10 July 2025: Articles 
Spontaneous Evisceration of a Parastomal Hernia with Small-Bowel Strangulation: A Case Report
Unusual clinical course
Doru-Florian-Cornel Moga ABCDEF 1,2*, Angela Georgiana Diaconu BEF 3, Valentin Oprea BCDEF 4,5DOI: 10.12659/AJCR.949330
Am J Case Rep 2025; 26:e949330






Abstract
BACKGROUND: Evisceration of intra-abdominal organs is a rare, serious event. It normally occurs in 2 particular situations: postoperative or post-traumatic. Spontaneous evisceration of abdominal contents is an uncommon condition.
CASE REPORT: An 83-year-old male patient, with a significant history of multiple comorbidities, prior abdomino-perineal resection for rectal adenocarcinoma, and ongoing chemotherapy for metastatic disease, presented to the Emergency Department with spontaneous evisceration of multiple small-bowel loops. The evisceration occurred through the site of a recurrent parastomal hernia, located on the left lateral aspect of the abdominal wall, adjacent to the colostomy site. The evisceration occurred due to rupture of the overlying skin in the area of the hernia sac, adjacent to the colostomy. At the time of the hospital presentation, approximately 6 hours after evisceration, the intestinal loops appeared congested. An emergency surgery was undertaken, involving segmental resection of the ileum with primary anastomosis and no mesh repair of the parastomal hernia, due to contamination. The postoperative outcome was slowly favorable and the patient was discharged on the 8th postoperative day.
CONCLUSIONS: This case report presents a rare but potentially serious clinical situation of spontaneous evisceration occurring in the context of a parastomal hernia in a patient with neoplasia.
Keywords: Hernia, Abdominal, Prolapse, Humans, Male, Aged, 80 and over, Intestinal Obstruction, Colostomy, Intestine, Small, incisional hernia, Hernia, Ventral, Surgical Stomas
Introduction
Evisceration of intra-abdominal contents is a rare and potentially life-threatening condition, most commonly caused by burst abdomen, stab wound, or abdominal gunshot injuries.
Spontaneous evisceration through an abdominal wall hernia is uncommon, typically occurring in the context of an acute (eg coughing or vomiting exertion) or chronic (eg, ascites, visceromegaly, pregnancy) increase in intra-abdominal pressure [1,2]. This presentation is exceedingly rare and small-bowel evisceration is even rarer [3].
Common stoma complications include poor stoma siting, high output, skin irritation, ischemia, retraction, parastomal hernia, and prolapse [4,5]. In patients with parastomal hernia, similar to other types of abdominal hernias, complications such as incarceration, bowel obstruction, and strangulation can occur [6]. However, parastomal evisceration is an exceptionally rare complication, with only a few cases documented in the literature to date [6,7].
Case Report
An 83-year-old man was referred to our center from his local hospital (Figure 1), with spontaneous rupture of a parastomal hernia on14 February 2025. At the time of admission, more than 6 hours after the onset of evisceration, the patient was conscious, oriented, and hemodynamically stable. Physical examination of the abdomen revealed strangulated small-bowel loops protruding through the parastomal defect.
