25 April 2025: Articles 
Agenesis of the Dorsal Pancreas and Its Possible Link to Pancreatic Neuroendocrine Tumors: Case Insights
Challenging differential diagnosis, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Alessia FassariDOI: 10.12659/AJCR.947512
Am J Case Rep 2025; 26:e947512






Abstract
BACKGROUND: Agenesis of the dorsal pancreas (ADP) is a rare congenital anomaly resulting from incomplete development of the dorsal pancreatic bud, affecting the body and tail of the pancreas. While often asymptomatic, it can present with clinical abnormalities such as abdominal pain, diabetes, or obstructive jaundice, and may be associated with chronic pancreatitis and tumors. We report the third documented case of a high-grade neuroendocrine tumor located at the head of the pancreas in a patient with complete ADP, along with a review of the literature.
CASE REPORT: An 86-year-old man presented with jaundice caused by a 3-cm pancreatic mass compressing the bile duct, confirmed through imaging to be associated with ADP. Surgical intervention was declined, and a combined laparoscopic and radiological approach was used to place a biliary stent, alleviating symptoms. Histopathological analysis confirmed a poorly differentiated neuroendocrine carcinoma (NEC). Despite initial symptomatic relief, the patient died due to complications 3 months later.
CONCLUSIONS: This report underscores the diagnostic challenges of ADP and its potential association with pancreatic neoplasms. Improved imaging techniques such as computed tomography (CT), magnetic resonance imaging (MRI), and endoscopic ultrasound (EUS) facilitate diagnosis and differentiation from similar conditions. The association between ADP and pancreatic tumors should warn us to be watchful with every patient diagnosed with ADP and focus on the early detection of possible malignancies. Further research is needed to clarify the genetic and developmental mechanisms linking ADP to tumorigenesis and to explore targeted therapeutic approaches.
Keywords: Congenital Abnormalities, neuroendocrine tumors, Pancreatic Diseases, Pancreatic Neoplasms, Humans, Male, Pancreas, Aged, 80 and over, Fatal Outcome
Introduction
Complete or partial agenesis of the dorsal pancreas (ADP) is a rare congenital anomaly caused by the failing embryological development of the dorsal pancreatic bud, including its body and tail. This condition may be asymptomatic, found incidentally on imaging, or associated with clinical abnormalities. The first description of ADP was published in 1911 in a post-mortem examination [1]; since then, more cases have been described in the literature.
Even more uncommon are pancreatic tumors arising within this malformation. We hereby present the third case ever reported of a neuroendocrine tumor located at the head of the pancreas developed in the context of ADP. This report also includes the case in the context of a broader review of the literature to provide the most complete illustration of ADP starting from clinical presentation, to diagnosis, and to the possible association with other pathologies, all fundamental aspects for choosing the best treatment when necessary.
Case Report
The present case report was developed according to the Consensus-based Clinical Case Reporting Guideline (CARE checklist) [2]. An 86-year-old man presented to our service due to sudden-onset jaundice. His medical history included chronic pancreatitis, hypercholesterolemia, systemic arterial hypertension, and infrarenal abdominal aortic aneurysm. Blood tests demonstrated jaundice with 7.5 mg/dL of total bilirubin (normal range 0.1 to 1.2 mg/dL), 6.8 mg/dL of direct bilirubin (normal value less than 0.3 mg/dL), and cholestasis with 762 UI/L of Gamma-GT (normal range 5 to 40 U/L). The other liver and pancreatic enzymes were normal. An abdominal computed tomography (CT) scan was performed, suspecting a pancreatic neoplasia. The imaging showed complete atrophy of the pancreatic body and tail, associated with a 3-cm mass of the head compressing the bile duct, thus causing intra- and extrahepatic biliary dilatation (Figure 1). The mass was in contact with the superior mesenteric vein (SMV) for 1/3 of its circumference (on the right side) and multiple lymph-adenomegalies were found (interaortic, caval, peri-pancreatic, and left of hepatic hilum). Tumoral markers (CEA, CA19.9) were within normal limits.
