20 June 2025: Articles 
Secondary Pituitary Abscess Inside a Macroadenoma Complicated by Postoperative Hemorrhage and Reinfection: A Case Report
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Rare coexistence of disease or pathology
Anastasija KrzemińskaDOI: 10.12659/AJCR.947794
Am J Case Rep 2025; 26:e947794






Abstract
BACKGROUND: Pituitary abscess is a rare, potentially life-threatening condition that is challenging to diagnose on magnetic resonance imaging (MRI). Here, we present a case of pituitary abscess within an adenoma with a complicated postoperative course.
CASE REPORT: A 72-year-old man with progressive headache and left-eye visual field deficit underwent MRI, which revealed a parasellar region lesion compressing the optic chiasm, suggesting a pituitary macroadenoma. An endoscopic transnasal transsphenoidal approach was used for total tumor resection, during which purulent material was evacuated. Pathology confirmed a pituitary adenoma, and microbiology identified Proteus mirabilis and Cutibacterium acnes. Postoperatively, the patient’s vision did not improve due to a hemorrhage in the postoperative bed necessitating reoperation. Staphylococcus epidermidis was isolated from the second procedure. Following hematoma evacuation, his vision improved.
CONCLUSIONS: Pituitary abscess within an adenoma is rare and difficult to diagnose with MRI. Symptoms overlap with those of pituitary adenomas and abscesses, making clinical recognition challenging. Management requires prompt abscess drainage, lesion resection, and prolonged antibiotic therapy. This case demonstrates the importance of maintaining a broad differential diagnosis and not focusing on a single suspected pathology.
Keywords: Endocrine System Diseases, Magnetic Resonance Imaging, Pituitary Neoplasms, Humans, Male, Aged, Adenoma, brain abscess, Postoperative Hemorrhage, Pituitary Diseases, Staphylococcal Infections
Introduction
Pituitary abscess (PA) is a rare, potentially life-threatening condition characterized by an infection in the pituitary gland, leading to the formation of a pus-filled cavity. It accounts for less than 1% of all pituitary lesions and approximately 0.2–1.1% of patients undergoing pituitary surgery [1–6]. The true incidence is likely underreported, as PA is frequently misdiagnosed due to its non-specific clinical and radiologic features.
PA can be classified as either primary or secondary. Primary PA occurs in a normal pituitary gland without a pre-existing lesion or history of pituitary surgery. Secondary PA arises in the presence of a co-existing pituitary lesion, such as a pituitary adenoma, craniopharyngioma, or Rathke’s cleft cyst. Iatrogenic PA can also occur as a complication of pituitary surgery, even years after the procedure [7].
Diagnosing PA preoperatively remains a significant challenge. MRI, the primary imaging modality for sellar masses, often fails to distinguish PA from other non-infectious sellar lesions such as pituitary adenomas, Rathke’s cleft cysts, craniopharyngiomas, necrotic tumors, or hemorrhagic pituitary apoplexy.
Typical MRI features of PA are:
Unlike brain abscesses, PA does not always present with fever or elevated inflammatory markers, making clinical correlation difficult. As a result, many cases are misdiagnosed as non-infectious sellar masses and are only correctly identified during surgical drainage.
We present a case of a 72-year-old man with a secondary pituitary abscess within a pituitary adenoma, whose postoperative course was complicated by hemorrhage in the postoperative bed and reinfection. This case highlights the challenges of preoperative diagnosis of PA and underscores the lack of consensus regarding the optimal treatment of PA.
Case Report
HISTORY AND EXAMINATION:
A 72-year-old man presented with a few weeks of unspecified deterioration in vision and dimming of vision in the central visual field of the left eye. He denied any headaches, neck pain, nuchal rigidity, fevers, or night sweats. He had undergone numerous surgical operations over the preceding 7 years (since 2017), including large-intestine resection due to colorectal cancer, right-sided inguinal hernia repair, hernia repair after colostomy closure, and percutaneous coronary intervention. On admission, he was conscious and oriented to both self and surroundings. The neurological examination revealed a visual deficit, with defects in the initial bedside visual field test in the left eye, which was confirmed by ophthalmological examination (left-eye central scotoma).
Laboratory analysis revealed slightly low sodium levels, with normal inflammatory parameters. The level of insulin-like growth factor 1 was mildly decreased. Levels of prolactin, adrenocorticotropic hormone (ACTH), cortisol, luteinizing hormone (LH), follicle-stimulating hormone (FSH), growth hormone, thyroid-stimulating hormone (TSH), triiodothyronine (T3), and thyroxine (T4) were all within normal limits. Nasal swab screening for methicillin-resistant Staphylococcus aureus (MRSA) was performed before surgery, with negative results (no MRSA culture was identified).
