06 July 2025: Articles 
Bowel Ischemia as a Rare Manifestation of Extracranial Moyamoya Disease: A Case Report
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Rare disease
Sameera Shuaibi ABCDEFG 1*, Najat AlSejari ABCDEFG 1, Ian Tobal ABCDEFG 1, Reinaldo Quevedo AEF 1DOI: 10.12659/AJCR.949530
Am J Case Rep 2025; 26:e949530






Abstract
BACKGROUND: Moyamoya disease (MMD) is a rare, progressive cerebrovascular disorder characterized by bilateral stenosis or occlusion of the internal carotid arteries and the development of fragile collateral vessels within the circle of Willis. The disease primarily affects the intracranial vasculature, with extracranial manifestations being exceedingly uncommon. Gastrointestinal (GI) involvement, in particular, is rarely described in the literature.
CASE REPORT: We present the case of a 20-year-old White man with a known diagnosis of MMD who developed severe gastrointestinal complications. He presented with persistent coffee-ground emesis, fatigue, and dizziness. Initial investigations revealed microcytic anemia, and upper-GI endoscopy showed advanced esophagitis and duodenal ulceration. Further imaging demonstrated mesenteric artery stenosis, suggestive of vascular involvement outside the cerebral circulation. Despite medical management, the patient required multiple blood transfusions due to ongoing bleeding and symptomatic anemia. This case is notable for its atypical presentation of MMD with systemic vascular involvement extending beyond the central nervous system. The presence of mesenteric artery stenosis and upper-GI tract ulceration raises the concern for extracranial arteriopathy potentially linked to the pathophysiologic processes of MMD.
CONCLUSIONS: Clinicians should maintain a high index of suspicion for extracranial involvement in patients with MMD who present with unexplained systemic symptoms, particularly gastrointestinal bleeding. Early recognition and multidisciplinary intervention are essential to mitigate complications and improve outcome.
Keywords: Esophagitis, Ischemia, Mesenteric Arteries, Humans, moyamoya disease, Male, young adult
Introduction
Moyamoya disease (MMD) is a rare, chronic, and progressive occlusive disorder primarily affecting the intracranial vessels. It was first reported with a high incidence among Asian populations, specifically in Japan [1]. Due to its initial geographical predilection, genetic etiologies were isolated [2]. However, more recently, the prevalence has been increasing in Western countries, sparking further investigation into the development of this disease. MMD is uncommon, with an incidence of 0.086 per 100 000 people, and affects females nearly twice as often as males [3,4]. MMD typically presents with symptoms secondary to disease involving the intracranial vessels such as headaches, seizures, stroke/TIA, and other neurological symptoms. It seldom affects extracranial vessels. Treatment is mainly surgical and focuses on tissue reperfusion, leaving little room for medical intervention. Gastrointestinal involvement of this disease is often overlooked. We present an unusual case of MMD with rare extracranial involvement affecting the vessels of the gastrointestinal system, leading to widespread gastrointestinal sequelae.
Case Report
A 20-year-old man with a history of moyamoya disease, multiple strokes, gastritis, and hypertension was evaluated for altered mental status. He initially presented to an outside facility with intractable nausea and vomiting of 6 weeks duration. Approximately 1 month prior to the start of his gastrointestinal (GI) symptoms, he was evaluated by Gastroenterology due to chronic nausea and vomiting and underwent an upper endoscopy, which yielded normal findings. However, the day he presented to the Emergency Department, his vomitus was frothy and coffee-ground in color. This was coupled with black, tarry stools. His medical history was otherwise notable for taking prophylactic aspirin due to his prior strokes.
Upon evaluation in the Emergency Department, his blood pressure was 264/168 mmHg. In addition, he was found to have an acute kidney injury with a creatinine of an 8.3 mg/dL, hyperkalemia of 5.5 mmol/L, hemoglobin of 6.9 g/dL (baseline 15 g/dL), platelet count of 79 000 K/uL, and a BNP of 5000 (Table 1). He received 1 unit of packed red blood cells, with minimal improvement in his Hgb. An initial CT head was negative, but repeat MRI showed multiple new and extensive areas of ischemic injury, predominantly affecting the frontal and left temporoparietal lobes and cerebellar regions. He was also in respiratory distress, requiring bilevel positive airway pressure (BIPAP) ventilation. Given his critical status, he was transferred to a higher level of care in the Intensive Care Unit (ICU).
