. We were surprised at the worsening of nocturnal asystole upon discontinuing BPAP therapy and starting HNS therapy, as our patient noticed improved sleep quality, self-reported benefit, and higher average nightly use with HNS therapy, which suggests some degree of efficacy. Conversely, BPAP therapy at lower self-reported benefit and lower average nightly use was highly effective at suppressing our patient’s nocturnal asystole. This is similar to previously reported data showing PAP therapy is highly effective in improving bradycardia and cardiac pauses [7]. We suggest that patients who are being treated successfully for nocturnal bradyarrhythmia with borderline PAP use should be cautioned that their bradyarrhythmia can worsen if they discontinue PAP therapy and proceed with HNS therapy alone, especially during the HNS self-titration phase. While some patients may be willing to use PAP therapy combined with HNS therapy until an effective HNS configuration is achieved, our patient, alarmed by the duration of nocturnal asystole, returned to PAP therapy alone and abandoned HNS therapy.
The second consideration shown by our case is the ability to use implanted loop recorder data as a surrogate for typical outcome measures (like AHI) prior to formal sleep testing during the HNS self-titration phase. In contrast to previously reported data showing PAP therapy’s effectiveness in improving bradyarrhythmias [7], we saw that HNS therapy during the self-titration phase was not effective in improving bradyarrhythmia. However, our patient decided to abandon HNS therapy before we were able to evaluate its effect on AHI with the HNS titration, so it is uncertain whether HNS therapy alone would have eventually been able to suppress his nocturnal asystole. Upon activation of HNS therapy, there is usually a delay in knowing its effectiveness in reducing the AHI, as an HNS titration is generally performed at least 3 months after activation [3]. PAP therapy with AHI reporting affords the patient a more immediate objective view of efficacy, as many PAP therapy devices have mobile device apps in which these data can be self-monitored nightly [9]. We suggest that in patients with implanted loop recorders undergoing HNS therapy, the frequency of nocturnal asystole and other arrhythmias may be a useful interim objective longitudinal efficacy metric that can be assessed while awaiting an HNS titration or other single-night sleep testing to help guide amplitude self-titration and adjustments.
The literature describing OSA treatment’s effects on bradyarrhythmia has centered around PAP therapy. Even with less than consistent usage, there have been improvements with bradyarrhythmia (58% of patients reported always using PAP therapy) [10]. Other treatment options with reported efficacy include tracheostomy [11], theophylline [12]. and supplemental oxygen (the efficacy of supplemental oxygen is uncertain) [13]. We were unable to find published data regarding the treatment effects of other PAP alternatives like HNS therapy, mandibular advancement devices, and positional therapy on nocturnal bradyarrhythmia. Clarifying the treatment effect on nocturnal bradyarrhythmias for each treatment modality is important given that even intermediate-length nocturnal pauses solely occurring at night increase the risk for adverse cardiovascular consequences, although notably not mortality [14]. Discussing the expected efficacy of HNS therapy for each patient based on their individual comorbidities is also necessary. In conclusion, while HNS therapy can be an effective treatment for OSA based on the usual metrics, patients switching from PAP therapy to HNS therapy may experience worsening of comorbidities, like nocturnal asystole, during the self-titration phase, despite symptomatic benefit, and implanted loop recorder data can provide interim efficacy data prior to HNS titration sleep testing.
Conclusions
Patients with controlled nocturnal asystole who switch from PAP therapy to HNS therapy may experience worsening of nocturnal asystole during the self-titration phase of HNS therapy. Worsening of comorbidities can lead to patients abandoning HNS therapy and returning to PAP therapy. Implanted loop recorder data can be a useful adjunct to evaluate efficacy of HNS therapy in patients with nocturnal bradyarrhythmia prior to the usual HNS titration sleep testing, which occurs several months after HNS activation.
Figures
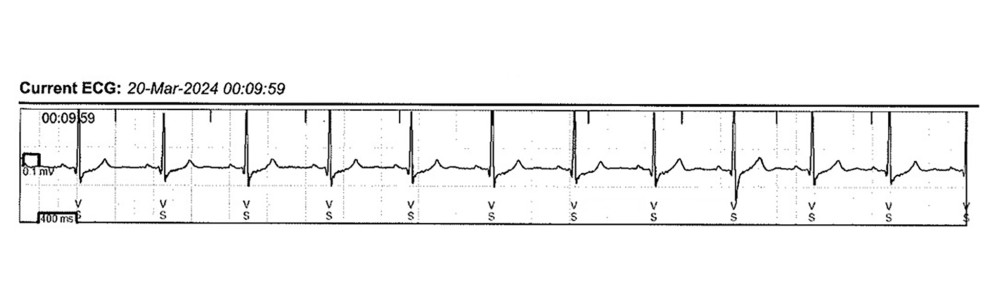 Figure 1. Baseline electrocardiogramThe patient’s baseline electrocardiogram from the implanted loop recorder.
Figure 1. Baseline electrocardiogramThe patient’s baseline electrocardiogram from the implanted loop recorder. 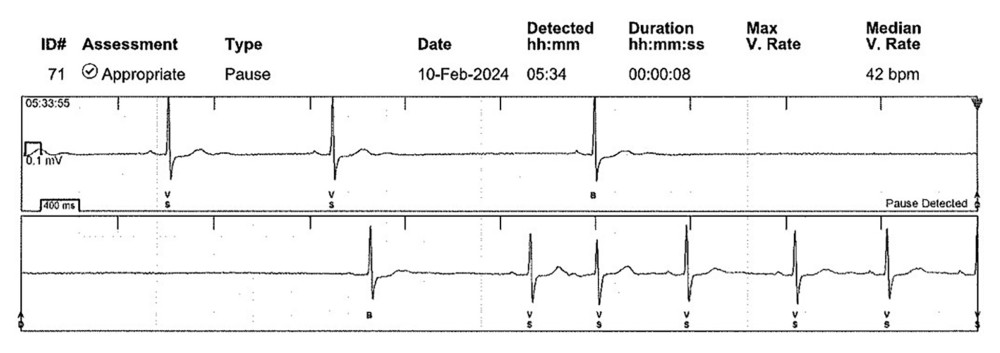 Figure 2. Eight-second asystoleThe electrocardiogram from the patient’s implanted loop recorder demonstrates an approximately 8-second asystole during his usual sleeping hours. This event occurred during the self-titration phase of hypoglossal nerve stimulation therapy, while off bilevel positive airway pressure therapy. The vertical lines at the top of each row denote 1-second intervals.
