25 December 2025: Articles 
The Silent Surge: A Case of Rhabdomyolysis-Induced Hypercalcemia
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents
Moath FatehDOI: 10.12659/AJCR.950626
Am J Case Rep 2025; 26:e950626






Abstract
BACKGROUND: Calcium is an essential extracellular cation that the body tightly regulates for numerous physiological functions. Rhabdomyolysis typically causes hypocalcemia due to calcium sequestration within damaged muscle tissue. However, in rare cases, it can progress to hypercalcemia, particularly during the recovery phase, often in patients with concurrent acute kidney injury.
CASE REPORT: A 48-year-old man with no prior medical or surgical history was admitted to the hospital after he had been found unresponsive at home. His initial toxicology screen revealed the presence of cocaine, fentanyl, and benzodiazepines. He was diagnosed with rhabdomyolysis complicated by acute kidney injury and left upper arm compartment syndrome, requiring emergent fasciotomy and renal replacement therapy. During hospitalization, he developed peritonitis secondary to bowel perforation, which warranted laparotomy. Six weeks later, he presented with nausea, vomiting, and constipation, leading to diagnosis of severe hypercalcemia (serum calcium level, 15.3 mg/dL [reference, 8.9-10.2 mg/dL]; albumin-corrected calcium level, 16.7 mg/dL). The patient received intravenous fluids and diuretics, followed by denosumab, which resulted in normalization of calcium levels and resolution of symptoms.
CONCLUSIONS: Rhabdomyolysis may initially present with severe hypocalcemia, followed by delayed hypercalcemia due to calcium sequestration and subsequent release from necrotic muscle tissue. In the present case, delayed hypercalcemia was successfully managed with intravenous fluids, diuretics, and denosumab. Recognition of this delayed pattern is critical for accurate diagnosis and appropriate management. Our patient exhibited a particularly delayed presentation of hypercalcemia and displayed an exceptionally high calcium level.
Keywords: rhabdomyolysis, Hypercalcemia, Renal Replacement Therapy, Endocrine System, Humans, Male, Middle Aged, Acute Kidney Injury
Introduction
Rhabdomyolysis is a clinical syndrome characterized by the breakdown of skeletal muscle cells, leading to the release of intracellular contents – including myoglobin, potassium, and phosphate – into the bloodstream [1]. Calcium behaves differently in this context because it typically becomes sequestered within necrotic or injured myocytes, resulting in hypocalcemia. However, in rare cases with unclear etiology, calcium may subsequently leak back into the circulation, leading to hypercalcemia [2].
Hypercalcemia is a rare but clinically significant late complication of rhabdomyolysis and acute kidney injury [3]. Although most reported cases describe the onset of hypercalcemia within days to a few weeks after the initial insult, the occurrence of substantially delayed hypercalcemia beyond 4 weeks is especially uncommon and poses diagnostic challenges. Failure to recognize this atypical timeline can result in unnecessary investigations and delays in appropriate treatment. Increased awareness of this rare but important phenomenon facilitates accurate diagnosis, optimizes patient management, and reduces the risk of misdiagnosis and overtreatment [4,5].
Here, we describe a 48-year-old man who developed profound hypercalcemia 6 weeks after rhabdomyolysis and acute kidney injury requiring renal replacement therapy. To our knowledge, the delayed hypercalcemia after rhabdomyolysis in this case is among the rarest instances reported; the patient’s exceptionally high calcium level is among the highest in published literature [6].
Case Report
A 48-year-old man with unremarkable medical and surgical history was admitted to the hospital after he had been found unresponsive at home. Cardiopulmonary resuscitation was initiated, and return of spontaneous circulation was achieved after 15 min. A drug overdose was suspected; toxicology screening showed the presence of cocaine, fentanyl, and benzodiazepines. On admission, he was diagnosed with rhabdomyolysis complicated by hyperkalemia, hypocalcemia, and acute kidney injury requiring continuous renal replacement therapy. He also exhibited left upper extremity compartment syndrome, with creatine kinase levels reaching 172 270 U/L (reference, 49–320 U/L) and compartment pressures exceeding 30 mm Hg; he required urgent fasciotomy. His hospital course was further complicated by bowel perforation requiring emergent exploratory laparotomy and bowel resection. Pathologic evaluation revealed peritonitis due to
An abdominal computed tomography scan (Figure 1) to identify abscesses revealed moderate ascites and peritoneal thickening consistent with peritonitis. Peripheral calcification was observed in the left gluteal musculature, with mild calcification involving the right gluteal region and the anterior abdominal wall musculature along the midline near the pubic symphysis. No evidence of lymphadenopathy or granuloma was noted.
The patient’s mental status improved after appropriate treatment. While undergoing dialysis, his calcium levels remained low but began to rise after completion of continuous renal replacement therapy; they continued to increase for more than 1 week despite intravenous fluid administration. The endocrinology service was consulted 10 days after continuous renal replacement therapy cessation for unexplained severe hypercalcemia (serum calcium level, 15.3 mg/dL [reference, 8.9–10.2 mg/dL]; albumin-corrected calcium level, 16.7 mg/dL). At the time of consultation, the patient was alert and oriented. He reported nausea, vomiting, and constipation but denied abdominal pain, polydipsia, polyuria, or bone pain. Further evaluation included measurement of parathyroid hormone, vitamin D levels, and other laboratory studies (Table 1). The 1,25-dihydroxy vitamin D result was pending at that time. Laboratory data indicated non-parathyroid hormone-mediated hypercalcemia. Alternative causes, including multiple myeloma, vitamin D intoxication, and medication-induced hypercalcemia, were excluded.