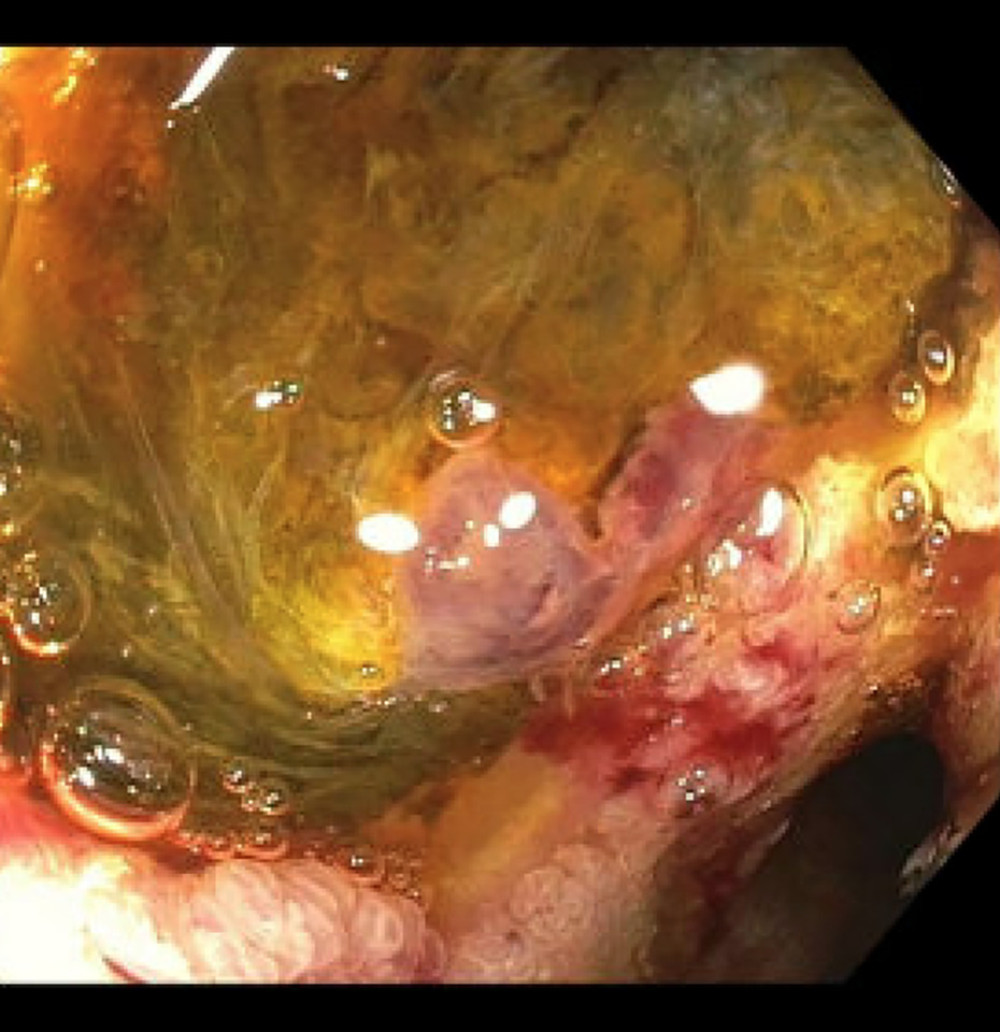
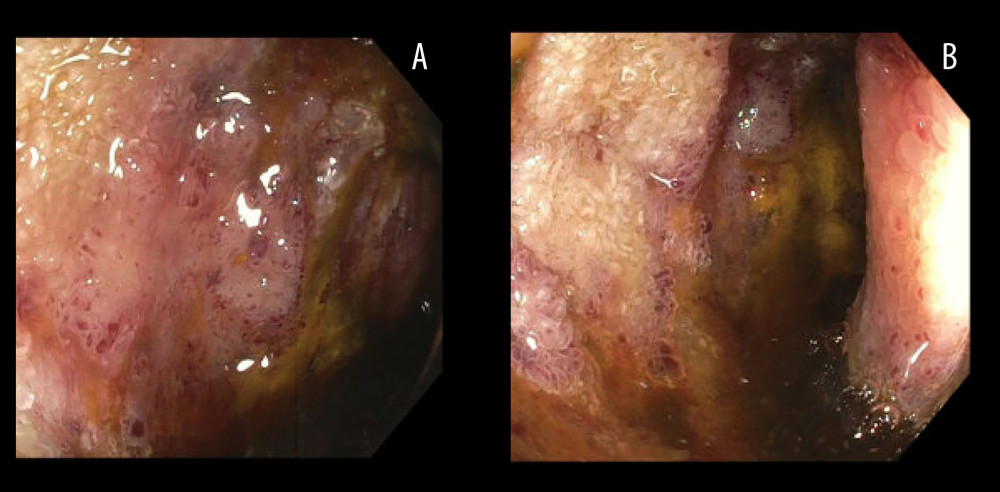
The Gastroenterology team initially deferred endoscopy until he was stabilized. However, his hemoglobin level continued to trend downward, despite transfusion. Ultrasound of mesenteric arteries revealed high-grade stenosis without evidence of mesenteric ischemia. He subsequently underwent an upper endoscopy, which showed LA grade D esophagitis without bleeding (Figure 1), 2 oozing, cratered ulcers in the duodenal bulb (Figure 2), another non-bleeding duodenal ulcer in the first portion of the duodenum, and diffuse mucosal changes characterized by congestion, discoloration, and erythema in the jejunum (Figure 3A, 3B). Biopsies obtained were consistent with nonspecific ulceration and did not yield any neoplasia.
