30 December 2025: Articles 
Beyond CKD-Associated Pruritus: Paraneoplastic Itch Revealing CLL/SLL in ESRD: A Case Report
Unknown etiology, Challenging differential diagnosis, Diagnostic / therapeutic accidents, Clinical situation which can not be reproduced for ethical reasons, Rare coexistence of disease or pathology
Julia KacperczykDOI: 10.12659/AJCR.949787
Am J Case Rep 2025; 26:e949787






Abstract
BACKGROUND: Pruritus is common in chronic dialysis patients, usually due to metabolic imbalance, xerosis, or other cutaneous complications of chronic kidney disease (CKD), leading to a diagnosis of CKD-associated pruritus (CKD-aP). When symptoms persist despite optimized dialysis, stable laboratory indices, and no dermatologic cause, alternative etiologies must be considered.
CASE REPORT: A 66-year-old man with end-stage renal disease (ESRD) of unknown origin, treated with peritoneal dialysis, developed progressive, treatment-resistant pruritus. Initially localized to the extremities without primary lesions, it was unresponsive to standard therapies. As the itch became generalized, systemic symptoms emerged, including fatigue, lower-extremity edema, and pancytopenia. Differential diagnoses were excluded. Pre-transplant abdominal CT revealed generalized lymphadenopathy and splenomegaly. A bone marrow biopsy confirmed chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) by immunophenotyping. Due to ESRD and active malignancy, the patient was ineligible for chemotherapy or kidney transplantation; pruritus management remained conservative.
CONCLUSIONS: Persistent pruritus in dialysis patients warrants reevaluation beyond CKD-aP, especially in those with unknown CKD etiology and hematologic abnormalities. Recognizing paraneoplastic itch as a potential early sign of malignancy can enable earlier diagnosis in high-risk populations.
Keywords: Hematologic Neoplasms, Kidney Failure, Chronic, Leukemia, B-Cell, Lymph Nodes, Pandemics, Pruritus, Humans, Male, Aged, Paraneoplastic Syndromes, Leukemia, Lymphocytic, Chronic, B-Cell
Introduction
Pruritus serves as a physiological defense mechanism against harmful and dangerous environmental factors [1–4]. Itching-related signals are transmitted by neurons and can originate in either the central or peripheral nervous system, ultimately reaching the free nerve endings in the skin, triggering an intense urge to rub or scratch the affected area to achieve relief [5,6]. The itch–scratch cycle, besides its well-documented contribution to cutaneous damage, is a distressing symptom negatively affecting quality of life (QoL) [4,7–10]. While transient pruritus is a common sensory experience in the general population, chronic or pathological itching is frequently associated with dermatologic conditions, such as atopic dermatitis and eczema, as well as systemic disorders involving metabolic, immunological, or endocrine dysregulation [10,11].
Chronic kidney disease-associated pruritus (CKD-aP) is a clinical diagnosis with 58–90% prevalence in patients undergoing chronic renal replacement therapy (RRT) [2,12,13]. Moderate-to-severe pruritus is expected to affect 40–55% of hemodialysis (HD) patients and 56% of those treated by peritoneal dialysis (PD) [12–14]. In patients undergoing dialysis, pruritus may arise either from uremia, hyperphosphatemia, and inflammation, or from the chronic dryness of the skin characteristic of chronic kidney disease (CKD) [7,15].
Although CKD-aP is the most common cause of chronic itch in dialysis patients, persistent, treatment-resistant pruritus – particularly when hematologic abnormalities are present – should raise the suspicion of potential systemic or paraneoplastic etiologies.
Our patient’s chronic pruritus had no clear renal etiology. Initially, it was managed as an idiopathic pruritus by a dermatologist for over a year. Chronic lymphocytic leukemia manifesting primarily as refractory pruritus in peritoneal dialysis patients is exceedingly rare, and only sporadic case reports have suggested an association; there remains no established guidance for evaluating pruritus as a paraneoplastic phenomenon in this population. During routine hematological evaluations related to dialysis management, lymphopenia was incidentally identified, prompting further investigation and ultimately leading to a hematological consultation, thus hastening the diagnostic process.
Paraneoplastic pruritus can precede a malignancy diagnosis by weeks to months, as lymphoma-associated itching has been reported in up to 30% of patients and can be an early warning sign. Reviews also document that malignancy-related pruritus often lacks primary skin lesions, aligning with our patient’s presentation.
