05 July 2025: Articles 
Whole-Genome Sequencing of Blood-Isolated Lactobacillus johnsonii in Thailand: Clinical Implications and Public Health Relevance
Challenging differential diagnosis, Management of emergency care, Rare disease
Arnon ChukamnerdDOI: 10.12659/AJCR.947564
Am J Case Rep 2025; 26:e947564






Abstract
BACKGROUND: Lactobacillus johnsonii is a probiotic bacterium commonly found in the gastrointestinal tracts of humans and other animals. It is non-pathogenic and plays a crucial role in maintaining gut health. L. johnsonii is often associated with beneficial effects on the host immune system and digestion. However, reports of L. johnsonii infections are rare, and their clinical characteristics remain poorly understood. This article reports a case of L. johnsonii isolated from a patient’s blood – the first such case documented in Thailand. Whole-genome sequencing (WGS) was performed on the isolate (LJ-PSU-blood) to investigate its genomic characteristics.
CASE REPORT: A 25-year-old Thai woman with a large abdominal mass was diagnosed with diffuse large B-cell lymphoma, and she was started on rituximab-cyclophosphamide, hydroxydaunorubicin, oncovin, and prednisolone chemotherapy. During her first rituximab infusion, she developed a fever, tachypnea, and tachycardia. Her blood cultures revealed an organism after 1 day. L. johnsonii was initially identified and subjected to WGS, and the sequence data were analyzed using bioinformatics tools. The findings demonstrated that the LJ-PSU-blood isolate possessed antibiotic resistance and virulence-associated genes. In addition, this isolate harbored bacteriocin-encoding genes and integrated bacteriophage sequences. Our genome was compared with 21 published genomes from various countries, hosts, and isolation sources. They were grouped into 3 monophyletic clades based on single-nucleotide polymorphism distances.
CONCLUSIONS: This case report describes the characteristics of L. johnsonii isolated from the blood of a Thai patient. Clinical and WGS data highlight important public health concerns associated with L. johnsonii infections.
Keywords: Blood, Genome, Bacterial, Lactobacillus johnsonii, Sequence Analysis, DNA, Virulence Factors, Humans, Female, Thailand, Whole Genome Sequencing, adult, Lactobacillus, Public Health, Gram-Positive Bacterial Infections
Introduction
Recently, the genomes of
Detailed genomic analysis is essential in unraveling the genomic makeup of
Case Report
CLINICAL DATA:
A 25-year-old previously healthy Thai woman presented with a month-old large abdominal mass and diffuse abdominal pain. Physical examination revealed multiple generalized lymphadenopathies and an abdominal mass 18 cm in diameter. She was admitted to Songklanagarind Hospital for an ultrasound-guided percutaneous abdominal mass biopsy. Histopathology examination revealed diffuse large B-cell lymphoma (DLBCL), and chemotherapy with the rituximab-cyclophosphamide, hydroxydaunorubicin, oncovin, and prednisolone (R-CHOP) regimen was planned as the definitive treatment. Her initial laboratory results, including anti-HIV, HBsAg, anti-HBc Ab, and anti-HCV, were all negative. She also reported regular consumption of yogurt containing
On day 8 of admission, coinciding with the first day of rituximab infusion, the patient became febrile, tachypneic, and tachycardic. She had confusion, a body temperature of 37.9°C, pulse rate of 112 beats per minute, respiratory rate of 24 breaths per minute, blood pressure of 102/67 mmHg, and oxygen saturation of 94% on room air. The fever was intermittent and of moderate grade. No other organ-specific signs or symptoms were present. Laboratory results revealed leukocytosis with a white blood cell count of 18,740 cells/mm3 (neutrophils 77%, bands 14%, lymphocytes 4%), hemoglobin of 8 g/dL, and platelet count of 272,000/μL. Blood chemistry showed a serum creatinine of 0.55 mg/dL, total bilirubin of 2.69 mg/dL, AST of 112 U/L, ALT of 27 U/L, and ALP of 259 U/L. Rituximab infusion was discontinued due to suspicion of sepsis or a rituximab infusion reaction. Two aerobic blood cultures were obtained, and the organism was detected after 1 day of incubation using an automated blood culture system. Gram staining revealed gram-positive bacilli, identified as L. johnsonii by matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) (Bruker Microflex®, BD, New Jersey, U.S.) with high-confidence identification (highest score value 2.218). No other bacteria were present in significant amounts. A computed tomography (CT) scan of the chest, abdomen, and pelvis did not reveal any source of bacteremia, except for the numerous enlarged cervical, axillary, and intra-abdominal nodes due to lymphoma. Transthoracic echocardiography showed a normal left ventricular ejection fraction (62%) with no valvular abnormalities or vegetations. Antimicrobial susceptibility testing was performed using a commercial broth microdilution method (Sensititre™ Gram Positive MIC Plate, Thermo Fisher Scientific, Inc., Massachusetts, U.S.). Interpretative criteria were based on the Clinical and Laboratory Standards Institute (CLSI) breakpoints for Lactobacillus spp. (Table 1). Empirical antibiotic therapy comprised ampicillin and gentamicin, which were later changed to vancomycin, based on the susceptibility results.