Additionally, magnetic resonance cholangiopancreatography (MRCP) was performed, confirming the complete absence of the pancreatic body and tail. The MRCP report described a major obstruction of the distal common bile duct due to an inhomogeneous pancreatic head mass, most likely of tumoral origin. A large lymph node was identified posterior to the splenomesenteric venous confluence. No evidence of secondary focal hepatic lesions was observed. Gallbladder distension was also noted (Figure 2).
After collegial discussion among staff, patient, and family members, who refused a burdensome surgical operation like pancreaticoduodenectomy, we proposed the positioning of an endoscopic biliary prosthesis. Two endoscopic retrograde cholangiopancreatography (ERCP) procedures were performed. The first ERCP showed a normal aspect of the major papilla, with absence of the dorsal ductal system and the minor papilla, definitively confirming the diagnosis of ADP. Partial opacification of the main bile duct revealed a stenosis in the distal portion, with upstream biliary dilatation. Multiple attempts were made to pass a guidewire beyond the stenosis, all of which were unsuccessful. During the procedure, congestion of the papilla of Vater was observed, leading to early termination of the examination. The second ERCP attempt also failed to pass the stenosis and place a stent, reinforcing the suspicion of a pancreatic neoplastic process causing a distal biliary stricture.
Thus, we had to resort to a radiologic approach by percutaneous transhepatic biliary drainage (PTBD), but this also encountered some obstacles. The patient had a significant colon interposition between liver and diaphragm, compatible with a Chilaiditi sign (Figure 3); therefore, we performed a combined procedure, with laparoscopic retraction of the right colon to better expose the liver and biliary target. Peritoneal exploration suggested a cholestatic liver, with slight fibrosis and precirrhosis. The right colon, interposed between the liver and diaphragm, was retracted out of the way, towards the pelvis, and the right colic flexure was fixed with an absorbable braided suture stitch. The PTBD, followed by metal biliary stent positioning, could then be safely approached and was carried out uneventfully (Figure 4). During the laparoscopic exploration, we encountered a small, whitish lesion corresponding to the IV liver segment, which was biopsied for pathological examination. The positioning of the PTBD led to a rapid decrease in bilirubin values, with improved patient comfort. He was discharged 11 days after the procedure and returned home assisted by his family and with a nursing care program.
The pathologic examination suggested a malignant neoplastic lesion. The immunohistochemistry results were positive for neuroendocrine markers CD56, chromogranin, and synaptophysin, positive for CK19, and negative for CK7, CK20, and hepatocyte (HePar1). Moreover, the tumor exhibited a high Ki-67 proliferation index (60%), nuclear atypia, and extensive necrosis, confirming the diagnosis of a poorly differentiated neuroendocrine carcinoma (NEC). The patient was readmitted to the hospital 3 months later due to a worsening general condition, with cachexia and abdominal pain. Laboratory tests showed worsening liver damage and function, associated with cholangitis, which despite antibiotics and supportive treatment, ultimately led to the patient’s death.
Discussion
CLINICAL PRESENTATION AND CASE-SPECIFIC INSIGHTS:
When symptomatic, ADP commonly presents with abdominal pain, often localized in the epigastric area with back radiation, and may be exacerbated by eating. Additional symptoms include bloating, dyspepsia, nausea, vomiting, diarrhea, steatorrhea, and altered blood glycemic control [4]. The association with chronic pancreatitis, as seen in our patient, is relevant because the absence of the pancreatic body and tail can pre-dispose to abnormal pancreatic duct pressure, leading to inflammation and fibrosis.
The sudden onset of obstructive jaundice in our patient was unusual and linked to the presence of a pancreatic head neoplasm. While some case reports in the literature have described biliary obstruction due to stones in the common bile duct, neoplastic involvement remains a rare presentation of ADP [5–11]. The lack of documented exocrine insufficiency and diabetes mellitus in our patient further supports the congenital nature of the pancreatic atrophy rather than an acquired atrophic process secondary to his chronic pancreatitis.