By discussing this unusual presentation, we propose that pruritus refractory to standard treatments in dialysis patients – especially when combined with pancytopenia – should be integrated into future diagnostic algorithms and clinical guidelines, ensuring earlier hematologic evaluation and timely intervention.
Case Report
A 66-year-old man with stage 5 CKD of idiopathic origin, supported exclusively on PD as his primary RRT for the past 6 months, presented with gradual worsening of symptoms.
He had a history of obesity (BMI: 31 kg/m2) and asymptomatic gallstones, diagnosed incidentally via abdominal ultrasonography with no scheduled cholecystectomy. He also had secondary hyperparathyroidism with parathyroid hormone (PTH) level of 25.5 pmol/L (normal range 1.6–6.9 pmol/L), consistent with prolonged renal dysfunction. A comprehensive diagnostic workup conducted prior to and following PD catheter insertion (performed in June 2020) revealed mild anemia, mild neutrophilia and eosinophilia, hypoproteinemia, and hypogammaglobulinemia. Abdominal ultrasonography showed no significant abnormalities, and the dialysis dose appeared to be sufficient.
Six months after peritoneal dialysis initiation, he developed persistent pruritus, primarily affecting the extremities. The most pronounced excoriations – linear, erythematous lesions predominantly affecting the calves – are shown in Figure 1.
Laboratory tests at that time revealed that urea and phosphate levels were within the expected range for a dialysis patient, thus ruling out chronic kidney disease-associated pruritus (CKD-aP). A dermatological evaluation led to a diagnosis of idiopathic pruritus, initially managed with dermocosmetics and antihistamines, but these provided only temporary relief. At no point was a primary dermatologic rash identified, supporting the notion that the itch was systemic in nature. Initially, it remained localized to the calves and arms, but eventually spread to involve the trunk and back, becoming generalized. As symptoms persisted, vascular assessments were performed, only to rule out venous insufficiency. Differential diagnoses considered at this stage included cholestasis, peripheral neuropathy, and metabolic pruritus, all of which were ruled out based on liver function tests, neurological examination, and adequate dialysis parameters, respectively. Over time, the pruritus worsened, coinciding with the onset of fatigue and lower-limb edema, complicating the clinical picture. Figure 2 illustrates the chronological appearance of the symptoms.
November 2021: The patient contracted moderate COVID-19, treated outside our center with systemic steroids (methylprednisolone, 16 mg twice daily). His pruritus temporarily subsided during this period but reoccurred shortly after steroid discontinuation.
April 2022: Given the symptom worsening, initial dermatology treatment was intensified with oral methylprednisolone (16 mg twice daily) and rupatadine (10 mg daily), offering partial symptom control. However, the underlying cause remained unclear, necessitating further diagnostic evaluation.
June 2021–July 2022: At that time, leukopenia was noted and initially attributed to viral infection following the patient’s COVID-19 illness. However, the prolonged period of leukopenia raised concern for an underlying hematologic disorder.
July 2022 – Kidney Transplant Evaluation: As part of the patient’s pre-transplant assessment, abdominal ultrasonography was performed, revealing splenomegaly and free fluid in the peritoneal cavity. These findings, combined with concurrent leukopenia, thrombocytopenia, and palpable subclavicular lymphadenopathy, prompted further hematological assessment. A follow-up CT confirmed generalized lymphadenopathy and hepatosplenomegaly, leading to temporary disqualification from transplant candidacy pending further diagnostic workup.
October 2023: The patient was admitted with progressive gastrointestinal symptoms, including anorexia, nausea, dyspepsia, and early satiety. X-ray imaging showed mediastinal widening and abdominal lymphadenopathy. CT scans (Figure 3) confirmed the findings.
April 2024: A bone marrow biopsy was performed, revealing >90% infiltration by CD20+, CD23+, CD79+ B cells with weak/focal CD5 expression and no CD34+ blasts. TP53 mutation was not detected, and the IGHV gene was mutated and productive – both markers are associated with a more favorable prognosis. No features of Richter transformation or p53 overexpression were present. Staging at diagnosis was consistent with advanced disease (Rai stage III-IV, Binet stage C), based on generalized lymphadenopathy, hepatosplenomegaly, leukopenia, and thrombocytopenia.
