26 May 2025: Articles 
Neurological and Cardiac Adverse Events in Cervical Cancer Treatment: A Case of Postoperative Sintilimab-Induced Encephalitis and Myocarditis
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Rare disease, Adverse events of drug therapy, Educational Purpose (only if useful for a systematic review or synthesis)
Haiyu Guo BCDEF 1, Huanlei Wu ACE 1, Jun Li BD 1, Ruichao Li ABE 1*DOI: 10.12659/AJCR.947730
Am J Case Rep 2025; 26:e947730






Abstract
BACKGROUND: Immune checkpoint inhibitors (ICIs) have shown considerable promise in enhancing patient outcomes and improving survival rates, offering a new frontier in cancer treatment. As a result, their use in clinical practice has become more widespread. However, the adverse effects associated with ICIs can compromise treatment efficacy. Among these, immune-related neurological adverse events are relatively uncommon, with an incidence rate of approximately 17%. Central nervous system (CNS) symptoms, although less frequent (around 6%), are particularly concerning due to their higher risk compared to peripheral nervous system involvement. Additionally, in recent years, the incidence of cardiac toxicity has been increasing, often indicated by elevated cardiac biomarkers, but most cases are asymptomatic.
CASE REPORT: This report presents a case of a middle-aged woman with cervical cancer who developed both encephalitis and myocarditis during postoperative consolidation therapy with an immune checkpoint inhibitor. A thorough evaluation, including laboratory tests, imaging studies, and an assessment of the patient’s medical history and clinical presentation, excluded infection and paraneoplastic encephalitis as potential causes. She was treated with high-dose corticosteroids and intravenous immunoglobulin (IVIG), resulting in gradual resolution of her central nervous system symptoms and normalization of cardiac biomarkers.
CONCLUSIONS: Although the incidences of immune-related encephalitis and myocarditis are generally low, they can be very severe. With the increasing use of ICIs in clinical practice, the incidence of immune-related neurological symptoms may rise. This highlights the need for increased vigilance in clinical applications, including early preventive measures and prompt diagnosis and treatment to mitigate the adverse effects of these therapies, thereby maximizing patient benefits.
Keywords: Encephalitis, Arbovirus, myocarditis, Neoplasms, Uterine Cervical Neoplasms, Humans, Female, Middle Aged, Immune Checkpoint Inhibitors, Antibodies, Monoclonal, Humanized, Encephalitis, Postoperative Complications, Antineoplastic Agents, Immunological
Introduction
ICIs have made groundbreaking advancements in cancer treatment, significantly extending overall survival and greatly enhancing patient prognosis. Their efficacy is even more pronounced when combined with other antitumor agents. Tumor cells can evade the normal immune system, primarily through the expression of PD-L1 on their surfaces, which binds to PD-1 on T cells. This interaction delivers negative regulatory signals to T cells, inhibiting their activation and proliferation while promoting apoptosis, thereby facilitating “immune escape” from immune-mediated destruction [1]. Under normal circumstances, T cells express PD-1 and healthy tissue cells express PD-L1. The binding of PD-1 to PD-L1 downregulates the immune response against normal cells, maintaining immune homeostasis and preventing autoimmune diseases. ICIs counteract this mechanism, restoring T cells’ ability to attack tumor cells. However, this can also lead to the immune system targeting normal cells, which is a major mechanism behind the adverse reactions associated with these inhibitors [2–5]. Immune-related adverse reactions can affect various organs and tissues throughout the body [3], and their onset is unpredictable, potentially occurring during treatment or months to years afterward [6].
Sintilimab is a recombinant, fully human IgG4 antibody that blocks programmed cell death protein 1 (PD-1). It has demonstrated promising therapeutic efficacy in various malignancies, including Hodgkin lymphoma, non-small cell lung cancer, liver cancer, and esophageal squamous cell carcinoma [7–11]. Although this class of ICIs significantly improves patient prognosis, they can also induce immune-related adverse reactions. These include skin toxicity, pulmonary toxicity, endocrine dysfunction, hepatic and renal impairment, pancreatitis, gastrointestinal inflammation, cardiac toxicity, and neurological toxicity [5,12–15]. Among these, neurological symptoms are less common and have a lower incidence compared to other adverse effects; however, they pose considerable risks and can severely impact patients’ quality of life, with potentially fatal outcomes [3,16,17]. According to the prescribing information for sintilimab, the overall incidence of immune-related neurological adverse reactions is reported at 0.4%, with the most severe central nervous system toxicity occurring at a rate of 0.1%.