Figure 2. Eight-second asystoleThe electrocardiogram from the patient’s implanted loop recorder demonstrates an approximately 8-second asystole during his usual sleeping hours. This event occurred during the self-titration phase of hypoglossal nerve stimulation therapy, while off bilevel positive airway pressure therapy. The vertical lines at the top of each row denote 1-second intervals. References
1. Chang JL, Goldberg AN, Alt JA, International consensus statement on obstructive sleep apnea: Int Forum Allergy Rhinol, 2023; 13(7); 1061-482
2. Strollo PJ, Soose RJ, Maurer JTSTAR Trial Group, Upper-airway stimulation for obstructive sleep apnea: N Engl J Med, 2014; 370(2); 139-49
3. Soose RJ, Faber K, Greenberg H, Post-implant care pathway: Lessons learned and recommendations after 5 years of clinical implementation of hypoglossal nerve stimulation therapy: Sleep, 2021; 44(Suppl 1); S4-S10
4. Kusumoto FM, Schoenfeld MH, Barrett C, 2018 ACC/AHA/HRS Guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society: Circulation, 2019; 140(8); e382-482
5. Troester MM, Quan SF, Berry RBfor the American Academy of Sleep Medicine: The AASM Manual for the scoring of sleep and associated events: Rules, terminology and technical specifications. Version 3 Available from: learn.aasm.org
6. Pordzik J, Ludwig K, Seifen C, Real-world data on polysomnography- and patient-reported outcomes in hypoglossal nerve stimulation and auto-titrating positive airway pressure therapy for obstructive sleep apnea: Respir Med, 2024; 232; 107750
7. Simantirakis EN, Schiza SI, Marketou ME, Severe bradyarrhythmias in patients with sleep apnoea: the effect of continuous positive airway pressure treatment: A long-term evaluation using an insertable loop recorder: Eur Heart J, 2004; 25(12); 1070-76
8. : fda.gov [Internet], c2023, Silver Spring: Food and Drug Administration [cited 2024 Jun 22]. Available from:https://www.accessdata.fda.gov/cdrh_docs/pdf13/P130008S089B.pdf
9. Shaughnessy GF, Morgenthaler TI, The effect of patient-facing applications on positive airway pressure therapy adherence: A systematic review: J Clin Sleep Med, 2019; 15(5); 769-77
10. Grimm W, Koehler U, Fus E, Outcome of patients with sleep apnea-associated severe bradyarrhythmias after continuous positive airway pressure therapy: Am J Cardiol, 2000; 86(6); 688-92
11. Guilleminault C, Connolly SJ, Winkle RA, Cardiac arrhythmia and conduction disturbances during sleep in 400 patients with sleep apnea syndrome: Am J Cardiol, 1983; 52(5); 490-94
12. Daoulah A, Ocheltree S, Al-Faifi SM, Sleep apnea and severe bradyarrhythmia – an alternative treatment option: A case report: J Med Case Rep, 2015; 9; 113
13. Huettner M, Koehler U, Nell C, Heart rate response to simulated obstructive apnea while awake predicts bradycardia during spontaneous obstructive sleep apnea: Int J Cardiol, 2015; 186; 216-18
14. Liu CM, Lin CY, Chang SL, Intermediate pause at daytime is associated with increased cardiovascular risk and mortality: An 8-year cohort study: J Am Heart Assoc, 2018; 7(12); e009034
Figures
Figure 1. Baseline electrocardiogramThe patient’s baseline electrocardiogram from the implanted loop recorder.Figure 2. Eight-second asystoleThe electrocardiogram from the patient’s implanted loop recorder demonstrates an approximately 8-second asystole during his usual sleeping hours. This event occurred during the self-titration phase of hypoglossal nerve stimulation therapy, while off bilevel positive airway pressure therapy. The vertical lines at the top of each row denote 1-second intervals. Tables
 Table 1. Nocturnal asystole (≥5 seconds) compilationThe table demonstrates the frequency of nocturnal asystole (≥5 seconds) events reported by the patient’s implanted loop recorder while using bilevel positive airway pressure (BPAP) and hypoglossal nerve stimulation (HNS).Table 1. Nocturnal asystole (≥5 seconds) compilationThe table demonstrates the frequency of nocturnal asystole (≥5 seconds) events reported by the patient’s implanted loop recorder while using bilevel positive airway pressure (BPAP) and hypoglossal nerve stimulation (HNS).
Table 1. Nocturnal asystole (≥5 seconds) compilationThe table demonstrates the frequency of nocturnal asystole (≥5 seconds) events reported by the patient’s implanted loop recorder while using bilevel positive airway pressure (BPAP) and hypoglossal nerve stimulation (HNS).Table 1. Nocturnal asystole (≥5 seconds) compilationThe table demonstrates the frequency of nocturnal asystole (≥5 seconds) events reported by the patient’s implanted loop recorder while using bilevel positive airway pressure (BPAP) and hypoglossal nerve stimulation (HNS). In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133