Given the patient’s advanced renal dysfunction and dialysis dependence, the hematology care team determined that initiating standard chemotherapy posed a significant risk of toxicity due to altered drug clearance. Furthermore, active malignancy disqualified the patient from the previously considered renal transplantation. Thus, the decision was made to adopt a supportive management approach with symptomatic treatment, accompanied by close nephrological and hematological monitoring, rather than the targeted therapy.
The patient’s condition evolved over several months, culminating in the identification of hepatosplenomegaly, widespread lymphadenopathy, and a definitive diagnosis of CLL/SLL, as shown in Table 1. To provide further clinical context, Figure 4 illustrates the longitudinal changes in leukocyte count. This case highlights a diagnostically complex and clinically rare presentation of CLL manifesting primarily as pruritus in a dialysis patient – a phenomenon that remains rarely described in the literature. This case underscores the importance of hematologic vigilance in evaluating persistent pruritus and suggests the need for an interdisciplinary approach when symptoms remain unexplained despite appropriate renal management.
Discussion
This case report illustrates a rare and diagnostically challenging presentation of CLL in a patient with ESRD undergoing peritoneal dialysis (PD), initially misattributed to mineral disturbances typical for CKD. While pruritus is a commonly experienced symptom in dialysis patients – reported in up to two-thirds of patients and often attributed to CKD-aP – its persistence despite standard therapy, particularly when accompanied by hematologic abnormalities, should prompt a broader diagnostic evaluation [2,8,10,14,16–18].
In our patient, moderate-to-severe pruritus persisted despite optimized dialysis parameters, topical treatments, and empirical therapy with antihistamines and oral corticosteroids. This clinical course was atypical for CKD-aP, which generally responds to conventional symptom management [3,4,9,15,19]. The concurrent presence of leukopenia and thrombocytopenia further supported the suspicion of an underlying systemic process. In the absence of uremic complications or dialysis inadequacy, these findings warranted investigation for a hematologic malignancy [3,10,17,18].
Although CLL has been described as a potential cause of renal dysfunction or glomerular injury [20–23], it is infrequently reported as the initial cause of pruritus in dialysis patients. A small number of case reports have documented hematologic malignancies presenting with treatment-refractory pruritus. Lelonek et al found that over 50% of patients with another hematological malignancy, polycythemia vera, experienced aquagenic pruritus prior to hematologic diagnosis, reinforcing the notion of pruritus as a possible paraneoplastic signal [24]. Despite increasing awareness of paraneoplastic itch in hematology and dermatology, its presence is rarely prioritized in the differential diagnosis of pruritus among dialysis patients. This may reflect diagnostic anchoring to CKD-aP, particularly in patients with known renal disease.
Our case is further distinguished by the unknown etiology of CKD, the absence of dialysis inadequacy or rash, and the fact that pruritus remained the sole clinical symptom for over a year. To the best of our knowledge, this is the first reported case of biopsy-confirmed CLL/SLL in a dialysis patient presenting with isolated pruritus over an extended period, without constitutional symptoms, lymphadenopathy, or organomegaly at onset.
Pruritus in hematologic malignancies is believed to arise from immune dysregulation, cytokine imbalance – particularly involving interleukins such as IL-6 and IL-31 – and altered neural signaling pathways [7,9,10,18,25,26]. Yosipovitch et al (2010) observed that pruritus preceded lymphoma diagnosis in a significant subset of patients, in some cases by several months [18]. These findings collectively emphasize the potential for itch to be an early, yet underrecognized, paraneoplastic manifestation in systemic disease [25–28].
In our case, the clinical trajectory of persistent pruritus without dermatologic pathology, the gradual appearance of cytopenias, and eventual radiologic evidence of lymphoproliferative disease, highlights the need to reassess persistent idiopathic pruritus in dialysis patients, particularly when hematologic abnormalities co-occur [27,28].
The nonspecific symptomatology and overlap with CKD-aP contributed to the delayed diagnosis of malignancy. Delays were further compounded by COVID-19–related disruptions in nephrology and hematology care, which further impacted specialist referrals and access to imaging [29,30].
In this patient, laboratory abnormalities raised concern, but the diagnosis of CLL was ultimately confirmed only after the pre-transplant imaging revealed hepatosplenomegaly and generalized lymphadenopathy, followed by bone marrow biopsy and immunophenotyping (CD5+, CD19+, and CD23+ clonal B cells). The absence of monoclonal gammopathy or paraproteinemia further supported a lymphoid etiology.