This article reports a case of a cervical cancer patient undergoing postoperative adjuvant therapy with sintilimab, who shortly after treatment developed immune-related encephalitis accompanied by myocarditis. Through a process of exclusionary diagnosis and empirical treatment with immunosuppressive agents, the patient’s neurological symptoms greatly improved. This suggests a correlation between the onset of encephalitis and the use of ICIs. Given the diverse symptomatology associated with immune-related encephalitis, this case also serves as a reference for the clinical manifestations of encephalitis induced by ICIs.
Case Report
We report the case of a middle-aged woman postoperatively diagnosed with stage IIA1 cervical cancer based on pathological findings. She had a history of good health, with no neurological disorders, hypertension, hyperlipidemia, or heart disease, and no history of unhealthy lifestyle habits.
She began experiencing contact vaginal bleeding in January 2023 and visited a local hospital in early March. After undergoing transvaginal ultrasound, MRI, discharge smear, and diagnostic curettage, she was diagnosed with cervical squamous cell carcinoma. In mid-March, she sought further treatment at our gynecology clinic. After laboratory and imaging examinations were conducted to rule out surgical contraindications, she underwent laparoscopic radical hysterectomy, bilateral adnexectomy, and pelvic lymphadenectomy under general anesthesia on March 23. The postoperative pathological examination revealed cervical cancer characterized as HPV-associated squamous cell carcinoma with a histological grade of moderately-to-poorly differentiated. The maximum tumor diameter was not measurable, and the depth of invasion was approximately 5 mm, extending into the inner one-third of the fibromuscular stroma. There was no definitive evidence of tumor invasion into the lower uterine segment, vaginal wall, bilateral round ligaments, bilateral broad ligaments, bilateral parametrial tissues, bilateral fallopian tubes, or bilateral ovaries. Lymphovascular invasion (LVI) was not observed. No metastatic carcinoma was identified in 12 left pelvic lymph nodes and 19 right pelvic lymph nodes. Immunohistochemical analysis showed positivity for PCK, CK5/6, P63, P40, and P16, with a Ki-67 labeling index of approximately 80%. Molecular testing for EBER was negative. Additional findings included uterine leiomyoma, proliferative-phase endometrial glands, bilateral chronic salpingitis, and no significant pathological abnormalities in both ovaries under microscopy. Based on the histopathological analysis indicating a moderately-to-poorly differentiated tumor with a high proliferation index of 80%, which is significant risk factor, she was advised by the surgical team to receive adjuvant therapy. On the 45th day after surgery, she began treatment with a TP+PD-1 regimen (sintilimab, nedaplatin, and paclitaxel) with the specific dosing schedule of 126 mg/m2 sintilimab and 152 mg/m2 paclitaxel on day 1 and 63 mg/m2 nedaplatin on day 2. On June 1, 2023, she had sudden onset of slurred speech and dysphagia at home after completing 1 cycle of chemotherapy. Over the following 2 days, her condition deteriorated rapidly, with a marked progression of symptoms. Due to her symptoms, she visited the otolaryngology and neurology outpatient clinics. Then, an ear, nose, and throat examination indicated pharyngitis, and the external hospital performed CT and MRI of the head to rule out intracranial bleeding and cerebral infarction. On June 12, 2023, she subsequently presented to our department for further evaluation and treatment (Figure 1). Routine cerebrospinal fluid (CSF) analysis revealed a nucleated cell count of 2×106/L, with no significant abnormalities (Table 1). Biochemical analysis showed a mild elevation in glucose (4.12 mmol/L) and lactate (2.80 mmol/L), while protein and chloride levels were normal (Table 1). CSF smear revealed lymphocytes and monocytes (Figure 2). Blood cultures for bacteria and fungi were negative, and PCR for viral nucleic acids in the CSF was also negative (Table 1). Rheumatological screening and CSF anti-neuronal antibody tests were both negative. Imaging follow-up with MRI of the head showed small punctate areas of high T1 and T2 signals in the bilateral frontal lobes and radiation crown, along with high signal on T2 FLAIR. Based on her symptoms and disease progression, combined with her medical history, medication history, as well as laboratory and imaging findings from both in-hospital and external evaluations, we sought to identify the underlying cause of the rapidly progressive neurological symptoms. Accordingly, our diagnostic team proposed several hypothetical diagnoses for thorough assessment. Meanwhile, additional relevant laboratory tests were conducted after her admission, revealing mildly elevated cardiac injury markers BNP (414.9 pg/ml), high-sensitivity cardiac troponin I (719.0 pg/ml), myoglobin (>1200.0 pg/ml), and creatine kinase isoenzyme (143.7 pg/ml). Electrocardiography showed sinus tachycardia and left anterior fascicular block, leading to suspicion of immune-related myocarditis, given her medical history. Laboratory tests showed elevated liver enzymes and decreased thyroid hormones.