DIAGNOSTIC CHALLENGES AND THE ROLE OF IMAGING:
In recent years there has been a notable increase in ADP diagnoses. This is not due to a real change in the incidence of this anomaly but rather to the improvement and innovation of diagnostic techniques, especially radiological and interventional ones that allow a definitive diagnosis. Although ultrasound (US) is almost always the first test performed for screening or sometimes to investigate the origin of abdominal pain, this exam has some limitations due to the deep location of the pancreas and possible interference from abdominal meteorism and does not allow a definitive diagnosis. Moreover, ADP recognizes a set of possible competing diagnoses with other entities such as pancreas divisum, failing fusion of the ventral and dorsal pancreatic ducts, pseudo-lipodystrophy of the pancreas, partial agenesis, pseudo-agenesis, and pancreatic lipomatosis [12]. To obtain a differential diagnosis it is necessary to identify the main pancreatic duct, which in ADP patients is typically absent in the body and tail of the gland. CT has become a cornerstone in diagnosing ADP, as it allows for the identification of characteristic radiological findings such as the “dependent stomach sign” and “dependent intestine sign” [13]. These signs indicate the absence of pancreatic tissue by demonstrating direct apposition of the stomach or intestinal loops to the splenic vein. This allows diagnosis of ADP and differentiates it from other conditions like atrophy, lipomatosis, and surgical excisions.
While ERCP is the criterion standard for evaluating the pancreatic duct, it is invasive and reserved as a last resort due to potential complications and operator-dependent success. Magnetic resonance imaging (MRI) and MRCP are preferred as less invasive alternatives (14). Endoscopic ultrasound (EUS) is also valuable for detecting the pancreatic duct, especially in cases of pancreas divisum and chronic pancreatitis [15]. Although few studies have focused on EUS for ADP diagnosis, it remains an important tool, particularly when combined with endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) for detecting pancreatic tumors [16]. Since each imaging modality has strengths and limitations, integrating multiple imaging techniques is crucial for accurate diagnosis and management.
In our case, the diagnosis was confirmed by 3 radiological exams – CT, MRCP, and ERCP – with the last necessary to attempt a prosthesis placement, without success. The interventional procedure was further complicated by the presence of Chilaiditi’s sign, a rare radiological finding first described in 1910 by Demetrius Chilaiditi [17]. This condition, marked by colonic interposition between the liver and diaphragm, posed a technical challenge in the placement of a biliary prosthesis. The necessity for a combined laparoscopic and percutaneous approach underscores the importance of individualized management strategies in patients with complex anatomical variants. The preoperative identification of Chilaiditi’s sign allowed us to anticipate procedural difficulties and plan accordingly, ensuring a safer intervention.
ASSOCIATED DISEASES:
Diabetes mellitus (DM) is the disorder most frequently associated with ADP, found in approximately 50% of cases. It is widely known that the islets are mainly located in the tail of the pancreas and that the β-cells ensure a better response to the glucose variation. The reduced count of β-cells in the ADP, similarly to patients who undergo pancreatic surgical resection, may contribute to the development of DM. This is partly due to the reduced in vivo replication of β-cells in the ADP and partly to β-cells apoptosis induced by DM type 2 [18–22]. An association with polysplenia syndrome (PS) has also been found. PS is a subtype of heterotaxy that occurs in approximately 4 of every million live births and is characterized by cardiac malformations, bilobed lung, visceral malrotation, multiple spleens, and vascular anomalies like interruption of the inferior vein cava with continuation azygos or hemiazygos and preduodenal portal vein [23–25]. Despite the vast heterogeneity of its manifestations, the only distinctive sign of PS is given by the presence of multiple spleens, typically located along the greater curve of the stomach. As the dorsal pancreas and spleen develop into the dorsal mesogastrium, concomitant abnormalities of both organs can occur in patients with PS.
In our patient, the spleen was normal, but he had a history of pancreatitis. This could be explained by the prominent or compensatory hypertrophy of the ventral gland, which leads to higher intrapancreatic duct pressures and sphincter of Oddi dysfunction [26–39].