Discussion
Moyamoya disease is divided into 2 entities: disease and syndrome. The former is an isolated type that occurs in the absence of an underlying disease process, as opposed to the latter, which occurs in the presence of a secondary disorder such as sickle cell anemia, Down’s syndrome, neurofibromatosis, and long-standing inflammatory conditions such as lupus, among many others [5,6]. Genetic causes have also been implicated, with mutations in chromosome 17 being the most common [14]. Moyamoya is characterized by the steno-occlusion of intracranial vessels, especially the internal carotid artery, in a bilateral or unilateral fashion. This leads to development of collateral vessels to bypass the occlusion in efforts to restore some cerebral blood flow. It subsequently manifests with ischemic strokes, which are the most common manifestations of the disease. This is what gives it the characteristic ‘hazy puff of smoke’ appearance on angiography, which translates to ‘moya moya’ in Japanese [7,8]. With time, these collaterals can be subjected to higher blood flow, which can lead to their rupture, and intracranial hemorrhage, which is considered a less common manifestation of the disease as opposed to its ischemic/stenotic counterpart [9–11]. Since most MMD manifestations and sequelae occur within the cerebrum, our case demonstrates an unusual presentation of the disorder that affected the gastrointestinal tract.
Typically, magnetic resonance angiography is confirmational, but if MRA is not readily available, CT angiography can suffice as a substitute [12–15]. Often, the treatment is surgical; bypass surgery to revascularize affected areas and enhance perfusion can be utilized. This inherently leaves very little room for medical management.
Extracranial vessel involvement is rare compared to the predilection of this disease process to the intracranial vessels. Only a few studies have commented on the proportion of extracranial involvement, not limited to gastrointestinal involvement alone, which was under 17% altogether. The pathophysiology of vascular involvement in the gastrointestinal tract is the same as that of the intracranial one, and the repercussions can be as immense. Physicians may not opt to pinpoint MMD as the culprit behind gastrointestinal manifestations, which highlights the importance of broadening the differential diagnosis, especially in young individuals, particularly those with underlying genetic diseases.
Conclusions
In conclusion, while moyamoya disease is traditionally associated with intracranial vascular changes, its potential to affect the gastrointestinal tract should not be overlooked. Extracranial manifestations, although rare, can significantly impact patient health and complicate diagnosis. Recognizing and addressing gastrointestinal involvement early is essential for improving patient outcomes and preventing further complications. This case highlights the importance of a comprehensive approach in moyamoya disease, considering the full spectrum of possible manifestations, including those in the gastrointestinal system.


References
1. Khan NT, Islam S, Bari A, A case report of moyamoya disease presenting as recurrent right-sided weakness: Cureus, 2023; 15(5); e39209
2. Ott WP, Bellamy S, Onyali CB, A rare case of moyamoya disease in a Hispanic woman: Unveiling non-asian ethnicity and atypical risk factors: Am J Case Rep, 2023; 24; e940353
3. Uchino K, Johnston SC, Becker KJ, Tirschwell DL, Moyamoya disease in Washington State and California: Neurology, 2005; 65(6); 956-58
4. Baba T, Houkin K, Kuroda S, Novel epidemiological features of moyamoya disease: J Neurol Neurosurg Psychiatry, 2008; 79(8); 900-4
5. Ashley WW, Zipfel GJ, Moran CJ, Moyamoya phenomenon secondary to intracranial atherosclerotic disease: diagnosis by 3T magnetic resonance imaging: J Neuroimaging, 2009; 19(4); 381-84
6. Ferris EJ, Levine HL, Cerebral arteritis: Classification: Radiology, 1973; 109(2); 327-41
7. Burke GM, Burke AM, Sherma AK, Moyamoya disease: A summary: Neurosurg Focus, 2009; 26(4); E11
8. Rupareliya C, Lui F, Moyamoya disease: StatPearls [Internet] Jun 25, 2023, Treasure Island (FL), StatPearls Publishing
9. Funaki T, Takahashi J, Takagi Y, Unstable moyamoya disease: Clinical features and impact on perioperative ischemic complications: J Neurosurg, 2015; 122(2); 400-7
10. Lee SU, Oh CW, Kwon O-Ki, Surgical treatment of adult moyamoya disease: Curr Treat Options Neurol, 2018; 20(7); 22
11. Demartini Z, Teixeira BC, Koppe GL, Moyamoya disease and syndrome: A review: Radiol Bras, 2022; 55(1); 31-37
12. Mertens R, Graupera M, Gerhardt H, The genetic basis of moyamoya disease: Transl Stroke Res, 2022; 13(1); 25-45
13. Yamada I, Matsushima Y, Suzuki SY, Moyamoya disease: Diagnosis with three-dimensional time-of-flight MR angiography: Radiology, 1992; 184(3); 773-78
14. Tarasów E, Kułakowska A, Lukasiewicz A, Moyamoya disease: Diagnostic imaging: Pol J Radiol, 2011; 76(1); 73-79
15. Scott RM, Smith ER, Moyamoya disease and moyamoya syndrome: N Engl J Med Mar, 2009; 360(12); 1226-37
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133