These findings prompted us to consider the underlying cause of the simultaneous, rapid involvement of the neurological, hepatic, myocardial, and endocrine systems. Based on the above test results, the patient’s clinical symptoms, and their adjuvant therapy following cervical cancer surgery, there was a high suspicion of immune-related encephalitis. The patient was treated empirically with high doses of corticosteroids and IVIG. On the second day of admission, she received 500 mg of methylprednisolone sodium succinate and 20 g of immunoglobulin for 3 days. By the third day of treatment, liver function markers showed a reduction in ALT from 278 U/L to 155 U/L and AST from 285 U/L to 54 U/L. Cardiac biomarkers also improved, with cardiac troponin I decreasing from 747 pg/mL to 234.6 pg/mL and CK-MB levels dropping from 143.7 pg/mL to 23.7 pg/mL. On the fifth day, the corticosteroid dose was adjusted to 200 mg and was continued for 2 days. As she had significantly improved articulation and stronger swallowing ability compared to baseline, the medication was adjusted to 100 mg of corticosteroids plus 5 g of immunoglobulin for 5 days. On the 15th day, ALT and BNP levels had returned to normal, and cardiac troponin I decreased to 35.7 pg/mL, and she stopped using immunoglobulin, with corticosteroids alone maintained until day 22, when the dosage was adjusted to 60 mg intravenously for 2 days. Her central nervous symptoms notably improved, cardiac injury markers returned to normal ranges, liver enzymes gradually normalized, and thyroid function improved (Figures 3–5). After discharge, she was gradually weaned off corticosteroids and stopped receiving sintilimab, transitioning to chemotherapy combined with pelvic radiotherapy. The radiotherapy regimen included both external and internal pelvic irradiation. For external pelvic irradiation, a total dose of 4600 Gy over 23 fractions was delivered, with treatments scheduled 5 days per week. Cisplatin at 30 mg was administered intravenously once weekly to enhance tumor cell radiosensitivity and improve radiotherapy efficacy. Due to equipment limitations at the hospital, internal pelvic irradiation was administered following the completion of external irradiation, with a total dose of 600 Gy over 3 fractions. Based on the actual dose reduction and treatment effectiveness, the radiation source was changed to 0.5 cm submucosally in the cervical tissue. She underwent regular outpatient follow-ups during and after radiotherapy. No recurrence of neurological symptoms was observed, and electrocardiography and cardiac function evaluations showed normal results, indicating no residual neurological sequelae or cardiac damage. She currently remains in a stable disease phase.
Discussion
The advent of ICIs has considerably improved cancer treatment, exceedingly enhancing therapeutic efficacy, improving patient prognosis, and extending overall survival [13,15,18–21]. In clinical practice, the combination of ICIs with other anticancer agents has also demonstrated effective results, offering new opportunities for cancer treatment [2,18]. However, the mechanism of ICIs involves restoring the ability of immune cells to attack tumor cells while inhibiting the immune escape of tumors. Although this mechanism activates the normal cytotoxicity of T cells against tumor cells, it can also disrupt the body’s immune tolerance, leading T cells to mistakenly attack healthy tissues, thereby compromising the homeostasis of the immune system and resulting in development of immune-related diseases [2–4]. The occurrence of immune-related adverse events (irAEs) can significantly affect the efficacy of ICIs and patient prognosis [5]. Common irAEs include diarrhea, enteritis, hepatitis, renal impairment, myocarditis, thyroid dysfunction (eg, hypothyroidism and hyperthyroidism), adrenal insufficiency, rash, myositis, dry eyes, uveitis, interstitial pneumonia, and neurological toxicity [1,6,7,12,13,20,22]. Among these, the incidence of central nervous system toxicity is approximately 6%, with symptoms ranging from mild sensory disturbances to severe conditions such as encephalitis, myasthenia gravis, and Guillain-Barré syndrome, which can be life-threatening in severe cases [3,16,17,23].
In this case report, we describe the case of a middle-aged woman with cervical cancer who developed encephalitis after receiving adjuvant therapy with sintilimab following surgery. Initially, we suspected a central nervous system infection and conducted comprehensive laboratory tests, which ruled out bacterial and fungal infections. CSF biochemical analysis, routine testing, smears, and viral PCR testing of the CSF were all negative, excluding viral infections. Preoperative cranial CT showed no abnormal lesions, and her neurological symptoms began after the administration of ICIs, while paraneoplastic encephalitis usually presents earlier than tumor-related symptoms. Since paraneoplastic encephalitis does not respond well to corticosteroids and other immunosuppressants, we ruled out this diagnosis.