ADP AND MALIGNANCY RISK:
A growing body of literature suggests a potential association between ADP and an increased risk of pancreatic neoplasia. An association with tumors was found in 30 patients, including our case (24.1% of all cases reported in the literature) [6,7,9–12,31–48] (Table 1). The absence of dorsal pancreatic tissue may predispose to chronic inflammation, which in turn can contribute to neoplastic transformation. In our case, the presence of a high-grade NEC in the pancreatic head highlights the importance of vigilance in ADP patients. The liver biopsy confirmed metastatic involvement, but the primary pancreatic lesion was not directly sampled. The tumor’s immunohistochemical profile, including CD56, chromogranin, synaptophysin positivity, and a Ki-67 index of 60%, was consistent with a highly aggressive NEC.
Several genetic pathways have been implicated in both pancreatic development and tumorigenesis. It was recently shown that retinoic acid (RA) signaling is essential for many aspects of mammalian physiology such as morphogenesis and organogenesis and fetal and perinatal growth [49]. To assess the effect of altered retinaldehyde dehydrogenase 2 (Raldh2), the enzyme required for RA synthesis, Martin et al studied the phenotype of mice with targeted deletion of the Raldh2 gene, finding that this gene was expressed in dorsal pancreatic mesenchyme, and Raldh2 deficiency led to a failure in pancreatic dorsal bud development in mice. Mutant mice also lacked Pdx1 expression and there were fewer cells expressing homeobox (HB) gene Hlxb9, both essential for proper pancreatic differentiation [50]. Since retinoids primarily affect cell growth, differentiation, and death, it seems clear that deregulation of retinoid signaling pathways is directly linked to tumorigenesis, which, in essence, is a developmental disorder. Brown found lower retinoids levels within tissues from patients with pancreatic ductal adenocarcinoma as measured by high-performance liquid chromatography mass spectroscopy compared with healthy pancreatic tissue [51]. Specifically, RARγ has been shown to be an oncogene for many different tumors by regulating DNA damage-induced cell death. Knowledge of these mechanisms appears increasingly important as numerous studies are already underway to identify target therapies to replace unsuccessful conventional chemotherapy.
Unfortunately, no genetic testing (eg, next-generation sequencing) or retinoid level analysis was performed in our patient. While these analyses could provide valuable insights into the molecular mechanisms linking ADP to tumorigenesis, we acknowledge this limitation and emphasize the importance of incorporating such approaches in future studies to better understand these potential pathways.
IMPLICATIONS FOR MANAGEMENT:
Given the association between ADP and pancreatic malignancies, heightened suspicion is needed in patients with this congenital anomaly, particularly when new clinical symptoms emerge. In our case, the lack of direct histological confirmation of the pancreatic mass remains a limitation, but the overall clinical and radiological findings strongly support a pancreatic primary. The decision to pursue palliative biliary drainage rather than surgical resection was guided by patient-specific factors, including age, comorbidities, and family preferences. This aligns with findings from studies evaluating oncological treatment strategies in elderly patients, which highlights the importance of individualized treatment approaches in older patients [52,53].
The association between ADP and pancreatic tumors underscores the need for long-term surveillance strategies in these patients. While routine screening for pancreatic neoplasms in ADP has not been established, a lower threshold for imaging and tissue sampling should be considered in symptomatic individuals.
Conclusions
Various authors have recently different suggested the role of deregulated hedgehog signaling in pancreatic development and pancreatic diseases, including DM, chronic pancreatitis, and pancreatic cancer. The association between ADP and pancreatic tumors should warn us to be watchful with every patient diagnosed with ADP and focus on the early detection of possible malignancies. The case presented here highlights the rare association between ADP and pancreatic NEC, emphasizing the importance of recognizing congenital pancreatic anomalies as potential risk factors for malignancy. The diagnostic complexity of ADP, compounded by anatomical variations such as Chilaiditi’s sign, underscores the need for a multidisciplinary approach in managing these patients. Further research is warranted to elucidate the genetic and inflammatory mechanisms linking ADP to pancreatic tumorigenesis, potentially paving the way for targeted surveillance and early intervention strategies.
