28 June 2025: Articles 
Coiling in Renovascular Hypertension: A Case Report of Fibromuscular Dysplasia and Complex Urinary Tract Abnormalities
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Rare coexistence of disease or pathology
Jakub PytlosDOI: 10.12659/AJCR.948913
Am J Case Rep 2025; 26:e948913






Abstract
BACKGROUND: Arterial hypertension (AH) affects 4% of children, with the most common etiologies including renal parenchymal disease, renovascular abnormalities, and primary hypertension. Severe hypertension in a patient with a urinary tract defect is a rare conjunction, requiring investigation for other coexisting pathologies.
CASE REPORT: We present the case of a 4-year-old boy with bedwetting, daytime urinary incontinence, and an episode of urinary tract infection, which led to an extensive diagnostic evaluation. The workup revealed bilateral vesicoureteral reflux, posterior urethral valves (PUV), suspected focal lesions in the left kidney, and stenosis of a branch of the right renal artery due to fibromuscular dysplasia. Initially, he required multidrug antihypertensive therapy, and coiling of the narrowed artery resulted in a significant improvement in blood pressure control. The urological conditions required pharmacotherapy for incontinence and an endoscopic transection of PUV. Currently, he remains on ramipril, desmopressin, and mirabegron, with good control of hypertension and urinary incontinence, normal renal function, and no recurrent urinary tract infections.
CONCLUSIONS: We present a unique case of a complex urinary tract defect with associated fibromuscular dysplasia treated with renal artery branch coiling. This combination of conditions is exceptionally uncommon, with only isolated reports in the literature describing such an approach. This case demonstrates the need for multidisciplinary management of children with hypertension and urinary symptoms. What initially appeared to be a straightforward urinary tract infection with bladder dysfunction evolved into a multifaceted clinical scenario requiring a combination of pharmacological management and staged interventional treatment.
Keywords: Fibromuscular Dysplasia, Hypertension, Renal Artery, Renal Circulation, Urethral Obstruction, Humans, Male, Hypertension, Renovascular, Child, Preschool, Renal Artery Obstruction, Embolization, Therapeutic, Urinary Incontinence
Introduction
Arterial hypertension, defined as blood pressure equal to or above the 95th percentile for age, sex, and height, affects approximately 4% of all children [1,2]. Secondary hypertension is elevated blood pressure resulting from a specific underlying cause, accounting for 45% to 85% of cases among children managed in pediatric nephrology or hypertension clinics [3]. Resistant hypertension is defined as elevated blood pressure that remains inadequately controlled despite the concurrent use of at least 3 antihypertensive drug classes, one of which must be a diuretic [2,4]. Among patients with resistant hypertension, the prevalence of secondary hypertension is significantly higher, underscoring the need for targeted diagnostic efforts to optimize management and outcomes [5].
Renal parenchymal disease is a significant etiology of secondary hypertension [6]. Vesicoureteral reflux, a common congenital urinary tract malformation, can result in renal parenchymal scarring and subsequent functional impairment, contributing to hypertension. Posterior urethral valves (PUV), exclusively affecting male patients, are a frequent cause of urinary tract obstruction and are commonly diagnosed prenatally. However, delayed diagnoses in childhood or adulthood are also documented [7].
Another important cause of secondary hypertension is fibromuscular dysplasia (FMD). FMD is an idiopathic, non-inflammatory disease of muscle tissue within the arterial walls, leading to narrowing of small and medium-sized arteries. In clinically symptomatic patients it predominantly affects the renal arteries, being the leading cause of renovascular hypertension (RVH) in North America and Europe. Additionally, it frequently involves cerebral vessels and, less commonly, the coronary, mesenteric, and extremity arteries. Diagnosis of FMD is difficult and requires a thorough differential diagnosis for other conditions such as inflammatory and monogenic arterial diseases [8–10].
Treatment of renovascular hypertension is particularly challenging because pharmacological treatment usually does not lead to complete recovery. Effective blood pressure control can be achieved or improved through percutaneous transluminal renal angioplasty (PTRA), stenting, or, in select cases, surgical angioplasty [11].