Further testing for neuronal autoantibodies (a panel of 7 antibodies) returned negative results, ruling out autoimmune encephalitis. As she was a middle-aged woman, a population with higher susceptibility to rheumatic diseases, we also considered rheumatologic causes. However, despite rheumatic disease-related encephalitis being rare as an initial presentation, a complete rheumatologic workup was performed, which returned negative results. She also received paclitaxel and nedaplatin as part of her adjuvant therapy, both of which can cause neurological symptoms, primarily peripheral neuropathy, such as numbness in the extremities. Additionally, chemotherapy-induced neurological symptoms typically appear later in the course of treatment [24]. We found no studies or case reports linking paclitaxel or platinum-based chemotherapy to central nervous system symptoms.
According to sintilimab’s prescribing information, the incidence of central nervous system toxicity is approximately 0.1%, with a median onset of 96 days; symptoms can appear as early as 19 days or as late as 108 days after treatment. In this case, the patient developed central nervous system symptoms 24 days after the start of therapy, which falls within this timeframe. After empirical treatment with high-dose corticosteroids and IVIG, her encephalitis symptoms gradually improved and returned to normal. Follow-up after discharge showed MRI results consistent with those from hospitalization, and no further neurological symptoms occurred outside the hospital. Therefore, we conclude that the encephalitis in this patient was associated with the use of sintilimab. This conclusion aligns with findings by Williams et al, who reported a correlation between encephalitis and ICIs [25]. Additionally, Zhang et al reported a similar case of a young female patient with small cell carcinoma of the fallopian tube who developed central nervous system symptoms after treatment with sintilimab [26].
Although our patient recovered from central nervous system symptoms after receiving corticosteroids and immunoglobulin therapy, leaving no neurological sequelae, the treatment regimen was adjusted to chemoradiotherapy maintenance after discontinuation of sintilimab, and no further neurological symptoms occurred. Currently, there is no research indicating whether continuing immune checkpoint inhibitor therapy after the resolution of neurological symptoms can lead to recurrence of the same symptoms or the development of new neurological problems. In a case report by Williams et al, a 60-year-old man with small cell lung cancer experienced partial tumor remission with ICIs but developed encephalitis on the fourth day of treatment, leading to discontinuation of ICIs, and he died from disease progression 19 weeks later [25]. This scenario highlights a critical concern in oncology treatment. As ICIs become more widely applied in clinical oncology, the incidence of immune-related encephalitis may increase, with potentially rising rates of occurrence. Thus, the benefit-risk profile of continuing ICIs for maintenance therapy in patients who have recovered from central nervous system symptoms warrants further research and evaluation.
As demonstrated in this case, we observed several clinical manifestations of immune-related encephalitis induced by ICIs, and found that damage to the central nervous system could be reversed with empirical treatment using high doses of corticosteroids combined with IVIG. Beyond corticosteroid therapy, additional immunosuppressive treatments, such as plasma exchange, IVIG, or rituximab, may be considered based on the severity of symptoms or when corticosteroid treatment is ineffective [27]. Therefore, when using ICIs in cancer treatment, the possibility of immune-related central nervous system toxicity should be anticipated. Preventive measures should be established, and prompt diagnosis and treatment should be implemented to achieve the best clinical outcomes while minimizing drug-related harm.
In the present case, a unique situation arose: while she was undergoing treatment with sintilimab, symptoms of immune-related encephalitis emerged. Upon admission and further examination, she was also diagnosed with immune-related myocarditis, immune-related hepatitis, and immune-related hypothyroidism. According to the prescribing information for sintilimab, the incidence of immune-related cardiotoxicity is approximately 0.5%. In our patient, while undergoing treatment with corticosteroids and IVIG, her myocardial injury markers gradually declined to normal levels, and an initial ECG showed mild myocardial damage, which subsequently resolved, as indicated by normal ECG findings during follow-up. Additional tests for autoimmune hepatitis antibodies were negative, and due to her medical history and administration of corticosteroids and liver-protective therapy during hospitalization, the abnormal markers had normalized by discharge. After discontinuing sintilimab and switching to radiotherapy and chemotherapy, periodic follow-up evaluations of these relevant markers revealed no further abnormalities, confirming that she had experienced multiple irAEs during postoperative sintilimab consolidation therapy for cervical cancer, including immune-related encephalitis, myocarditis, hepatitis, and hypothyroidism. Cases of extensive sintilimab use resulting in immune-related injuries affecting multiple organs and tissues are rare, and this report is, to the best of our knowledge, the first of its kind. This case offers valuable clinical insights into the use of sintilimab in management of malignant tumors, underscoring the importance of monitoring for irAEs involving multiple organs during immunotherapy.