Figures
References:
1.. Heiberg KA, [A case of missing cauda pancreatis (in a diabetic patient).]: Centralbl Allg Pathol Patholog Anat, 1911; 22; 676-77 [in German]
2.. Gagnier JJ, Kienle G, Altman DG, CARE Group The CARE guidelines: Consensus-based clinical case reporting guideline development: BMJ Case Rep, 2013; 2013 bcr2013201554
3.. Haldorsen IS, Vesterhus M, Raeder H, Lack of pancreatic body and tail in HNF1B mutation carriers: Diabet Med, 2008; 25(7); 782-87
4.. Doxey BW, Jackson WD, Adler DG, A unique presentation: dorsal agenesis of the pancreas manifesting as pancreatic exocrine insufficiency in the absence of diabetes mellitus in an 8-year-old boy: Dig Dis Sci, 2008; 53(7); 2005-6
5.. Fukuoka K, Ajiki T, Yamamoto M, Complete agenesis of the dorsal pancreas: J Hepatobiliary Pancreat Surg, 1999; 6(1); 94-97
6.. Ulusan S, Yakar T, Koc Z, Adenocarcinoma of the pancreas associated with dorsal agenesis: Pancreas, 2006; 33(4); 437-39
7.. Kapoor A, Singh R, Periampullary carcinoma in a patient with agenesis of dorsal pancreas: J Surg Case Rep, 2011; 2011(9); 4
8.. Low JP, Williams D, Chaganti JR, Polysplenia syndrome with agenesis of the dorsal pancreas and preduodenal portal vein presenting with obstructive jaundice – a case report and literature review: Br J Radiol, 2011; 84(1007); e217-20
9.. Dumitraşcu T, Scarlat A, Diaconescu A, Ionescu M, Dorsal pancreas agenesis and ductal adenocarcinoma: Surgical implications of an extremely rare association: Chirurgia (Bucur), 2012; 107(3); 389-92
10.. Mistry JH, Yadav A, Nundy S, Ampullary carcinoma in a patient with agenesis of the dorsal pancreas: A case report: Indian J Surg, 2015; 77(Suppl. 1); 32-34
11.. Sannappa RM, Buragohain J, Sarma D, Agenesis of dorsal pancreas associated with periampullary pancreaticobiliary type adenocarcinoma: JOP, 2014; 15(5); 489-92
12.. Deignan RW, Nizzero A, Malone DE, Case report: Agenesis of the dorsal pancreas: A cause of diagnostic error on abdominal sonography: Clin Radiol, 1996; 51(2); 145-47
13.. Lal H, Yadav P, Mourya C, Dependent stomach sign and dependent intestine sign of dorsal pancreatic agenesis: Abdom Radiol (NY), 2017; 42(2); 667-69
14.. Thakur S, Jhobta A, Sharma D, Thakur CS, MR in complete dorsal pancreatic agenesis: Case report and review of literature: Indian J Radiol Imaging, 2014; 24(2); 156-59
15.. Jeong JH, Kim GH, Song GA, Polysplenia syndrome with congenital agenesis of dorsal pancreas presenting as acute pancreatitis and the role of endoscopic ultrasonography in its diagnosis: Korean J Gastroenterol, 2012; 60(1); 47-51