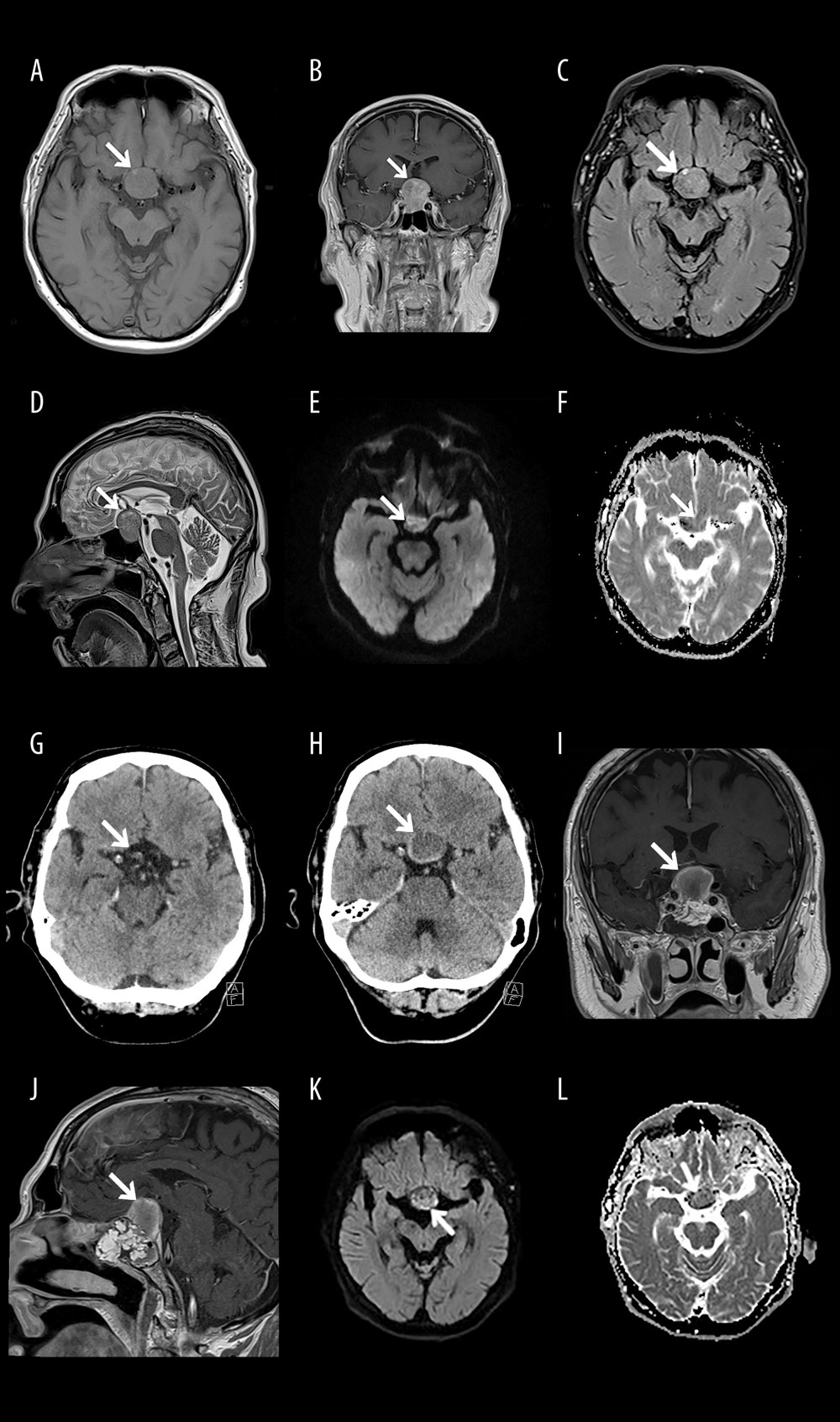
MRI examination, with and without gadolinium contrast, revealed a 30×25×23 mm solid contrast-enhancing sellar mass, extending into the suprasellar cistern and the sphenoid sinus. No characteristic, clearly defined peripheral enhancement of the lesion was observed after contrast administration. The mass compressed the optic chiasm and the bottom of the third ventricle, and displaced the pituitary infundibulum and gland (Figure 1A–1F). The lesion appeared isodense on T2-weighted dark fluid sequence, except for a hyperintense part measuring 4×4×10 mm in the upper portion of the lesion. The DWI sequence showed increased signal within the lesion, with features of diffusion restriction. Given these findings, the radiological image did not raise suspicion of a pituitary abscess. Instead, an MRI-based suspicion of a pituitary adenoma was suggested.
OPERATING PROCEDURE:
An endoscopic transsphenoidal transnasal approach was used to remove the lesion. Upon opening the sphenoid sinus, the bony septum was excised. After removing the mucosa, the floor of the sella was exposed. Once the bottom of the sella was opened and the dura was incised, part of the adenoma and purulent contents spontaneously evacuated. The adenoma was completely removed, resulting in decompression of the optic chiasm. The arachnoid remained intact, with no CSF leak. Hemostasis was achieved using Spongostan. A piece of adipose tissue was then taken from the left mid-abdomen. According to the protocol developed by F. Esposito et al, sellar floor plasty was performed using adipose tissue and tissue glue.
HISTOPATHOLOGIC ANALYSIS:
Microscopic analysis revealed pituitary adenoma/pituitary neuroendocrine tumor, PitNET. Immunohistochemical staining revealed a Ki-67 (MIB-1) of 1%.