In this case, the treatment for immune-related encephalitis involved high-dose intravenous methylprednisolone sodium succinate pulse therapy for 3 days. Compared to the previously reported regimens by Williams et al and Papadopoulos et al, which utilized 1000 mg/day of intravenous methylprednisolone for 5 consecutive days [25,28], we adjusted the dosage to 500 mg/day based on the patient’s condition and symptom improvement. Remarkably, she experienced significant relief of central nervous system symptoms within 2 days, accompanied by notable reductions in cardiac injury markers and liver enzymes (Figures 3–5).
Another notable aspect of this case is the administration of adjuvant immunotherapy following cervical cancer surgery. After surgical intervention, the attending surgeons may recommend adjuvant therapy combining chemotherapy and immunotherapy based on identification of 2 significant risk factors for tumor recurrence in the postoperative pathological assessment: moderately-to-poorly differentiated histology and an elevated proliferation index of 80%. Prior to establishing a definitive diagnosis, the patient sought medical evaluation and treatment across multiple departments after symptom onset. Ultimately, she was diagnosed and managed in our department. However, the decision to administer combined chemotherapy and immunotherapy as adjuvant treatment remains controversial based on the patient’s postoperative pathological staging and current clinical guidelines for cervical cancer management, as well as evidence from clinical trials. This therapeutic approach may be an overly aggressive treatment strategy, which could potentially explain the development of multiple irAEs in this case, including encephalitis, myocarditis, and thyroiditis.
Conclusions
As ICIs achieve remarkable success in cancer treatment, their clinical use has expanded substantially. In clinical practice, more emphasis must be placed on ensuring the safety of these drugs. Prevention is the most important measure, and it is essential to closely monitor for immune-related reactions that can occur during treatment. Treatment adjustments should be made based on the severity of symptoms and the patient’s overall condition. A thorough evaluation of the risks and benefits of continued treatment is necessary to optimize patient outcomes. Special attention should be given to any unexplained neurological symptoms during treatment, as immune-related encephalitis should be considered as a potential cause. Early intervention is key to reducing adverse effects, minimizing patient harm, and decreasing the occurrence of severe symptoms. Moreover, the standardized use of immunotherapy is an essential strategy for reducing the risk of irAEs in patients.
Figures
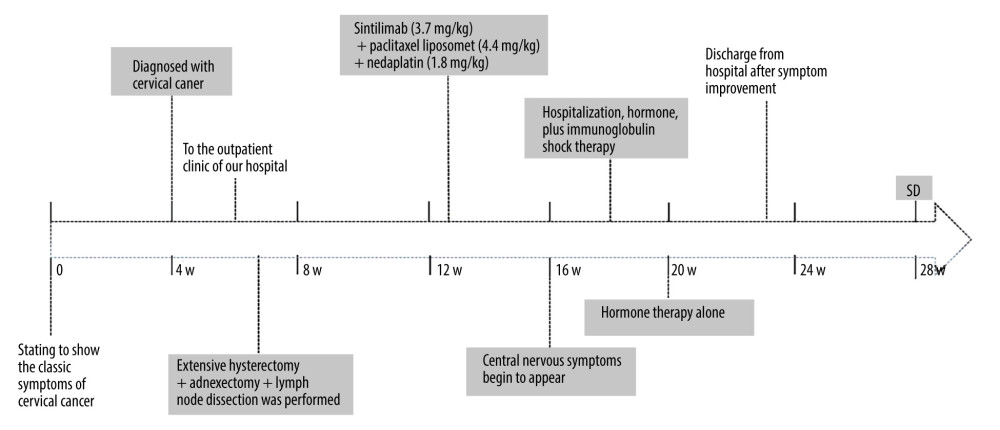 Figure 1. Timeline of the onset and treatment of immune-associated encephalitis caused by sintilimab.
Figure 1. Timeline of the onset and treatment of immune-associated encephalitis caused by sintilimab. 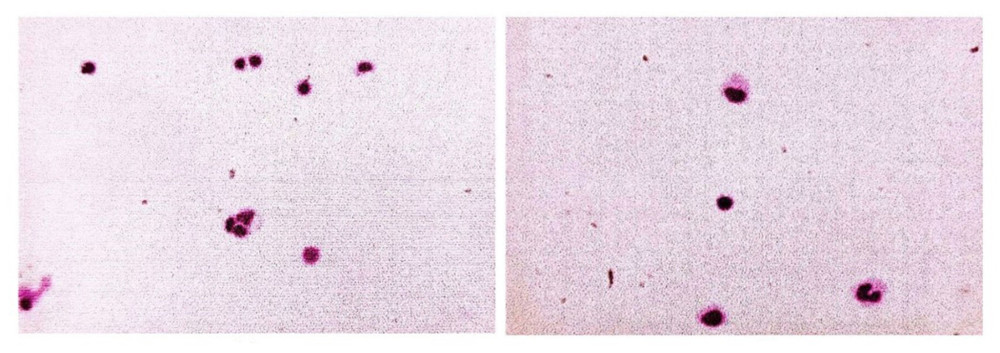 Figure 2. Results of cerebrospinal fluid smear under electron microscopy. Lymphocytes, monocytes, and occasional macrophages are seen under microscopy (cerebrospinal fluid).