Congenital anomalies of the kidney and urinary tract (CAKUT) are innate developmental abnormalities affecting the kidneys, ureters, bladder, and/or urethra. These abnormalities range from kidney malformations or agenesis to blockages and other structural defects within the urinary tract. Interconnected pathologies regarding renal arteries and CAKUT are exceptionally rare.
In this case report, we outline the diagnostic process and therapeutic approach in a patient with interconnected pathologies, emphasizing the challenges and strategies involved in achieving effective blood pressure control and preventing adverse outcomes. We emphasize the importance of a multidisciplinary approach and targeted management in cases of secondary hypertension.
Case Report
A 4-year-old boy presented to the Nephrology Department with primary nocturnal enuresis, daily urinary incontinence, and suspected arterial hypertension. Five months before, he experienced a
The boy was born as a second child at 39 weeks of gestation via cesarean section to a mother with gestational diabetes. He weighed 3920 grams and had an Apgar score of 10. The perinatal period was uncomplicated. However, his developmental milestones were delayed, and he achieved independent sitting and walking at 13 months. He was also diagnosed with attention deficit hyperactivity disorder (ADHD) and a history of recurrent otitis media, resulting in conductive hearing impairment.
The boy was admitted in good general condition; his physical examination revealed no abnormalities, he had not been circumcised and had no phimosis. His height was 110 cm (94th percentile), weight was 20.7 kg (97th percentile), and his blood pressure was up to 150/116 mmHg (above the 95th percentile) [12,13]. The laboratory tests showed normal kidney function, hyperkalemia, metabolic alkalosis, and markedly elevated plasma renin activity and aldosterone levels (Table 1) [14]. An abdominal ultrasound revealed no kidney or urinary tract abnormalities. Voiding cystourethrography (VCUG) provided a more detailed assessment, revealing bilateral vesicoureteral reflux: grade I active reflux on the right side and grade III/IV active and passive reflux on the left side (Figure 1). Uroflowmetry showed low bladder capacity, an irregular micturition curve, and no post-void residual urine. Dynamic renal scintigraphy suggested possible post-inflammatory changes in the left kidney parenchyma, along with changes resembling a calyx neck stricture or prolonged parenchymal transit in the dorsal region of the right kidney. The effective renal plasma flow (%ERPF) was 44.5% in the left kidney and 55.5% in the right kidney. A Doppler ultrasound of the renal arteries was performed, revealing no abnormalities. However, a subsequent CT angiography of the abdomen demonstrated possible stenosis of the lower branch of the right renal artery and hypodense areas in the left kidney (Figure 2). Given the need to differentiate between a renovascular and hyperplastic etiology, an oncologic evaluation and magnetic resonance imaging (MRI) were performed, ruling out a neoplastic process (Figure 3). As for hypertension-mediated organ damage, the ophthalmology evaluation suggested a slight narrowing of the vessels in the posterior pole, echocardiography showed no abnormalities (left ventricular mass index 39.14 g/m2.7), and urinary albumin excretion was 6.21 mg/g. Following a titration of antihypertensive medications, the patient was discharged on ramipril 3.75 mg (0.1 mg/kg/24 h) and metoprolol 2×6.25 mg (0.63 mg/kg/24 h).
A month later, office blood pressure measurements and 24-hour ambulatory blood pressure monitoring (ABPM) revealed persistent severe arterial hypertension. To address this, the antihypertensive regimen was adjusted by increasing the dose of metoprolol 25+12.5 mg (2 mg/kg/24 h) and adding hydrochlorothiazide 25+12.5 mg (2 mg/kg/24 h) and amlodipine 1×5 mg (0.25 mg/kg/24 h). These changes significantly reduced blood pressure (110-120/70-80 mmHg). However, follow-up laboratory tests revealed elevated serum urea (37 md/dl), uric acid (7.8 mg/dl), and calcium (10.4 mg/dl) levels, prompting a subsequent decrease in the hydrochlorothiazide dosage of 1×12.5 mg (0.63 mg/kg/24 h).