16.. Malak M, Masuda D, Ogura T, Yield of endoscopic ultrasound-guided fine needle aspiration and endoscopic retrograde cholangiopancreatography for solid pancreatic neoplasms: Scand J Gastroenterol, 2016; 51(3); 360-67
17.. Saber AA, Boros MJ, Chilaiditi’s syndrome: What should every surgeon know?: Am Surg, 2005; 71(3); 261-63
18.. Wildling R, Schnedl WJ, Reisinger EC, Agenesis of the dorsal pancreas in a woman with diabetes mellitus and in both of her sons: Gastroenterology, 1993; 104(4); 1182-86
19.. Klein WA, Dabezies MA, Friedman AC, Agenesis of dorsal pancreas in a patient with weight loss and diabetes mellitus: Dig Dis Sci, 1994; 39(8); 1708-13
20.. Liang K, Ou X, Huang X, Lan Q, Agenesis of the dorsal pancreas: a rare cause of insulin-dependent diabetes without abdominal pain: Case report: Medicine (Baltimore), 2018; 97(9); e0046
21.. Lalchandani A, Maurya A, Rizvi SFM, Yadav A, Agenesis of the dorsal pancreas: A rare cause of diabetes and recurrent upper abdominal pain: Cureus, 2023; 15(2); e34689
22.. Lång K, Lasson A, Müller MF, Dorsal agenesis of the pancreas – a rare cause of abdominal pain and insulin-dependent diabetes: Acta Radiol, 2012; 53(1); 2-4
23.. Maier M, Wiesner W, Mengiardi B, Annular pancreas and agenesis of the dorsal pancreas in a patient with polysplenia syndrome: Am J Roentgenol, 2007; 188(2); W150-53
24.. Herman TE, Siegel MJ, Polysplenia syndrome with congenital short pancreas: Am J Roentgenol, 1991; 156(4); 799-800
25.. Soler R, Rodríguez E, Comesaña ML, Agenesis of the dorsal pancreas with polysplenia syndrome: CT features: J Comput Assist Tomogr, 1992; 16(6); 921-23
26.. Mahey S, Chawla AS, Agenesis of dorsal pancreas with chronic calcific pancreatitis: The head without a body: Pancreas, 2022; 51(5); e80-e82
27.. Xia LZ, Bu XF, Jiang PC, Agenesis of the dorsal pancreas with chronic suppurative pancreatitis: Case report and literature review: Medicine (Baltimore), 2021; 100(49); e28137
28.. Bretagne JF, Darnault P, Raoul JL, Calcifying pancreatitis of a congenital short pancreas: A case report with successful endoscopic papillotomy: Am J Gastroenterol, 1987; 82(12); 1314-17
29.. Oldenburg B, van Leeuwen MS, van Berge Henegouwen GP, Pancreatitis and agenesis of the dorsal pancreas: Eur J Gastroenterol Hepatol, 1998; 10(10); 887-89