Figure 2. Results of cerebrospinal fluid smear under electron microscopy. Lymphocytes, monocytes, and occasional macrophages are seen under microscopy (cerebrospinal fluid). 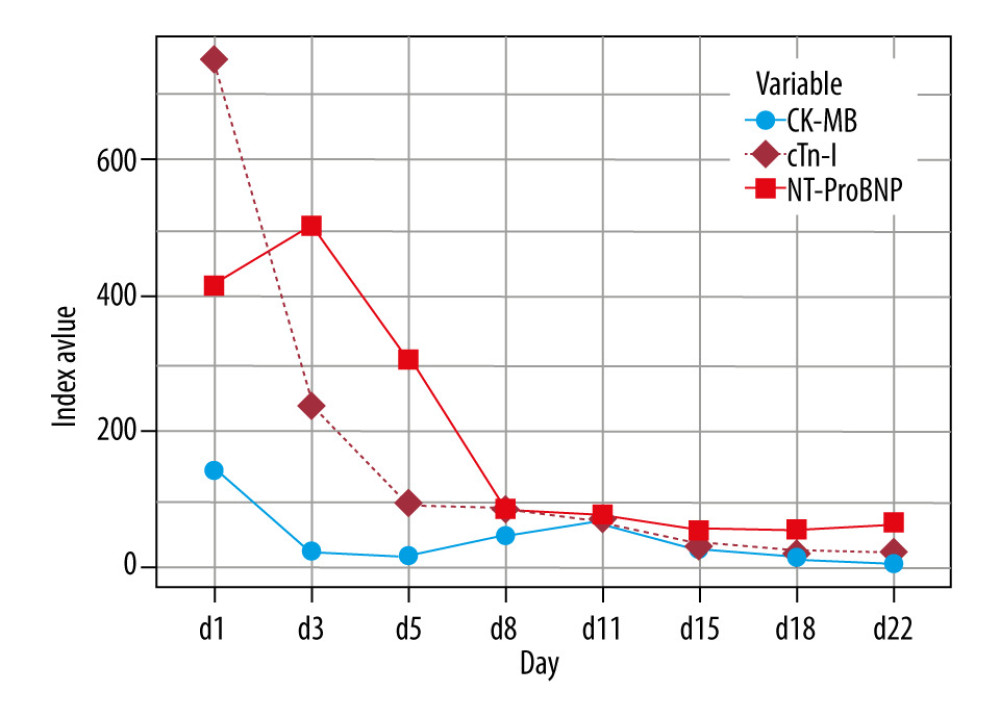 Figure 3. Trends of myocardial enzyme spectra.
Figure 3. Trends of myocardial enzyme spectra. 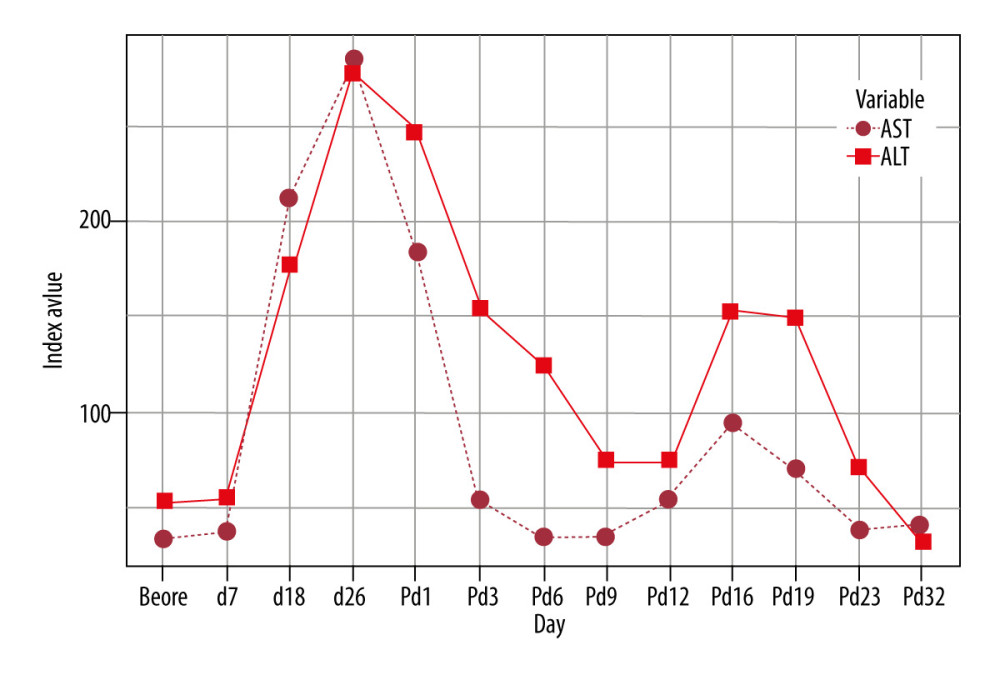 Figure 4. Trends of liver enzymes (P: post-treatment)
Figure 4. Trends of liver enzymes (P: post-treatment) 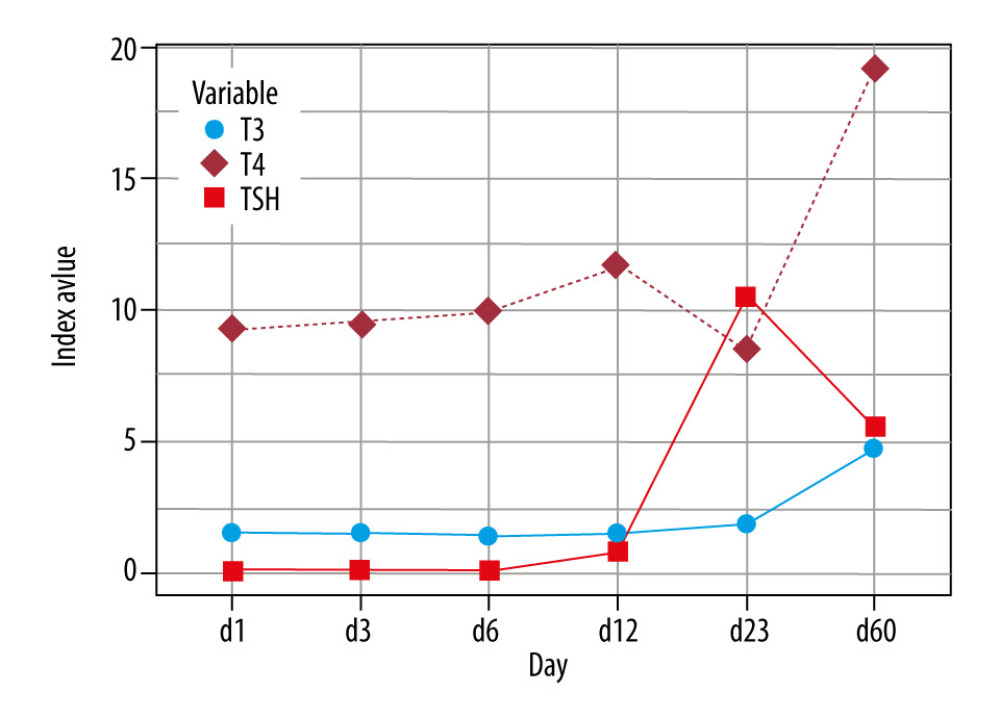 Figure 5. Trends of thyroid function.
Figure 5. Trends of thyroid function. 
References
1. Pang K, Shi ZD, Wei LY, Research progress of therapeutic effects and drug resistance of immunotherapy based on PD-1/PD-L1 blockade: Drug Resist Updat, 2023; 66; 100907
2. Chen Q, Wang C, Chen G, Delivery strategies for immune checkpoint blockade: Adv Healthc Mater, 2018; 7(20); e1800424
3. Duong SL, Barbiero FJ, Nowak RJ, Baehring JM, Neurotoxicities associated with immune checkpoint inhibitor therapy: J Neurooncolo, 2021; 152(2); 265-77
4. Postow MA, Callahan MK, Wolchok JD, Immune checkpoint blockade in cancer therapy: J Clin Oncol, 2015; 33(17); 1974-82
5. Ramos-Casals M, Brahmer JR, Callahan MK, Immune-related adverse events of checkpoint inhibitors: Nat Rev Dis Primers, 2020; 6(1); 38
6. Johnson DB, Manouchehri A, Haugh AM, Neurologic toxicity associated with immune checkpoint inhibitors: A pharmacovigilance study: J Immunother Cancer, 2019; 7(1); 134
7. Sidaway P, Addition of sintilimab to standard therapy improves event-free survival: Nat Rev Clini Oncol, 2024; 21(9); 640
8. Wang X, Sun X, Lei Y, The efficacy and safety of radiofrequency ablation combined with lenvatinib plus sintilimab in unresectable hepatocellular carcinoma: A real-world study: BMC Cancer, 2024; 24(1); 1036