A multidisciplinary team of nephrologists, oncologists, and radiologists, after reviewing the patient’s complex clinical presentation of resistant arterial hypertension and urinary tract anomalies, determined that arteriography was indicated. This procedure confirmed significant focal narrowing (90–95%) of the proximal aspect of a segmental artery supplying the lower pole of the right kidney, a stenosis more severe than initially observed on CT imaging. After 2 unsuccessful attempts at percutaneous transluminal renal angioplasty using 4×10 mm balloons with poor morphological results, the decision was made to occlude the vessel through coiling. The procedure was successfully carried out using 5 coils, leading to exclusion of a region in the lower part of the kidney (Figure 4). The procedure allowed for a significant reduction in antihypertensive medication dosages to amlodipine 1×5 mg (0.25 mg/kg/24 h) and ramipril 1×3.75 mg (0.1 mg/kg/24 h).
We consulted the Institute of Rheumatology about our patient’s results, which definitively ruled out a diagnosis of a systemic disease or systemic vasculitis as the cause of renal artery stenosis. Based on the characteristic CT findings and the exclusion of an inflammatory etiology and syndromic presentation for the narrowing, a diagnosis of fibromuscular dysplasia was proposed.
A comprehensive assessment was conducted to evaluate the presence of FMD-related lesions beyond the renal arteries. MRI of the head revealed no focal lesions or other abnormalities. CT angiography of the head confirmed no vessel narrowing, aneurysms, or other arterial malformations.
The boy experienced persistent nocturnal enuresis and daily urinary incontinence (multiple times a day). Despite initial treatment with mirabegron and tamsulosin for bladder dysfunction with prophylactic furazidine, his symptoms did not improve. Due to subsequent recurrent urinary tract infections, he was qualified for cystoscopy with a possible endoscopic reflux treatment. During the procedure, previously unrecognized posterior urethral valves were identified and resected (at age 6 years). After the procedure, there was a notable reduction in the severity of diurnal enuresis (once a week) and nocturnal enuresis (once or twice a week). Cystometry demonstrated normal bladder capacity, a normal flow rate, a normal pressure-flow curve, and minimal post-void residual urine. With the addition of desmopressin therapy, both diurnal and nocturnal enuresis were significantly improved.
After 4 years of continuous antihypertensive therapy, a follow-up CT angiography was performed which revealed no significant renal artery stenosis, although the possibility of minor stenosis adjacent to the previously placed coil could not be excluded (Figure 5). Repeat PTRA was recommended if blood pressure control deteriorated. To address polypharmacy, the patient’s mirabegron dose was reduced, and discontinuation of desmopressin was attempted but unsuccessful. These medications, despite their positive effects on bladder function, can have hypertensive effects.
The patient is now 10 years old, remains under outpatient nephrology clinic care, has normal height (150 cm; 91th percentile) and weight (47.7 kg; 91th percentile), kidney function, and sodium and potassium levels (Table 1), and is currently prescribed ramipril 5 mg (0.1 mg/kg/24 h), desmopressin 120 μg, and tamsulosin 0.4 mg [14,15]. During follow-up visits, blood pressure measurements have remained consistently within the normal range. Ambulatory blood pressure monitoring showed mean systolic and diastolic blood pressure below the 95th percentile during waking (126/77 mmHg) and sleep periods (113/62 mmHg) [16]. Episodes of enuresis are now infrequent and sporadic. The patient, along with his parents, reported a good overall sense of well-being, with no significant concerns during follow-up. They also emphasized that the patient tolerated the treatment regimen well, without experiencing any notable adverse effects.
Discussion
This case report presents a successful diagnosis and management in a patient with interconnected urinary tract and renal vessel pathologies. In cases of resistant hypertension, a renovascular etiology should always be considered and assessed through imaging. Notably, arterial hypertension is uncommon among patients with congenital anomalies of the kidney and urinary tract (CAKUT). Doppler ultrasound is an excellent initial screening tool; however, it is insufficient to definitively exclude the presence of a stenosis, particularly in small segmental vessels [2,17]. Therefore, CT angiography or magnetic resonance angiography is generally recommended in cases of uncertain involvement of renal arteries, allowing for a more comprehensive evaluation [9].