The coexistence of CLL/SLL and ESDR imposed significant therapeutic limitations. Chemotherapy posed a substantial risk of toxicity due to impaired renal clearance [31–33], and active malignancy rendered the patient ineligible for kidney transplantation. Therefore, the therapeutic approach focused on symptom control and multidisciplinary monitoring.
Although novel agents such as difelikefalin or gabapentinoids may provide relief in CKD-aP [4,10,17,19,34–36], their safety in patients with concurrent hematologic malignancies remains uncertain. Our experience underscores the need for further research on supportive care strategies tailored to patients with overlapping renal dysfunction and hematologic malignancy.
The association between CKD and lymphoproliferative disorders warrants further study. ESRD patients exhibit higher rates of monoclonal B-cell lymphocytosis (MBL), likely due to chronic immune activation and impaired B-cell regulation [37–41]. In this case, the absence of a clear cause for CKD raises the possibility that undiagnosed early-stage CLL or MBL may have contributed to the renal decline, although this remains speculative in the absence of renal histopathology [22,37–41].
Notably, no kidney biopsy was performed earlier to assess for leukemic infiltration or immune-mediated glomerular injury in this patient, limiting our ability to establish a definitive causal link between CLL and renal failure in our patient. Nonetheless, CLL/SLL has been reported to affect the kidneys via direct infiltration or paraneoplastic mechanisms [20–22,31,39,42].
Dialysis-related immune dysfunction may have also influenced disease progression, given the altered lymphocyte profiles observed in this population [40,42,43]. Due to the diagnosis of CLL/SLL, close hematologic surveillance was initiated. While observation remains the standard of care for asymptomatic early-stage CLL, patients with ESRD require more frequent assessment for cytopenias, lymphadenopathy, or signs of Richter’s transformation [21,32,33,38,40,44].
From a clinical perspective, our case report recognizes the importance of comprehensive malignancy screening in patients with chronic pruritus of unknown pathology, particularly when systemic symptoms or hematological abnormalities arise. A multidisciplinary diagnostic strategy involving nephrology, dermatology, and hematology could be implemented in chronic dialysis patients with idiopathic generalized pruritus. Future research or guidelines explicitly recognizing paraneoplastic pruritus as a red flag may benefit this unique and high-risk population.
Conclusions
This case report underscores the importance of reassessing presumed CKD-aP in dialysis patients when pruritus is refractory to standard interventions. Hematologic evaluation should be considered in patients with unexplained cytopenias, persistent systemic symptoms, or atypical pruritus patterns. The findings in this case emphasize the potential interplay between CKD and hematologic disorders, raising questions about the role of dialysis-related immune dysfunction in lymphoproliferative disease evolution.
Figures
 Figure 1. Severe linear excoriations on the patient’s calves, attributed to chronic pruritus. The photograph was taken during the most recent admission in May 2024, at a time when pruritus had slightly decreased. The distribution and morphology of the lesions suggest a secondary etiology, consistent with CKD-aP. The absence of primary dermatologic pathology supports a systemic origin.
Figure 1. Severe linear excoriations on the patient’s calves, attributed to chronic pruritus. The photograph was taken during the most recent admission in May 2024, at a time when pruritus had slightly decreased. The distribution and morphology of the lesions suggest a secondary etiology, consistent with CKD-aP. The absence of primary dermatologic pathology supports a systemic origin. 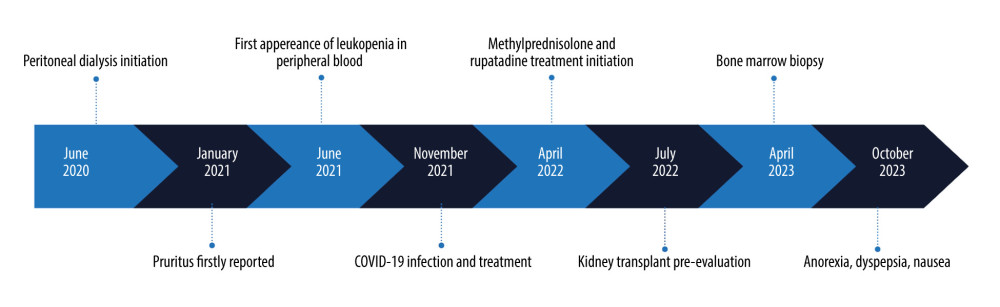 Figure 2. Diagnostic process and findings revealed during PD control admissions. This illustrates the chronological appearance of the symptoms found in our patient, presented in the order and timing of each manifestation as they were first reported, with the starting date being the peritoneal dialysis catheter insertion.