9. Zeng Z, Yang A, Yang J, Sintilimab (anti-PD-1 antibody) combined with high-dose methotrexate, temozolomide, and rituximab (anti-CD20 antibody) in primary central nervous system lymphoma: A phase 2 study: Signal Transduction and Targeted Therapy, 2024; 9(1); 229
10. Zhang C, Sun YX, Yi DC, Neoadjuvant sintilimab plus chemotherapy in EGFR-mutant NSCLC: Phase 2 trial interim results (NEOTIDE/CTONG2104): Cell Rep Med, 2024; 5(7); 101615
11. Zhou B, Zhang F, Guo W, Five-year follow-up of neoadjuvant PD-1 inhibitor (sintilimab) in non-small cell lung cancer: J Immunother Cancer, 2024; 12(8); e009355
12. Barrios DM, Do MH, Phillips GS, Immune checkpoint inhibitors to treat cutaneous malignancies: J Am Acad Dermatol, 2020; 83(5); 1239-53
13. Hong Y, Ding ZY, PD-1 inhibitors in the advanced esophageal cancer: Front Pharmacol, 2019; 10; 1418
14. Tian Y, Abu-Sbeih H, Wang Y, Immune checkpoint inhibitors-induced hepatitis: Adv Exp Med Biol, 2018; 995; 159-64
15. Zhang Y, Yang Y, Chen Y, PD-L1: Biological mechanism, function, and immunotherapy in gastric cancer: Front Immunol, 2022; 13; 1060497
16. Cuzzubbo S, Javeri F, Tissier M, Neurological adverse events associated with immune checkpoint inhibitors: Review of the literature: Eur J Cancer, 2017; 73; 1-8
17. Wang DY, Salem JE, Cohen JV, Fatal toxic effects associated with immune checkpoint inhibitors: A systematic review and meta-analysis: JAMA Oncol, 2018; 4(12); 1721-28
18. Geng Y, Zhang Q, Feng S, Safety and efficacy of PD-1/PD-L1 inhibitors combined with radiotherapy in patients with non-small-cell lung cancer: A systematic review and meta-analysis: Cancer Med, 2021; 10(4); 1222-39
19. Marvin EA, Furrow KL, Kar A, Cuoco JA, Response of pembrolizumab alone for non-small cell lung cancer with brain metastasis: A case report and literature review: Front Oncol, 2020; 10; 577159
20. Mutlu L, Harold J, Tymon-Rosario J, Santin AD, Immune checkpoint inhibitors for recurrent endometrial cancer: Expert Rev Anticancer Ther, 2022; 22(3); 249-58