30.. Rittenhouse DW, Kennedy EP, Mascaro AA, The novel triad of dorsal agenesis of the pancreas with concurrent pancreatic ductal adenocarcinoma and nonalcoholic chronic calcific pancreatitis: A case series and review of the literature: J Gastrointest Surg, 2011; 15(9); 1643-49
31.. Ulusan S, Bal N, Kizilkilic O, Case report: Solid-pseudopapillary tumour of the pancreas associated with dorsal agenesis: Br J Radiol, 2005; 78(929); 441-43
32.. Rodrigues P, Oliveira RC, Oliveira CM, Neuroendocrine tumour in pancreatic dorsal agenesis: A rare association: BMJ Case Rep, 2017; 2017 bcr201722
33.. Saikaly E, El Asmar A, Abi Fadel F, Agenesis of the dorsal pancreas associated with mucinous adenocarcinoma and cystic teratoma: A case report and literature review: Clin Case Rep, 2017; 5(2); 175-81
34.. Erotokritou A, Gerharz CD, Sagir A, Agenesis of dorsal pancreas associated with pancreatic neuroendocrine tumor: A case report and review of the literature: J Med Case Rep, 2018; 12(1); 185
35.. Nakamura Y, Egami K, Maeda S, Solid and papillary tumor of the pancreas complicating agenesis of the dorsal pancreas: J Hepatobiliary Pancreat Surg, 2001; 8(5); 485-89
36.. Nonent M, Linard J, Lévèque E, Dorsal pancreas agenesis: Computed tomography appearance with three-dimensional volume rendering reconstruction: Surg Radiol Anat, 2003; 25(2); 161-63
37.. Otani T, Shioiri T, Mishima H, Bile duct schwannoma developed in the remnant choledochal cyst – a case associated with total agenesis of the dorsal pancreas: Dig Liver Dis, 2005; 37(9); 705-8
38.. Sakpal SV, Sexcius L, Babel N, Agenesis of the dorsal pancreas and its association with pancreatic tumors: Pancreas, 2009; 38(4); 367-73
39.. Namikawa T, Utsunomiya M, Yokota K, Laparoscopic total gastrectomy for concurrent gastric cancer and complete agenesis of the dorsal pancreas: Asian J Endosc Surg, 2023; 16(2); 266-70
40.. Shyr BS, Wang SE, Chen SC, Pancreatic head sparing surgery for solid pseudopapillary tumor in patients with agenesis of the dorsal pancreas: J Chin Med Assoc, 2022; 85(10); 981-86
41.. Pasaoglu L, Vural M, Hatipoglu HG, Agenesis of the dorsal pancreas: World J Gastroenterol, 2008; 14(18); 2915-16
42.. Jha N, Prasad U, Kumar D, The role of cross-sectional imaging in the diagnosis of agenesis of the dorsal pancreas: A case series: Cureus, 2023; 15(6); e40930
43.. Julianov AE, Saroglu AS, Pancreatic head cancer in a patient with complete agenesis of dorsal pancreas: Hepatobiliary Surg Nutr, 2019; 8(3); 327-28