On day 11 of admission (72 hours after antibiotic initiation), the patient’s fever resolved. Repeat blood cultures were negative. She received an 8-day course of antibiotic therapy, and no recurrence of
On day 17 of admission, she developed coffee ground emesis, passing melena, and hemorrhagic shock. She developed dyspnea, became confused, and was intubated. Emergency esophagogastroduodenoscopy revealed circumferential ulcer nodular lesions along the upper to lower esophagus, focal mucosal thickening with redness in the upper corpus of the stomach, and diffuse circumferential mucosal nodularity along the first to third parts of the duodenum. Multiple biopsies of the esophagus, stomach, and duodenum were performed. Histopathology results showed non-specific ulcers in the esophagus and stomach and DLBCL involvement in the duodenum.
On day 20 of admission, the R-CHOP chemotherapy regimen was reinitiated after stabilization and completion of antibiotic therapy, with no evidence of ongoing gastrointestinal bleeding. However, 2 days later, she developed pneumonia and septicemia caused by multidrug-resistant
GENOMIC DNA EXTRACTION AND WHOLE-GENOME SEQUENCING:
The genomic DNA of
GENOME ASSEMBLY, GENOME ANNOTATION, AND SEQUENCE ANALYSIS:
The sequence reads were de novo assembled and annotated using SPAdes v3.15.5 [18] and Prokka v1.14.6 [19]. After identifying the species using MALDI-TOF MS and 16S rRNA sequencing, the L. johnsonii strain was confirmed using KmerFinder v3.2 [20,21]. ARGs, plasmids, and VAGs were identified using ResFinder v4.1 [22,23] and PlasmidFinder v2.1 [23,24] in the Center for Genomic Epidemiology and VFanalyzer v1.0.0 in the virulence factor Database [25]. The bacteriocin-encoding genes were detected using BAGEL4 v1.2 [26], while integrated bacteriophage sequences (IBSs) were searched using PHASTER v1.0.0 [27]. In comparative genomics, the core gene alignment of our studied genome and the public genomes selected from the National Center for Biotechnology Information (NCBI) database (Table 2) was obtained from Roary v3.13.0, the pan-genome pipeline [28]. The single-nucleotide polymorphisms (SNPs) were called using snp-sites v2.5.1 [29], and then an SNP-based phylogenetic tree was generated using Geneious Tree Builder in Geneious Prime software R10 with a selection of the neighbor-joining method and 1000 replicates [30].
The WGS results demonstrated that the L. johnsonii LJ-PSU-blood genome had a 1,910,935 bp genome length and 34.37% GC content. The N50 value and the number of contigs were 136,766 bp and 37, respectively. For downstream analysis, the tet(W) gene conferring tetracycline resistance was identified in this isolate. Notably, 16 VAGs were detected in the isolate, as shown in Table 3. These VAGs encode several virulence factors, including adherence, other adhesion-related proteins, enzymes, immune evasion, regulation, antiphagocytosis, bile resistance, cell surface components, proteases, surface protein anchoring, and toxins. In addition, the genes encoding pediocin, lactacin-F_subunit_lafA, and helveticin-J were found in this isolate. The most common IBSs, such as Lactobacillus, Listeria, Streptococcus, and Oenococcus phages, were also detected in the isolate.