Figure 2. Diagnostic process and findings revealed during PD control admissions. This illustrates the chronological appearance of the symptoms found in our patient, presented in the order and timing of each manifestation as they were first reported, with the starting date being the peritoneal dialysis catheter insertion. 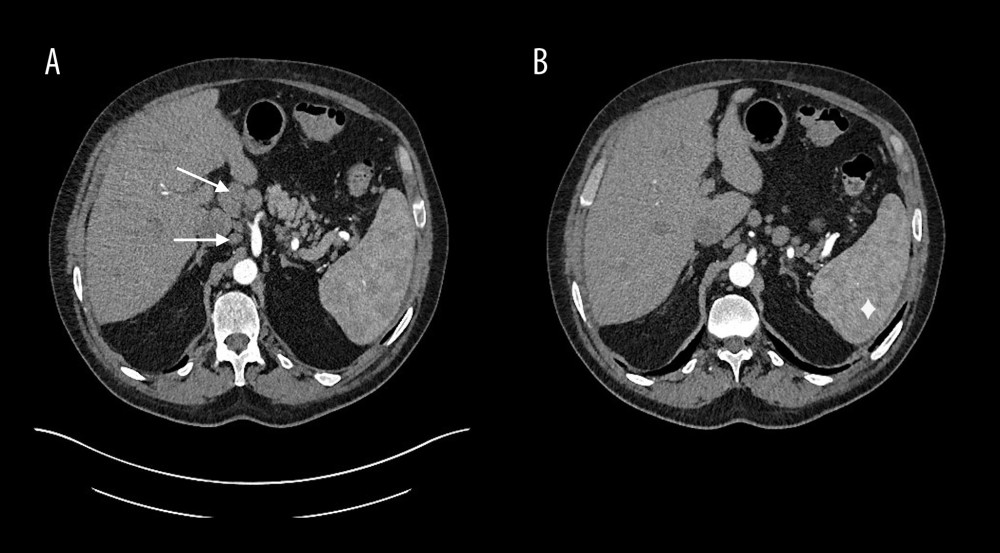 Figure 3. (A, B) CT scans performed on admission to our hospital. The image presents CT of the abdomen performed on admission in October 2023. The enlargement of the spleen and lymphadenopathy are shown. The diamond has been placed to show the spleen, while the arrows point to abnormal lymph nodes.
Figure 3. (A, B) CT scans performed on admission to our hospital. The image presents CT of the abdomen performed on admission in October 2023. The enlargement of the spleen and lymphadenopathy are shown. The diamond has been placed to show the spleen, while the arrows point to abnormal lymph nodes.  Figure 4. Leukocyte count progression over time. The chart illustrates the patient’s white blood cell (WBC) leukocyte counts, emphasizing the persistent leukopenia observed throughout disease progression. Despite fluctuations, the continued decline in WBC counts, coupled with the emergence of thrombocytopenia, contributed to the clinical suspicion of an underlying hematological disorder. Key diagnostic and clinical events are mapped alongside laboratory findings to demonstrate their correlation with disease evolution.