21. Wang Y, Chen R, Wa Y, Tumor immune microenvironment and immunotherapy in brain metastasis from non-small cell lung cancer: Front Immunol, 2022; 13; 829451
22. Barroso-Sousa R, Barry WT, Garrido-Castro AC, Incidence of endocrine dysfunction following the use of different immune checkpoint inhibitor regimens: A systematic review and meta-analysis: JAMA Oncol, 2018; 4(2); 173-82
23. Dalakas MC, Neurological complications of immune checkpoint inhibitors: What happens when you ‘take the brakes off’ the immune system: Ther Adv Neurol Disord, 2018; 11; 1756286418799864
24. Touat M, Talmasov D, Ricard D, Psimaras D, Neurological toxicities associated with immune-checkpoint inhibitors: Curr Opin Neurol, 2017; 30(6); 659-68
25. Williams TJ, Benavides DR, Patrice KA, Association of autoimmune encephalitis with combined immune checkpoint inhibitor treatment for metastatic cancer: JAMA Neurol, 2016; 73(8); 928-33
26. Zhang GM, Song N, Gao M, Pharmaceutical care for immune-related neurological adverse reactions caused by sintilimab: Medical Herald, 2020; 39(12); 1700-3
27. Gkoufa A, Gogas H, Diamantopoulos PT, Encephalitis in a patient with melanoma treated with immune checkpoint inhibitors: Case presentation and review of the literature: J Immunother, 2020; 43(7); 224-29
28. Papadopoulos KP, Romero RS, Gonzalez G, Anti-hu-associated autoimmune limbic encephalitis in a patient with PD-1 inhibitor-responsive myxoid chondrosarcoma: Oncologist, 2018; 23(1); 118-20
Figures
Figure 1. Timeline of the onset and treatment of immune-associated encephalitis caused by sintilimab.Figure 2. Results of cerebrospinal fluid smear under electron microscopy. Lymphocytes, monocytes, and occasional macrophages are seen under microscopy (cerebrospinal fluid).Figure 3. Trends of myocardial enzyme spectra.Figure 4. Trends of liver enzymes (P: post-treatment)Figure 5. Trends of thyroid function. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133