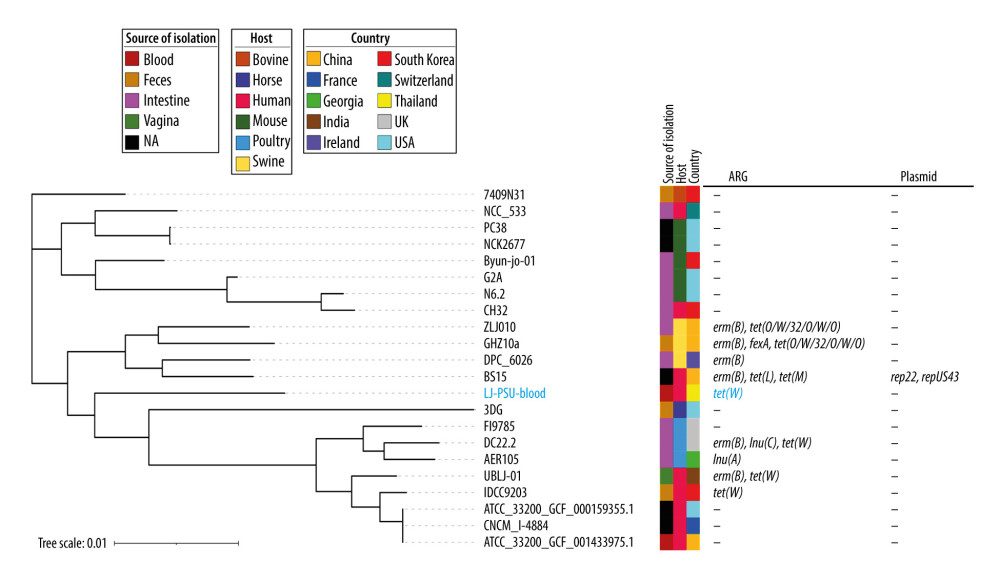
In the comparative genomic analysis, most isolates were collected from animal intestines, especially mice and poultry. Of the 22 isolates, 9 harbored at least 1 ARG. The erm(B) and tet genes, which confer macrolide and tetracycline resistance, were found at high frequencies. Moreover, 2 plasmid markers were identified in the BS15 isolate collected from humans in China. An SNP-based phylogenetic tree revealed 3 monophyletic clades among the 22 included genomes, as illustrated in Figure 1. The LJ-PSU-blood isolate clustered within the largest clade, which included other isolates carrying antimicrobial resistance genes and plasmid markers, whereas neither of these was detected in the other 2 clades.
Discussion
This report describes the first case of
The
To better understand the pathogenic potential and strain characteristics of
A comparative genomic analysis revealed that macrolide- and tetracycline-resistance genes are commonly present in
Conclusions
This case report reveals the clinical and genomic characteristics of
References
1. Quinto EJ, Jiménez P, Caro I, Probiotic lactic acid bacteria: A review: Food Nutr Sci, 2014; 5(18); 1765
2. Mann E, Schmitz-Esser S, Zebeli Q, Mucosa-associated bacterial microbiome of the gastrointestinal tract of weaned pigs and dynamics linked to dietary calcium-phosphorus: PLoS One, 2014; 9(1); e86950
3. Fernández S, Fraga M, Silveyra E: Benef Microbes, 2018; 9(4); 613-24
4. Davoren MJ, Liu J, Castellanos J: Gut Microbes, 2019; 10(4); 458-80
5. Lee SH, Yang EH, Kwon HS: Microbiol Biotechnol Lett, 2008; 36(2); 121-27
6. Huang R, Wu F, Zhou Q, Lactobacillus and intestinal diseases: Mechanisms of action and clinical applications: Microbiol Res, 2022; 260; 127019
7. Sharma A, Das P, Buschmann M, The future of microbiome-based therapeutics in clinical applications: Clin Pharmacol Ther, 2020; 107(1); 123-28
8. Bereswill S, Ekmekciu I, Escher U: Sci Rep, 2017; 7(1); 2138
9. Aiba Y, Ishikawa H, Tokunaga M: FEMS Microbiol Lett, 2017; 364(11); fnx102
10. Chen S, Li y, Chu B: Microorganisms, 2021; 9(9); 1983
11. Wang H, Ni X, Liu L: Lipids Health Dis, 2017; 16(1); 1-10
12. Rossi F, Amadoro C, Colavita G: Microorganisms, 2019; 7(5); 126
13. Kullar R, Goldstein EJ, Johnson S: Microorganisms, 2023; 11(4); 896
14. Boekhorst J, Siezen RJ, Zwahlen MC: Microbiology, 2004; 150(11); 3601-11
15. Zhang W, Wang J, Zhang D: Front Genet, 2019; 10; 812
16. Vazquez-Munoz R, Thompson A, Russell JT: Front Microbiol, 2022; 13; 853762
17. Boucard AS, Florent I, Polack B: Microorganisms, 2022; 10(2); 273
18. Bankevich A, Nurk S, Antipov D, SPAdes: A new genome assembly algorithm and its applications to single-cell sequencing: J Comput Biol, 2012; 19(5); 455-77
19. Seemann T, Prokka: Rapid prokaryotic genome annotation: Bioinformatics, 2014; 30(14); 2068-69
20. Clausen PT, Aarestrup FM, Lund O, Rapid and precise alignment of raw reads against redundant databases with KMA: BMC Bioinform, 2018; 19(1); 307
21. Larsen MV, Cosentino S, Lukjancenko O, Benchmarking of methods for genomic taxonomy: J Clin Microbiol, 2014; 52(5); 1529-39
22. Bortolaia V, Kaas RS, Ruppe E, ResFinder 4.0 for predictions of phenotypes from genotypes: J Antimicrob Chemother, 2020; 75(12); 3491-500