Figure 4. Leukocyte count progression over time. The chart illustrates the patient’s white blood cell (WBC) leukocyte counts, emphasizing the persistent leukopenia observed throughout disease progression. Despite fluctuations, the continued decline in WBC counts, coupled with the emergence of thrombocytopenia, contributed to the clinical suspicion of an underlying hematological disorder. Key diagnostic and clinical events are mapped alongside laboratory findings to demonstrate their correlation with disease evolution. References
1. Chung BY, Um JY, Kim JC, Pathophysiology and treatment of pruritus in elderly: Int J Mol Sci, 2020; 22(1); 174
2. Makar M, Smyth B, Brennan F, Chronic kidney disease-associated pruritus: A review: Kidney Blood Press Res, 2021; 46(6); 659-69
3. Skrzypczak T, Skrzypczak A, Nockowski P, Szepietowski J, Identification and management of CKD-associated pruritus: Current insights: Int J Nephrol Renov Dis, 2024; 17; 339-54
4. Shirazian S, Aina O, Park Y, Chronic kidney disease-associated pruritus: Impact on quality of life and current management challenges: Int J Nephrol Renov Dis, 2017; 10; 11-26
5. Agarwal P, Garg V, Karagaiah P, Chronic kidney disease-associated pruritus: Toxins, 2021; 13(8); 527
6. Aresté N, Sanchez-Alvarez JE, Prieto-Velasco M, Prevalence and severity of pruritus in Spanish patients with chronic kidney disease and impact on quality of life: A cross-sectional study: Clin Kidney J, 2023; 16(6); 1035-37
7. Mack MR, Kim BS, The itch–scratch cycle: A neuroimmune perspective: Trends Immunol, 2018; 39(12); 980-91
8. Ko MJ, Peng YS, Wu HY, Uremic pruritus: Pathophysiology, clinical presentation, and treatments: Kidney Res Clin Pract, 2023; 42(1); 39-52
9. Manenti L, Leuci E, Do you feel itchy? A guide towards diagnosis and measurement of chronic kidney disease-associated pruritus in dialysis patients: Clin Kidney J, 2021; 14(Suppl 3); i8-i15
10. Sutaria N, Adawi W, Goldberg R, Itch: Pathogenesis and treatment: J Am Acad Dermatol, 2022; 86(1); 17-34
11. Cheng AY, Wong LS, Uremic pruritus: From diagnosis to treatment: Diagnostics, 2022; 12(5); 1108
12. Sanchez-Alvarez E, Goicoechea M, Lanot A, The prevalence of chronic kidney disease-associated pruritus and its impact on quality of life in hemodialysis patients: A commentary from experts from two countries: Clin Kidney J, 2024; 17(1); sfae003
13. Hu X, Sang Y, Yang M, Prevalence of chronic kidney disease-associated pruritus among adult dialysis patients: A meta-analysis of cross-sectional studies: Medicine (Baltimore), 2018; 97(21); e10633
14. Rayner HC, Larkina M, Wang M, International comparisons of prevalence, awareness, and treatment of pruritus in people on hemodialysis: Clin J Am Soc Nephrol, 2017; 12(12); 2000-7
15. Marcello M, Marturano D, Ronco C, Zanella M, The role of blood purification therapies in the treatment of chronic kidney disease-associated pruritus: A systematic review: Clin Kidney J, 2024; 17(9); sfae266
16. Ozen N, Cinar FI, Askin D, Mut D, Uremic pruritus and associated factors in hemodialysis patients: A multi-center study: Kidney Res Clin Pract, 2018; 37(2); 138-47
17. Ahdoot RS, Kalantar-Zadeh K, Burton JO, Lockwood MB, Novel approach to unpleasant symptom clusters surrounding pruritus in patients with chronic kidney disease and on dialysis therapy: Curr Opin Nephrol Hypertens, 2022; 31(1); 63-71
18. Yosipovitch G, Chronic pruritus: A paraneoplastic sign: Dermatol Ther, 2010; 23(6); 590-96
19. Lamb YN, Difelikefalin in pruritus associated with chronic kidney disease: A profile of its use: Drugs Ther Perspect, 2022; 38(10); 423-30
20. Corlu L, Rioux-Leclercq N, Ganard M, Renal dysfunction in patients with direct infiltration by B-cell lymphoma: Kidney Int Rep, 2019; 4(5); 688-97