MICROBIOLOGIC ANALYSIS:
POSTOPERATIVE COURSE:
The patient did not report improvement in the visual field and had a constant headache, which was not present before the surgery. A brain CT scan performed 10 hours after the surgery showed the postoperative bed without any residual adenoma (Figure 1G). Deviations in laboratory tests included low ACTH, testosterone, estradiol, T3, LH, and TSH levels; thus, the patient was diagnosed with anterior pituitary insufficiency. Due to the satisfactory postoperative brain CT results, the patient was discharged from the hospital. However, 9 days later, he was readmitted due to severe headache (which had not improved with pharmacological treatment) and worsening visual disturbances. Visual field defects also appeared in the right eye. Laboratory tests revealed low sodium levels (122 mmol/l), and CRP was elevated (61.9 mg/l), while other inflammatory markers were normal.
The follow-up brain CT examination revealed a mass of heterogeneous density in the sellar-suprasellar area, approximately 20×24×21 mm in size. An MRI confirmed the presence of a heterogeneous lesion showing peripheral enhancement on T1-weighted images. The DWI sequence showed increased signal within the lesion, indicating features of diffusion restriction. The lesion was pressing on the optic chiasm and the pituitary gland, along with the infundibulum (Figure 1H–1L).
REOPERATION:
The patient underwent urgent surgery, with a revision of the postoperative bed performed using a transsphenoidal endoscopic approach. A hematoma from the postoperative bed was evacuated. During the operation, material was collected for bacteriological testing, and Staphylococcus epidermidis was isolated. The strain was found to be sensitive to gentamicin, erythromycin, clindamycin, linezolid, and vancomycin. After the reoperation, he reported improvement in the visual field and no further headache.
Discussion
LIMITATIONS OF THE STUDY:
The case shows that MRI can be insufficient in diagnosing pituitary abscess (PA) within an adenoma, but we do not propose an alternative diagnostic method or biomarkers for better early detection. The patient underwent surgery in 2024, so there was no long-term follow-up to assess the final outcomes, including any long-term sequelae related to vision or other neurological issues. Without follow-up data, the long-term impact of the management strategy cannot be fully evaluated.
Conclusions
Pituitary abscess within an adenoma is a rare condition that is difficult to diagnose based solely on MRI examination, and presents a significant challenge in everyday clinical practice. The symptoms are non-specific and do not differ between a pituitary abscess with or without a pituitary adenoma, or a pituitary adenoma with or without an abscess. The most common imaging feature suggestive of PA is a lesion with high T2 and low T1 signal intensity, often with peripheral (rim) contrast enhancement, and possibly restricted diffusion on DWI. However, these findings are not definitive.
Given the diagnostic ambiguity, we recommend the following practical strategies to support clinical decision-making and improve early detection:
This case reinforces the importance of considering PA in the differential diagnosis of atypical sellar lesions, particularly when imaging and clinical features are incongruent. It also underscores the importance of not focusing on a single diagnosis, but rather remaining open to other possible diagnoses.
References
1. Vates GE, Berger MS, Wilson CB, Diagnosis and management of pituitary abscess: A review of twenty-four cases: J Neurosurg, 2001; 95(2); 233-41
2. Liu F, Li G, Yao Y, Diagnosis and management of pituitary abscess: Experiences from 33 cases: Clin Endocrinol (Oxf), 2011; 74(1); 79-88
3. Wang L, Yao Y, Feng F, Pituitary abscess following transsphenoidal surgery: The experience of 12 cases from a single institution: Clin Neurol Neurosurg, 2014; 124; 66-71
4. Agyei JO, Lipinski LJ, Leonardo J, Case report of a primary pituitary abscess and systematic literature review of pituitary abscess with a focus on patient outcomes: World Neurosurg, 2017; 101; 76-92
5. Gao L, Guo X, Tian R, Pituitary abscess: clinical manifestations, diagnosis and treatment of 66 cases from a large pituitary center over 23 years: Pituitary, 2017; 20(2); 189-94
6. Stringer F, Foong YC, Tan A, Pituitary abscess: A case report and systematic review of 488 cases: Orphanet J Rare Dis, 2023; 18(1); 165
7. Li Z, Yang C, Bao X, Clinical features and treatment of secondary pituitary abscess after transsphenoidal surgery: A retrospective study of 23 cases: World Neurosurgery, 2018; 113; e138-e45
8. Simmonds M, Ueber embolishe prozesse in der hypophysis: Virchow Arch Pathol Anat, 1914; 217; 226-39
9. Whalley N, Abscess formation in a pituitary adenoma: J Neurol Neurosurg Psychiatry, 1952; 15; 66-67
10. Tate MC, Jahangiri A, Blevins L, Infected Rathke cleft cysts: Distinguishing factors and factors predicting recurrence: Neurosurgery, 2010; 67(3); 762-69
11. Awad AJ, Rowland NC, Mian M, Etiology, prognosis, and management of secondary pituitary abscesses forming in underlying pituitary adenomas: J Neurooncol, 2014; 117; 469-76
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133