Fibromuscular dysplasia is a rare systemic vasculopathy requiring detailed evaluation for extra-renal involvement in all patients. This assessment should specifically include, but is not limited to, the craniocervical, aortic, mesenteric, and coronary arteries [18].
As demonstrated in the case of our patient, pharmacological treatment alone often fails to achieve adequate and sustained blood pressure control, despite the concurrent use of multiple drug classes. In clinical practice, it serves as a temporary measure for patients undergoing evaluation for RVH, for those in whom therapeutic interventions are not feasible, and as a supplementary treatment following such interventions [8,19].
Percutaneous transluminal renal angioplasty (PTRA) is regarded as an effective treatment for renovascular hypertension [17,20]. Despite its invasive nature, the procedure remains the preferred choice for patients with FMD due to its benefits, including the restoration and preservation of renal perfusion and a reduction in polypharmacy. Stenting is considered an alternative treatment option; however, it has notable limitations, including the risk of restenosis due to growth-related evolution of arteries and uncertain long-term outcomes. Stents may be appropriate in selected cases, such as severe or recurrent stenosis, iatrogenic dissections, or vessels exhibiting significant elastic recoil or restenosis following angioplasty. For patients who are not suitable candidates for minimally invasive interventions, open surgical revascularization remains a definitive therapeutic option [11]. Unlike stenting or procedures involving artificial grafts, PTRA preserves the artery’s ability to grow with the patient. However, the risk of restenosis remains substantial, with reported rates of 50.8% after the first PTRA and 41.7% after the second [21].
In our patient, because PTRA failed to produce a significant morphological improvement in 2 separate attempts, we decided to proceed with complete occlusion of the narrowed segmental artery. The use of embolization coils in improving blood pressure control in renovascular hypertension is considered controversial. Many authors do not recommend this approach due to the variability of outcomes, as ischemic regions can trigger renin secretion, sustaining collateral circulation and potentially maintaining hypertension [21–25]. However, the procedure has successfully been used in managing hypertension in children [26,27]. Likewise, in our patient, coil embolization led to a significant reduction in antihypertensive medication requirements.
Posterior urethral valves are the most frequent cause of urinary tract obstruction and one of the most common entities leading to chronic and end-stage kidney disease within the pediatric population [28]. In male patients presenting with urinary disorders, diurnal or nocturnal enuresis, or urinary tract infections, PUV should always be considered. The voiding cystourethrogram is considered the criterion standard for PUV diagnosis, as Tambo et al diagnosed 88.9% of all PUV using this technique [29]. Due to its variable severity and morphology, PUV diagnosis can be challenging and it can occur during later childhood, adolescence, or even adulthood [30]. Vesicoureteral reflux is a potential complication of PUV and was observed in this patient. Notably, the morphology of the urethra in VCUG and the results of uroflowmetry were not suggestive of PUV, emphasizing the need for an individual approach in every case of a boy with recurrent UTI and urinary disturbances.
Arterial hypertension is not a typical feature of patients with CAKUT. On the contrary, many of these children experience urinary salt and water loss, predisposing them to hypotension and episodes of dehydration. However, a recent analysis of 331 pediatric patients with CAKUT identified arterial hypertension in 62 cases (19%), with posterior urethral valves (PUV) emerging as a significant risk factor for its development [31]. Arterial hypertension poses a substantial threat to kidney function in patients with CAKUT, and adequate antihypertensive treatment is crucial in slowing the progression of chronic kidney disease (CKD). As renin-angiotensin-aldosterone system overactivation remains the crucial driver of blood pressure elevation in these patients, angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers type I, which also promote an anti-fibrotic effect, are drugs of choice in these cases [32].