21. Peshin S, Modi S, Kolagatla S, Moka N, CLL-033 an unusual case of renal infiltration in chronic lymphocytic leukemia: Clin Lymphoma Myeloma Leuk, 2024; 24; S340-S41
22. Strati P, Nasr SH, Leung N, Renal complications in chronic lymphocytic leukemia and monoclonal B-cell lymphocytosis: The Mayo Clinic experience: Haematologica, 2015; 100(9); 1180-88
23. Van Der Willik EM, Lengton R, Hemmelder MH, Itching in dialysis patients: Impact on health-related quality of life and interactions with sleep problems and psychological symptoms – results from the RENINE/PROMs registry: Nephrol Dial Transplant, 2022; 37(9); 1731-41
24. Lelonek E, Matusiak Ł, Wróbel T, Szepietowski JC, Aquagenic pruritus in polycythemia vera: clinical characteristics: Acta Derm Venereol, 2018; 98(5); 496-500
25. Welz-Kubiak K, Reszke R, Szepietowski JC, Pruritus as a sign of systemic disease: Clin Dermatol, listopad, 2019; 37(6); 644-56
26. Saini KS, Patnaik MM, Tefferi A, Polycythemia vera-associated pruritus and its management: Eur J Clin Invest, 2010; 40(9); 828-34
27. Das S, Common cutaneous manifestations in hematological malignancies: J Hematol Allied Sci, 2025; 5; 40-46
28. Deng J, Parthasarathy V, Adawi W: JAMA Dermatol, 2022; 158(7); 791
29. Mackintosh L, Busby A, Farrington K, Impact of the COVID-19 pandemic on services for patients with chronic kidney disease: Findings of a national survey of UK kidney centres: BMC Nephrol, 2023; 24(1); 356
30. Natale P, Zhang J, Scholes-Robertson N, The impact of the COVID-19 pandemic on patients with CKD: Systematic review of qualitative studies: Am J Kidney Dis, 2023; 82(4); 395-409e1
31. Nie G, Sun L, Zhang C, Clinicopathological features and individualized treatment of kidney involvement in B-cell lymphoproliferative disorder: Front Immunol, 2022; 13; 903315
32. Gordon MJ, Ferrajoli A, Unusual complications in the management of chronic lymphocytic leukemia: Am J Hematol, 2022; 97(Suppl 2); S26-S34
33. Sugiura H, Sezaki N, Ishikawa T, Successful treatment of relapsed chronic lymphocytic leukemia with venetoclax in a patient with severe chronic kidney disease: Clin Case Rep, 2022; 10(4); e05735
34. Steinhoff M, Cevikbas F, Ikoma A, Berger TG, Pruritus: Management algorithms and experimental therapies: Semin Cutan Med Surg, 2011; 30(2); 127-37
35. De Sequera P, Martínez-Sesmero JM, Romo I, Unmet needs in the management of chronic kidney disease-associated pruritus and the characteristics of the ideal treatment: A Spanish cross-sectional survey from a multidisciplinary perspective: J Clin Med, 2025; 14(2); 624
36. Aucella F, Zerbi S, Monaco MP, Difelikefalin for CKD-aP: Real world evidence of efficacy and safety in Italian patients: Clin Kidney J, 2025; 18(9); sfaf050
37. Suzuki Y, Koya J, Ebisawa K, Sequential development of monoclonal B cell lymphocytosis-derived small lymphocytic lymphoma and plasma cell leukemia: Ann Hematol, 2018; 97(5); 917-19
38. Soldarini M, Farina L, Genderini A, Bolli N, A rare case of atypical chronic lymphocytic leukaemia presenting as nephrotic syndrome: BMJ Case Rep, 2017; 2017; bcr2016218850
39. Wynsberghe MV, Lenain P, Drieux F, Monoclonal B lymphocytosis and minimal change disease: A new monoclonal B-cell disorder of renal significance?: J Nephrol, 2018; 31(2); 317-20
40. Strati P, Shanafelt TD, Monoclonal B-cell lymphocytosis and early-stage chronic lymphocytic leukemia: Diagnosis, natural history, and risk stratification: Blood, 2015; 126(4); 454-62
41. Plessi J, Mori G, Magistroni R, Cappelli G, Monoclonal B lymphocytosis in a kidney transplant recipient: BMJ Case Rep, 2021; 14(6); e242889
42. Wanchoo R, Bernabe Ramirez C, Barrientos J, Jhaveri KD, Renal involvement in chronic lymphocytic leukemia: Clin Kidney J, 2018; 11(5); 670-80
43. Steiger S, Rossaint J, Zarbock A, Anders HJ, Secondary immunodeficiency related to kidney disease (SIDKD) – definition, unmet need, and mechanisms: J Am Soc Nephrol, 2022; 33(2); 259-78