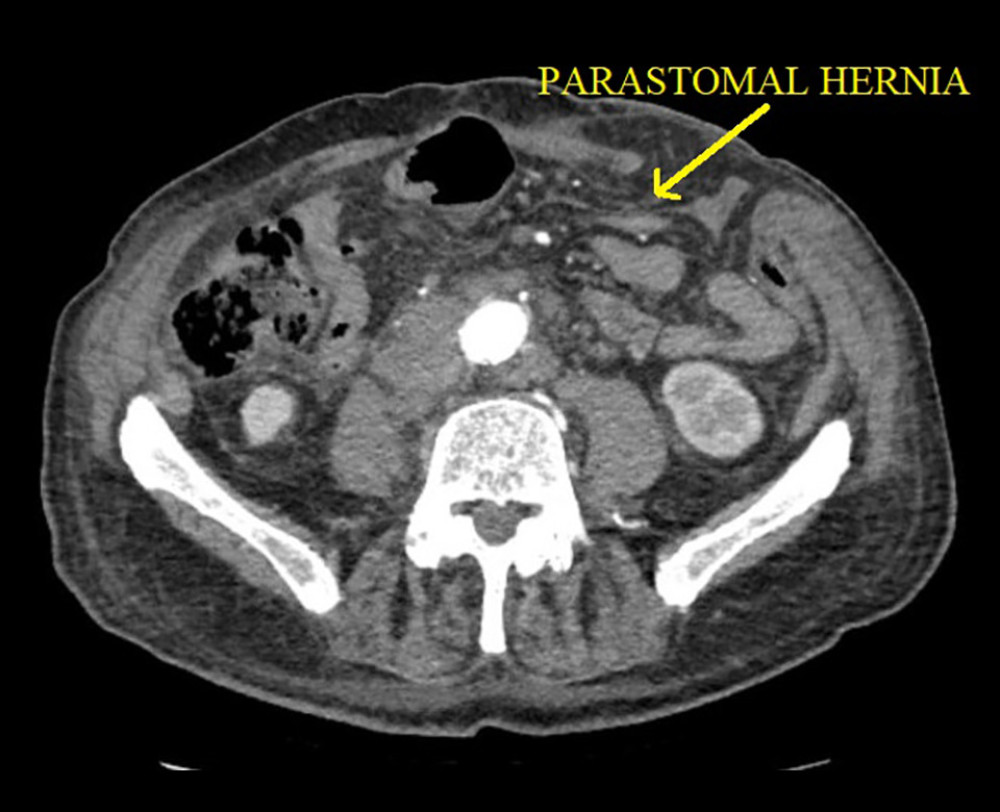
The patient’s significant surgical history included a Miles’ operation for rectal adenocarcinoma with multiple hepatic metastases performed 3 years ago, followed by tissue-based surgical repair of a parastomal hernia 2 years ago. At the time of presentation, he was undergoing adjuvant chemotherapy (Xelox and Bevacizumab). Review of his medical records revealed a known recurrence of the parastomal hernia (Figure 2).
The patient did not report any recent episodes of coughing, vomiting, abdominal trauma, or symptoms suggestive of bowel obstruction, such as the absence of flatus or stool from the stomal site. Laboratory investigations showed mild anemia (hemoglobin: 9.2 g/dL) and coagulopathy, with an INR of 1.54 (reference range 0.80–1.2) and thrombocytopenia (platelet count 48 000/mm3).
Emergency surgical intervention was carried out, without any additional imaging investigation. Intraoperative findings included a prolapsed stoma and approximately 1 meter of small intestine eviscerated through a 5-centimeter skin defect located at the superior border of the colostomy site (Figure 3). Manual reduction of the eviscerated bowel was not feasible due to bowel distention, induration, and signs of venous congestion and early hemorrhagic changes. In these conditions, a midline laparotomy was performed. Consequently, segmental ileal resection was undertaken (Figure 4), followed by a latero-lateral ileo-ileal anastomosis. Concomitantly, the stoma prolapse was corrected and no mesh repair of the parastomal hernia was performed, due the risk of using the mesh in contaminated fields.
The patient received transfusions of 4 units of fresh frozen plasma and 1 unit of packed red blood cells. Postoperative recovery was slowly favorable and the patient was discharged on the 8th postoperative day (the histological appearance suggested small-bowel infarction).
Discussion
Incisional hernias are a common sequela of abdominal surgeries, with a reported incidence of up to 20% in patients undergoing laparotomy [8]. Among individuals with stomas, the risk is even higher, with parastomal hernias being one of the most common long-term complications.
Spontaneous bowel evisceration from primary or incisional hernia is rare and has been reported from umbilical [1,3], incisional [8–11], parastomal [4–7,12,13], and inguinal hernias [14], with ascites, pregnancy [15], and obesity as predisposing factors.
Parastomal evisceration is a very uncommon late complication of a stoma, with only a few cases currently published in the literature (Table 1).
The spontaneous rupture of an incisional or parastomal hernia can occur either suddenly, often in response to a rapid increase in intra-abdominal pressure (eg, coughing, heavy lifting), or gradually, as a result of chronic pressure and tissue thinning. Gradual rupture has been associated with ulceration at the dependent portion of the hernia sac. Larger hernias are generally more prone to rupture due to the thin hernia sac, with atrophied, avascular overlying skin [8,10]. There are authors who consider that the combination of a prolapsed colostomy and an underlying parastomal hernia can predispose to necrosis of the colostomy wall, ultimately leading to evisceration [4,13]. However, in our assessment, there is insufficient evidence to confirm that the coexistence of these 2 conditions directly increases the risk of evisceration. Rather, their simultaneous presence may reflect a neglected or long-standing hernia process, indicating progressive deterioration of the abdominal wall integrity.