44.. Kabnurkar R, Rokade ML, Bandekar K, Incidentally detected agenesis of dorsal pancreas on PET/CT: Case report and review of literature: Indian J Nucl Med, 2017; 32(1); 33-35
45.. Zhou Y, Chen M, Liu Y, Agenesis of dorsal pancreas confirmed by three-dimensional reconstruction CT: Int J Clin Exp Med, 2014; 7(9); 3110-12
46.. Montero-Macías R, Krief D, Villefranque V, Anatomy, embryology, and imaging of situs ambiguous with polysplenia and left IVC: Radiol Case Rep, 2023; 18(5); 1727-32
47.. Nassif S, Ponchiardi C, Sachs T, Pancreatic neuroendocrine tumor in the setting of dorsal agenesis of the pancreas: Case Rep Gastrointest Med, 2016; 2016; 380
48.. Elhattabi K, Elyamine O, Bouali M, Polysplenia with agenesis of the dorsal pancreas and preduodenal portal vein, about a case: Int J Surg Case Rep, 2020; 76; 357-60
49.. Di Masi A, Leboffe L, De Marinis E, Retinoic acid receptors: From molecular mechanisms to cancer therapy: Mol Aspects Med, 2015; 41; 1-115
50.. Martín M, Gallego-Llamas J, Ribes V, Dorsal pancreas agenesis in retinoic acid-deficient Raldh2 mutant mice: Dev Biol, 2005; 284(2); 399-411
51.. Brown G, Targeting the retinoic acid pathway to eradicate cancer stem cells: Int J Mol Sci, 2023; 24(3); 2373
52.. Brozzetti S, D’Alterio C, Bini S, Surgical resection is superior to TACE in the treatment of HCC in a well selected cohort of BCLC-B elderly patients – a retrospective observational study: Cancers (Basel), 2022; 14(18); 4422
53.. Di Carlo S, Cavallaro G, La Rovere F, Synchronous liver and peritoneal metastases from colorectal cancer: Is cytoreductive surgery and hyperthermic intraperitoneal chemotherapy combined with liver resection a feasible option?: Front Surg., 2022; 9; 1006591
Figures
Tables
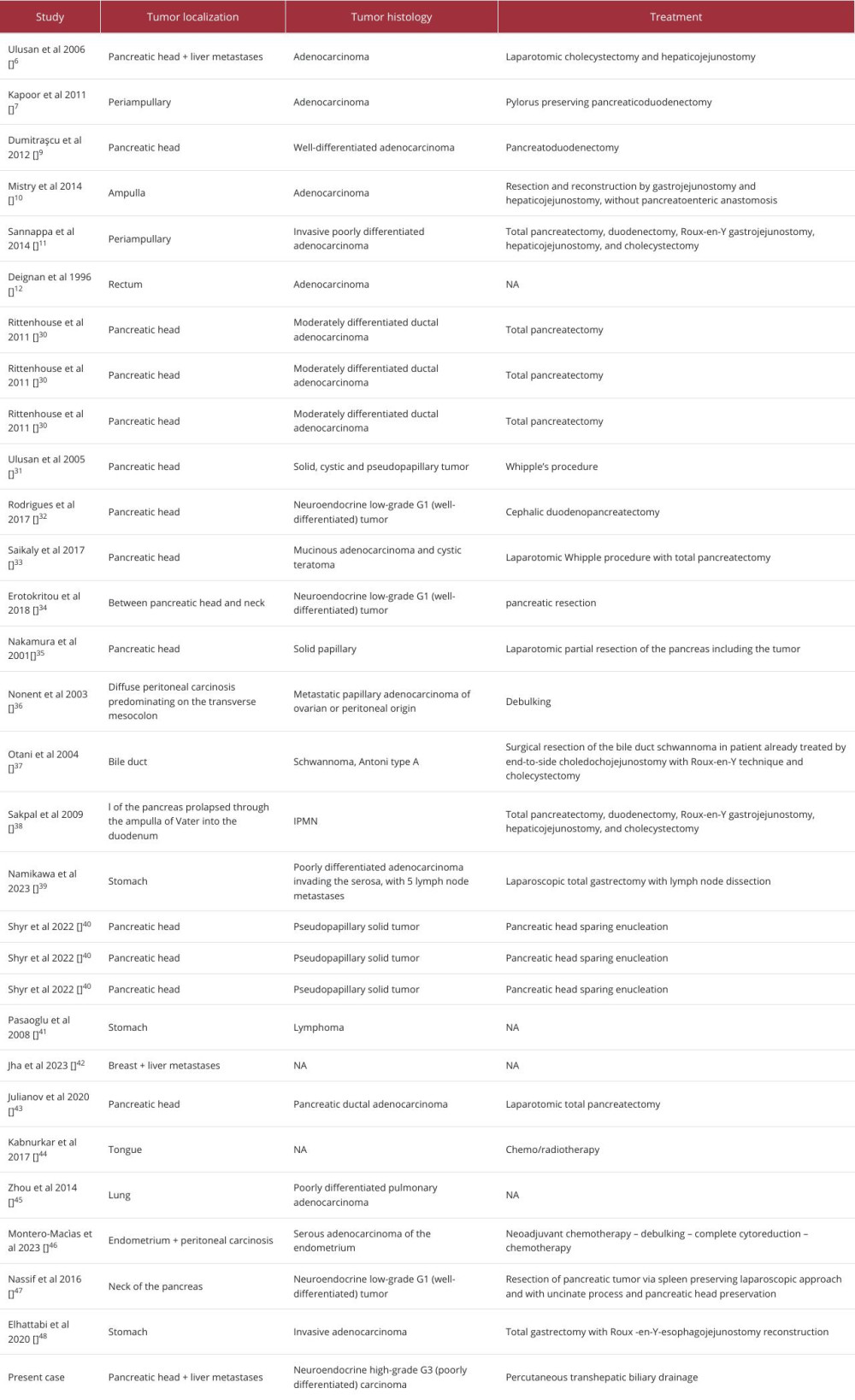 Table 1.. Studies reporting the association between agenesis of dorsal pancreas and neoplastic lesions of the pancreas or distal structures. NA, not available.Table 1.. Studies reporting the association between agenesis of dorsal pancreas and neoplastic lesions of the pancreas or distal structures. NA, not available.
Table 1.. Studies reporting the association between agenesis of dorsal pancreas and neoplastic lesions of the pancreas or distal structures. NA, not available.Table 1.. Studies reporting the association between agenesis of dorsal pancreas and neoplastic lesions of the pancreas or distal structures. NA, not available. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133