44. Xiang FF, Zhu JM, Cao XS, Lymphocyte depletion and subset alteration correlate to renal function in chronic kidney disease patients: Ren Fail, 2016; 38(1); 7-14
Figures
Figure 1. Severe linear excoriations on the patient’s calves, attributed to chronic pruritus. The photograph was taken during the most recent admission in May 2024, at a time when pruritus had slightly decreased. The distribution and morphology of the lesions suggest a secondary etiology, consistent with CKD-aP. The absence of primary dermatologic pathology supports a systemic origin.Figure 2. Diagnostic process and findings revealed during PD control admissions. This illustrates the chronological appearance of the symptoms found in our patient, presented in the order and timing of each manifestation as they were first reported, with the starting date being the peritoneal dialysis catheter insertion.Figure 3. (A, B) CT scans performed on admission to our hospital. The image presents CT of the abdomen performed on admission in October 2023. The enlargement of the spleen and lymphadenopathy are shown. The diamond has been placed to show the spleen, while the arrows point to abnormal lymph nodes.Figure 4. Leukocyte count progression over time. The chart illustrates the patient’s white blood cell (WBC) leukocyte counts, emphasizing the persistent leukopenia observed throughout disease progression. Despite fluctuations, the continued decline in WBC counts, coupled with the emergence of thrombocytopenia, contributed to the clinical suspicion of an underlying hematological disorder. Key diagnostic and clinical events are mapped alongside laboratory findings to demonstrate their correlation with disease evolution. Tables
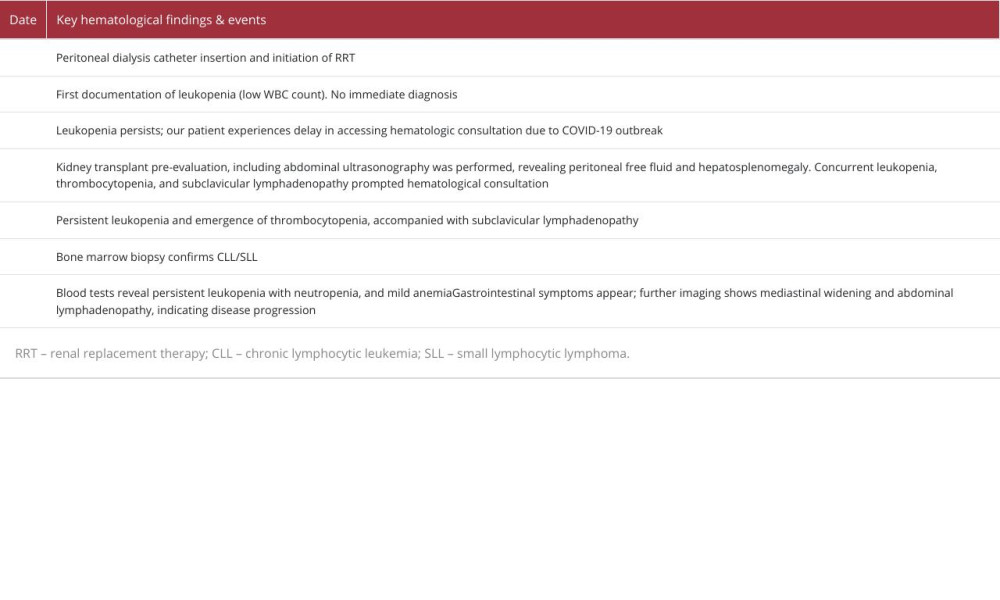 Table 1. Timeline of key hematological findings and disease symptoms evolution. The table illustrates the chronological evolution of hematologic abnormalities in the patient, highlighting the persistence of leukopenia, the emergence of thrombocytopenia, and the discovery of generalized lymphadenopathy. Key diagnostic milestones, including imaging findings and bone marrow biopsy confirmation of CLL/SLL, are mapped against the patient’s clinical symptoms and systemic manifestations.Table 1. Timeline of key hematological findings and disease symptoms evolution. The table illustrates the chronological evolution of hematologic abnormalities in the patient, highlighting the persistence of leukopenia, the emergence of thrombocytopenia, and the discovery of generalized lymphadenopathy. Key diagnostic milestones, including imaging findings and bone marrow biopsy confirmation of CLL/SLL, are mapped against the patient’s clinical symptoms and systemic manifestations.
Table 1. Timeline of key hematological findings and disease symptoms evolution. The table illustrates the chronological evolution of hematologic abnormalities in the patient, highlighting the persistence of leukopenia, the emergence of thrombocytopenia, and the discovery of generalized lymphadenopathy. Key diagnostic milestones, including imaging findings and bone marrow biopsy confirmation of CLL/SLL, are mapped against the patient’s clinical symptoms and systemic manifestations.Table 1. Timeline of key hematological findings and disease symptoms evolution. The table illustrates the chronological evolution of hematologic abnormalities in the patient, highlighting the persistence of leukopenia, the emergence of thrombocytopenia, and the discovery of generalized lymphadenopathy. Key diagnostic milestones, including imaging findings and bone marrow biopsy confirmation of CLL/SLL, are mapped against the patient’s clinical symptoms and systemic manifestations. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133