The presence of complex urogenital and renovascular anomalies requires a multidisciplinary approach to patient care. Data regarding a potential association between renovascular hypertension and obstructive uropathy are limited [33]. Pharmacological management may be insufficient in these cases, and surgical or endovascular interventions may be required to achieve significant clinical improvement.
Conclusions
We present a unique case of a complex urinary tract defect with associated fibromuscular dysplasia treated with renal artery branch coiling. This combination of conditions is exceptionally rare, with only isolated reports in the literature describing such an approach to renal artery stenosis treatment in children. Timely detection and management of CAKUT and renal artery stenosis can reduce the risk of complications. This case demonstrates the need for a multidisciplinary approach to children with hypertension and urinary symptoms. What initially appeared to be a straightforward urinary tract infection with bladder dysfunction evolved into a multifaceted clinical scenario requiring a combination of pharmacological management and staged interventional treatment.
Figures
 Figure 1. Voiding cystourethrogram. Bilateral vesicoureteral reflux: grade I active reflux on the right side (→) and grade III/IV active and passive reflux on the left side. Dilated left renal pelvis (*).
Figure 1. Voiding cystourethrogram. Bilateral vesicoureteral reflux: grade I active reflux on the right side (→) and grade III/IV active and passive reflux on the left side. Dilated left renal pelvis (*). 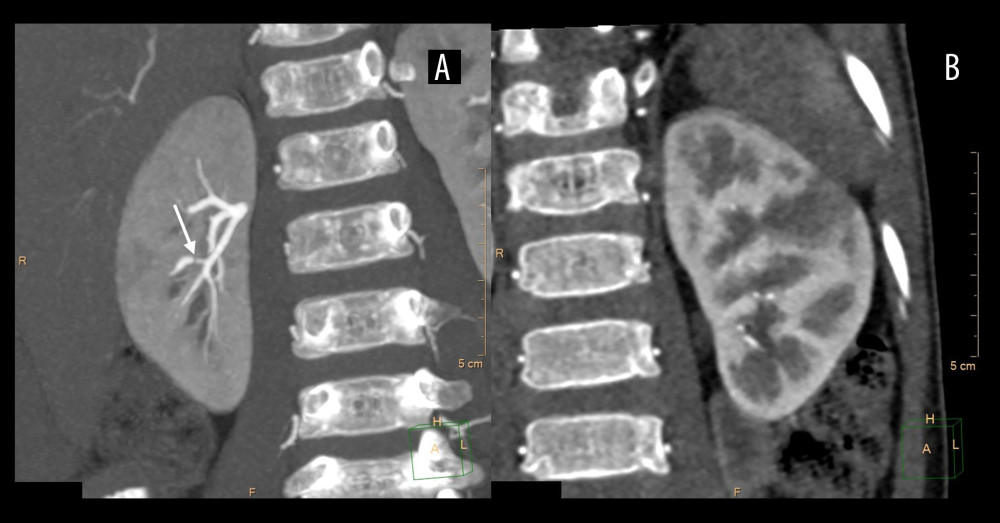 Figure 2. CT angiography of the abdomen. A stenosis of the lower branch of the right renal artery (A, →) and hypodense areas in the left kidney (B).