Spontaneous bowel evisceration requires immediate surgical intervention. Delayed management can result in bowel incarceration, ischemia, gangrene, and even perforation [10,11]. In most cases, the defect acts as a constrictive ring, which causes a vicious cycle of arterial impedance in the herniated contents. Hence, the contents progress from induced hypoxia from incarceration to gangrenous rupture [11]. For parastomal hernia repair, the procedures used can be with or without mesh, at the surgeon’s discretion, depending on the degree of contamination.
The approach to management depends on the viability of the eviscerated bowel. In cases without necrosis, reduction through an enlarged hernia orifice may be sufficient. However, if the bowel is found to be nonviable, segmental resection followed by anastomosis is warranted [8,12].
Conclusions
Spontaneous evisceration of a parastomal hernia with associated small-bowel strangulation is an exceptionally rare but serious late complication of stoma formation. Given its potentially life-threatening nature, prompt surgical intervention is imperative to prevent irreversible bowel injury and optimize clinical outcomes and minimize morbidity. Regular follow-up for high-risk stoma patients is mandatory.




References
1. Good DW, Royds JE, Smith MJ, Umbilical hernia rupture with evisceration of omentum from massive ascites: A case report: J Med Case Rep, 2011; 5; 170
2. West C, Richards J, Sujendran V, Wheeler J, Spontaneous evisceration of the appendix through an incisional hernia at rest: BMJ Case Rep, 2016; 2016; bcr2016217585
3. Grappolini N, Zanchetta M, Inversini D, Ietto G, Spontaneous bowel evisceration through umbilical hernia in an adult non-cirrhotic patient: BMJ Case Rep, 2024; 17(4); e258602
4. Lolis ED, Savvidou P, Vardas K, Parastomal evisceration as an extremely rare complication of a common procedure: Ann R Coll Surg Engl, 2015; 97; e103-e104
5. Yucel AF, Pergel A, Aydin I, Sahin DA, A rare stoma-related complication: parastomal evisceration: Ind J Surg, 2014; 76; 154-55
6. Basnayake O, Jayarajah U, Jayasinghe J, Spontaneous rupture of a parastomal hernia with evisceration of small bowel: A case report: BMC Surg, 2019; 19(1); 43
7. Izwan S, Perera OM, Guy S, Late parastomal evisceration: A case report of a rare complication following loop ileostomy for an obstructing rectal cancer: Int J Surg Case Rep, 2023; 105; 107936
8. Shiva Ahmad F, Manpreet Hemanth K, Breaking bad: Spontaneous rupture of incisional hernia: Cureus, 2024; 16(3); e56009
9. Friedman MH, Spontaneous evisceration through a ventral hernia: Can Med Assoc J, 1965; 92(13); 670-71
10. Thalahitiyage N, Ravindrakumar S, Nandasena J, Spontaneous evisceration of incisional hernia with strangulation of small bowel: A life threatening complication: Case Rep Surg, 2021; 2021; 6684360
11. Das S, Shaikh O, Gaur NK, Balasubramanian G, Spontaneous evisceration of small bowel in incisional hernia: Cureus, 2022; 14(2); e22374
12. Kulkarni AA, Chauhan V, Sharma V, Singh H, Parastomal evisceration: A report of two cases and review of literature: Cureus, 2019; 11(9); e5750
13. Lapeña-Rodríguez M, Fernández-Moreno MC, Late parastomal evisceration: Int J Colorectal Dis, 2020; 35(9); 1787-89
14. Zaz MA, Dass T, Muhee A, Kawoosa U, An unusual case of inguinal hernia with spontaneous evisceration: Hernia, 2011; 15(6); 705-7
15. Ahmed A, Stephen G, Ukwenya Y, Spontaneous rupture of umbilical hernia in pregnancy: A case report: Oman Med J, 2011; 26(4); 285-87
16. Villa M, Iannelli E, Grande M, An unusual case of small intestine evisceration through a transverse loop colostomy: Colorectal Dis, 2012; 14; e27-e28
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133