23. Camacho C, Coulouris G, Avagyan V, BLAST+: Architecture and applications: BMC Bioinform, 2009; 10(1); 421
24. Carattoli A, Zankari E, Garcìa-Fernandez A, PlasmidFinder and pMLST: In silico detection and typing of plasmids: Antimicrob Agents Chemother, 2014; 58(7); 3895-903
25. Liu B, Zheng D, Zhou S, VFDB 2022: A general classification scheme for bacterial virulence factors: Nucleic Acids Res, 2022; 50(D1); D912-D17
26. Jong A, Hijum SA, Bijlsma JJ, BAGEL: A web-based bacteriocin genome mining tool: Nucleic Acids Res, 2006; 34(Suppl 2); W273-W79
27. Arndt D, Grant JR, Marcu A, PHASTER: A better, faster version of the PHAST phage search tool: Nucleic Acids Res, 2016; 44(W1); W16-W21
28. Page AJ, Cummins CA, Hunt M, Roary: Rapid large-scale prokaryote pan genome analysis: Bioinformatics, 2015; 31(22); 3691-93
29. Page AJ, Taylor B, Delaney AJ, SNP-sites: Rapid efficient extraction of SNPs from multi-FASTA alignments: Microb Genom, 2016; 2(4); e000056
30. Kearse M, Moir R, Wilson A, Geneious Basic: An integrated and extendable desktop software platform for the organization and analysis of sequence data: Bioinformatics, 2012; 28(12); 1647-49
31. Péchiné S, Hennequin C, Boursier C: PLoS One, 2013; 8(11); e81112
32. Begley M, Sleator RD, Gahan CG: Infect Immun, 2005; 73(2); 894-904
33. Burkholder KM, Bhunia AK: Infect Immun, 2010; 78(12); 5062-73
34. Kadioglu A, Taylor S, Iannelli F: Infect Immun, 2002; 70(6); 2886-90
35. Gao XY, Zhi XY, Li HW: PLoS One, 2014; 9(6); e101229
36. Kalscheuer R, Weinrick B, Veeraraghavan U: Proc Natl Acad Sci USA, 2010; 107(50); 21761-66
37. Bogaerts B, Fraiture MA, Huwaert A: Front Microbiol, 2023; 14; 1173594
38. Nakhamchik A, Wilde C, Chong H, Evidence for the horizontal transfer of an unusual capsular polysaccharide biosynthesis locus in marine bacteria: Infect Immun, 2010; 78(12); 5214-22
39. Shankar N, Coburn P, Pillar C, Enterococcal cytolysin: Activities and association with other virulence traits in a pathogenicity island: Int J Med Microbiol, 2004; 293(7–8); 609-18
40. Yu Y, Wang J, Han R: Virulence, 2020; 11(1); 1059-74
41. Soucy SM, Huang J, Gogarten JP, Horizontal gene transfer: Building the web of life: Nat Rev Genet, 2015; 16(8); 472-82
42. Zhao M, Li Y, Zhang Y: Front Microbiol, 2024; 15; 1437036
43. Chevallereau A, Pons BJ, Houte S, Interactions between bacterial and phage communities in natural environments: Nat Rev Microbiol, 2022; 20(1); 49-62
Tables
 Table 1. Susceptibility breakpoints for Lactobacillus spp.
Table 1. Susceptibility breakpoints for Lactobacillus spp. Table 2. Information for 21 selected public genomes from the NCBI database.
Table 2. Information for 21 selected public genomes from the NCBI database. Table 3. Virulence factors (VFs) in an L. johnsonii LJ-PSU-blood isolate.Table 1. Susceptibility breakpoints for Lactobacillus spp.Table 2. Information for 21 selected public genomes from the NCBI database.Table 3. Virulence factors (VFs) in an L. johnsonii LJ-PSU-blood isolate.
Table 3. Virulence factors (VFs) in an L. johnsonii LJ-PSU-blood isolate.Table 1. Susceptibility breakpoints for Lactobacillus spp.Table 2. Information for 21 selected public genomes from the NCBI database.Table 3. Virulence factors (VFs) in an L. johnsonii LJ-PSU-blood isolate. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133