Figure 2. CT angiography of the abdomen. A stenosis of the lower branch of the right renal artery (A, →) and hypodense areas in the left kidney (B). 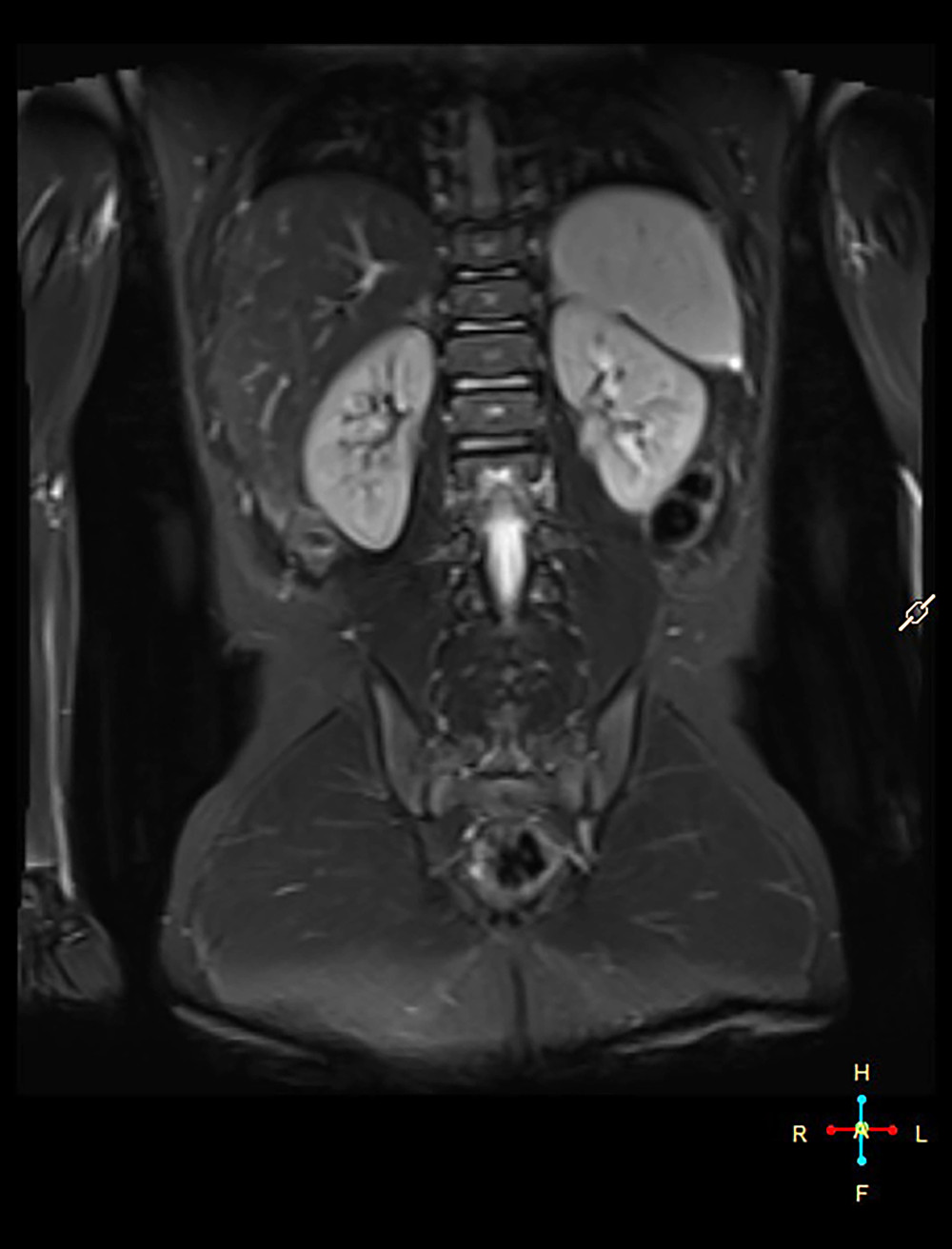 Figure 3. MRI of the abdomen. No abnormalities within the left kidney.
Figure 3. MRI of the abdomen. No abnormalities within the left kidney. 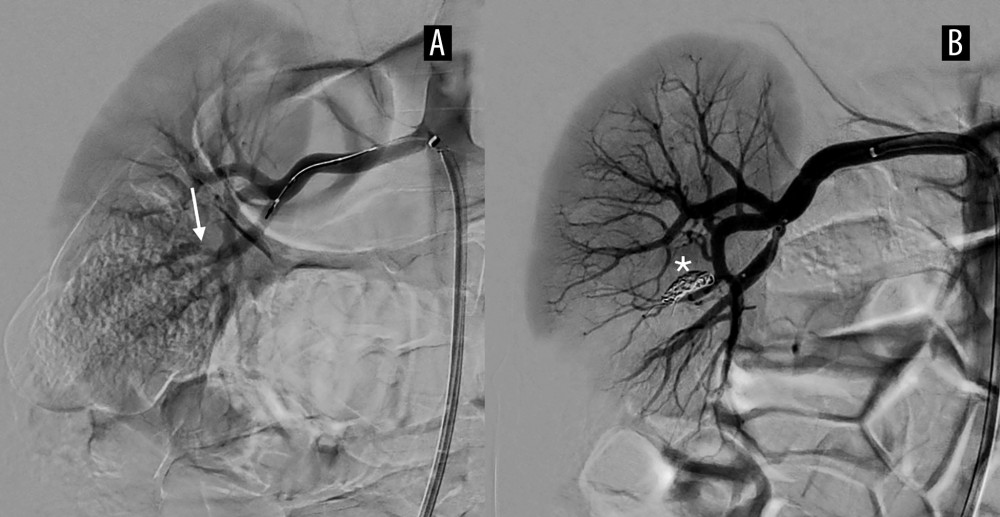 Figure 4. Arteriography. Significant focal narrowing of the proximal aspect of a segmental artery (→), branch arising from the lower division of the right renal artery (A). Coils occluding the narrowed vessel (B, *).
Figure 4. Arteriography. Significant focal narrowing of the proximal aspect of a segmental artery (→), branch arising from the lower division of the right renal artery (A). Coils occluding the narrowed vessel (B, *).  Figure 5. Follow-up CT angiography 4 years after coiling.
Figure 5. Follow-up CT angiography 4 years after coiling. 
References
1. Song P, Zhang Y, Yu J, Global prevalence of hypertension in children: JAMA Pediatr, 2019; 173; 1154
2. Carey RM, Calhoun DA, Bakris GL, Resistant hypertension: Detection, evaluation, and management: A scientific statement from the American Heart Association: Hypertension, 2018; 72(5); e53-e90
3. Nugent JT, Young C, Funaro MC, Prevalence of secondary hypertension in otherwise healthy youths with a new diagnosis of hypertension: A meta-analysis: J Pediatr, 2022; 244; 30-37e10
4. Williams B, Mancia G, Spiering W, 2018 ESC/ESH Guidelines for the management of arterial hypertension: Eur Heart J, 2018; 39; 3021-104
5. Sudano I, Suter P, Beuschlein F, Secondary hypertension as a cause of treatment resistance: Blood Press, 2023; 32(1); 2224898
6. Uwaezuoke SN, Odimegwu CL, Mbanefo NR, Posterior urethral valve in children: Using novel biomarkers as an early predictive tool for the onset and progression of chronic kidney disease: Front Urol, 2022; 2; 904452
7. Zornoza M, Angulo JM, Parente A, Late diagnosis of posterior urethral valves: Actas Urol Esp, 2015; 39; 646-50
8. Villegas L, Cahill AM, Meyers K, Pediatric renovascular hypertension: Manifestations and management: Indian Pediatr, 2020; 57; 443-51
9. Gornik HL, Persu A, Adlam D, First International Consensus on the diagnosis and management of fibromuscular dysplasia: Vasc Med, 2019; 24; 164-89
10. Plouin P-F, Baguet J-P, Thony F, High prevalence of multiple arterial bed lesions in patients with fibromuscular dysplasia: Hypertension, 2017; 70; 652-58
11. Pytlos J, Michalczewska A, Majcher P, Renal artery stenosis and mid-aortic syndrome in children – a review: J Clin Med, 2024; 13; 6778
12. Kułaga Z, Grajda A, Gurzkowska B, Polish 2012 growth references for preschool children: Eur J Pediatr, 2013; 172; 753-61
13. Grajda A, Kułaga Z, Gurzkowska B, Preschool children blood pressure percentiles by age and height: J Hum Hypertens, 2017; 31; 400-8
14. Schwartz GJ, Muñoz A, Schneider MF, New equations to estimate GFR in children with CKD: J Am Soc Nephrol, 2009; 20; 629-37
15. Kułaga Z, Litwin M, Tkaczyk M, Polish 2010 growth references for school-aged children and adolescents: Eur J Pediatr, 2011; 170; 599-609
16. Wühl E, Witte K, Soergel M, Distribution of 24-h ambulatory blood pressure in children: Normalized reference values and role of body dimensions: J Hypertens, 2002; 20; 1995-2007
17. Patel PA, Cahill AM, Renovascular hypertension in children: CVIR Endovasc, 2021; 4; 10
18. Savard S, Steichen O, Azarine A, Association between 2 angiographic subtypes of renal artery fibromuscular dysplasia and clinical characteristics: Circulation, 2012; 126; 3062-69
19. Louis R, Levy-Erez D, Cahill AM, Imaging studies in pediatric fibromuscular dysplasia (FMD): A single-center experience: Pediatr Nephrol, 2018; 33; 1593-99
20. Gottsater A, Lindblad B, Optimal management of renal artery fibromuscular dysplasia: Ther Clin Risk Manag, 2014; 10; 583-95
21. Kądziela J, Jóźwik-Plebanek K, Pappaccogli M, Risks and benefits of renal artery stenting in fibromuscular dysplasia: Lessons from the ARCADIA-POL study: Vasc Med, 2024; 29; 50-57
22. Tullus K, Brennan E, Hamilton G, Renovascular hypertension in children: Lancet, 2008; 371; 1453-63
23. McLaren CA, Roebuck DJ, Interventional radiology for renovascular hypertension in children: Tech Vasc Interv Radiol, 2003; 6; 150-57
24. Hobbs DJ, Barletta G-M, Mowry JA, Renovascular hypertension and intrarenal artery aneurysms in a preschool child: Pediatr Radiol, 2009; 39; 988-90
25. Ognjanovic M V, Selective renal embolisation for renovascular hypertension?: Arch Dis Child, 2002; 86; 127-29
26. Warren WC, Warshaw BL, Hymes LC, Selective embolization of a stenotic intrarenal artery for control of hypertension: J Pediatr, 1982; 101; 743-45
27. Docx MK, Vandenberghe P, Maleux G, Severe hypertension due to renal polar artery stenosis in an adolescent treated with coil embolization: Pediatr Radiol, 2009; 39; 1234-37
28. Nishio H, Mizuno K, Kato T, A case of posterior urethral valve identified in an older child by straining to void: Urol Case Rep, 2022; 40; 101886
29. Tambo FFM, Tolefac PN, Ngowe MN, Posterior urethral valves: 10 years audit of epidemiologic, diagnostic and therapeutic aspects in Yaoundé gynaeco-obstetric and paediatric hospital: BMC Urol, 2018; 18; 46
30. Bomalaski MD, Anema JG, Coplen DE, Delayed presentation of posterior urethral valves: A not so benign condition: J Urol, 1999; 162; 2130-32
31. Taha K, Catapang M, Becknell B, Hypertension in children with congenital anomalies of the kidney and urinary tract: Pediatr Nephrol, 2024; 39; 1185-92
32. Gabriele MM, Koch Nogueira PC, Management of hypertension in CAKUT: Protective factor for CKD: Front Pediatr, 2019; 7; 222
33. Muchant DG, Gloor JM, Norling LL, Persistent severe hypertension in an infant with posterior urethral valves: Pediatric Nephrology, 1996; 10; 764-65
Figures
Figure 1. Voiding cystourethrogram. Bilateral vesicoureteral reflux: grade I active reflux on the right side (→) and grade III/IV active and passive reflux on the left side. Dilated left renal pelvis (*).Figure 2. CT angiography of the abdomen. A stenosis of the lower branch of the right renal artery (A, →) and hypodense areas in the left kidney (B).Figure 3. MRI of the abdomen. No abnormalities within the left kidney.Figure 4. Arteriography. Significant focal narrowing of the proximal aspect of a segmental artery (→), branch arising from the lower division of the right renal artery (A). Coils occluding the narrowed vessel (B, *).Figure 5. Follow-up CT angiography 4 years after coiling. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133