Uncommon etiologies were also considered, including vitamin D-mediated hypercalcemia secondary to fungal infection. A trial of prednisone 40 mg daily was initiated and continued for 2 days but did not result in clinically significant improvement; thus, it was discontinued. Subsequent laboratory findings indicated a 1,25-dihydroxy vitamin D level below 5.0 pg/mL (reference, 19.9–79.3 pg/mL), confirming that the hypercalcemia was not mediated by vitamin D. Given the patient’s clinical presentation of rhabdomyolysis, non-vitamin D-mediated hypercalcemia, and prior computed tomography evidence of muscular calcifications, a diagnosis of post-rhabdomyolysis hypercalcemia was made.
Supportive measures, including intravenous fluids and diuretics to promote calcium excretion, were continued. Due to persistent and prolonged hypercalcemia, denosumab 60 mg was administered with careful monitoring of renal function; calcium levels normalized by day 3 after administration (Figure 2). Laboratory findings at discharge are summarized in Table 2, and the overall clinical course is illustrated in Figure 3. The patient was subsequently discharged in stable condition.
Discussion
Delayed hypercalcemia after rhabdomyolysis is exceedingly rare and may complicate diagnosis, leading to misclassification and unnecessary interventions. Most reports describe hypercalcemia as developing within 2 to 4 weeks after rhabdomyolysis [7]; however, in the present case, calcium elevation occurred after a particularly prolonged interval. To date, only 2 similar cases have been documented since publication of the earliest reports [4,5], underscoring the need for continued clinical vigilance even several weeks after the initial episode. In our patient, severe hypercalcemia (serum calcium level, 15.3 mg/dL; albumin-corrected calcium level, 16.7 mg/dL) was detected 6 weeks after admission for rhabdomyolysis. This represents an exceptionally elevated calcium level associated with rhabdomyolysis-induced hypercalcemia; the highest documented value was 20 mg/dL [6].
Hypercalcemia constitutes an elevated serum calcium concentration commonly encountered in clinical practice. The condition is primarily regulated by parathyroid hormone and may present with diverse manifestations, including bone pain, nephrolithiasis, abdominal discomfort, depression, and constipation [8,9]. The predominant causes of hypercalcemia – comprising more than 90% of cases – are primary hyperparathyroidism and malignancy [8,10]. Rhabdomyolysis, a condition characterized by skeletal muscle breakdown secondary to injury, represents an uncommon and poorly understood cause of hypercalcemia. It typically presents with initial hypocalcemia, followed by subsequent rebound hypercalcemia during recovery [7].
Extensive workups were performed to identify the underlying cause of hypercalcemia in our patient. Serum protein electrophoresis (SPEP) and urine protein electrophoresis (UPEP) results were both normal, indicating that multiple myeloma was unlikely. To exclude granulomatous disease, we conducted imaging and physical examinations of the lymph nodes, which revealed no evidence of lymphadenopathy or granuloma. Furthermore, the patient’s low 1,25-dihydroxyvitamin D level (<5 pg/mL) indicated that hypercalcemia was not mediated by vitamin D. Therefore, infectious causes such as
In our patient, computed tomography demonstrated calcification in the gluteal region and anterior abdominal wall musculature. In 2016, bone scintigraphy was performed in a case of hypercalcemia after simvastatin-induced rhabdomyolysis; it revealed multiple areas of uptake in the muscles and soft tissue of the chest wall and upper and lower extremities [1]. Similar imaging findings have been reported in 2 additional cases using technetium-99m medronate (MDP) [11] and technetium-99m pyrophosphate [12].
Our patient had multiple complications, including acute kidney injury, compartment syndrome, and fungal peritonitis, consistent with prior reports that acute kidney injury commonly accompanies rhabdomyolysis and substantially contributes to morbidity [13,14]. A previous report described trauma-induced rhabdomyolysis complicated by hypercalcemia and acute kidney injury that was successfully treated with intravenous fluids, calcitonin, pamidronate, and a single hemodialysis session involving calcium-free dialysate [6]. In our case, serum calcium became normalized with intravenous fluids and furosemide, followed by denosumab, in conjunction with continuous renal replacement therapy. Another report of simvastatin-induced rhabdomyolysis-associated hypercalcemia required calcitonin, zoledronic acid, and hemodialysis for correction [1]. Table 3 summarizes reported cases of delayed hypercalcemia after rhabdomyolysis.
The present case highlights the importance of recognizing delayed hypercalcemia after rhabdomyolysis, particularly in the setting of acute kidney injury. Early recognition may improve symptoms and mitigate renal impairment. We recommend close monitoring of calcium levels in patients with rhabdomyolysis and maintaining suspicion for hypercalcemia even when onset is delayed. Although intravenous fluid administration remains the primary treatment, monoclonal antibody therapy such as denosumab, along with appropriate diuretics, may help to regulate calcium levels and alleviate symptoms.
Conclusions
Rhabdomyolysis may present with a biphasic calcium pattern, beginning with severe hypocalcemia due to sequestration of calcium within necrotic muscle tissue and later progressing to hypercalcemia as calcium reenters the bloodstream. Recognition of this delayed onset is essential to guide diagnosis and management and to exclude other etiologies such as malignancy and endocrine disorders. Awareness of this rare and silent surge in calcium emphasizes the need for continued monitoring to aid diagnosis and prevent unnecessary interventions.
Figures
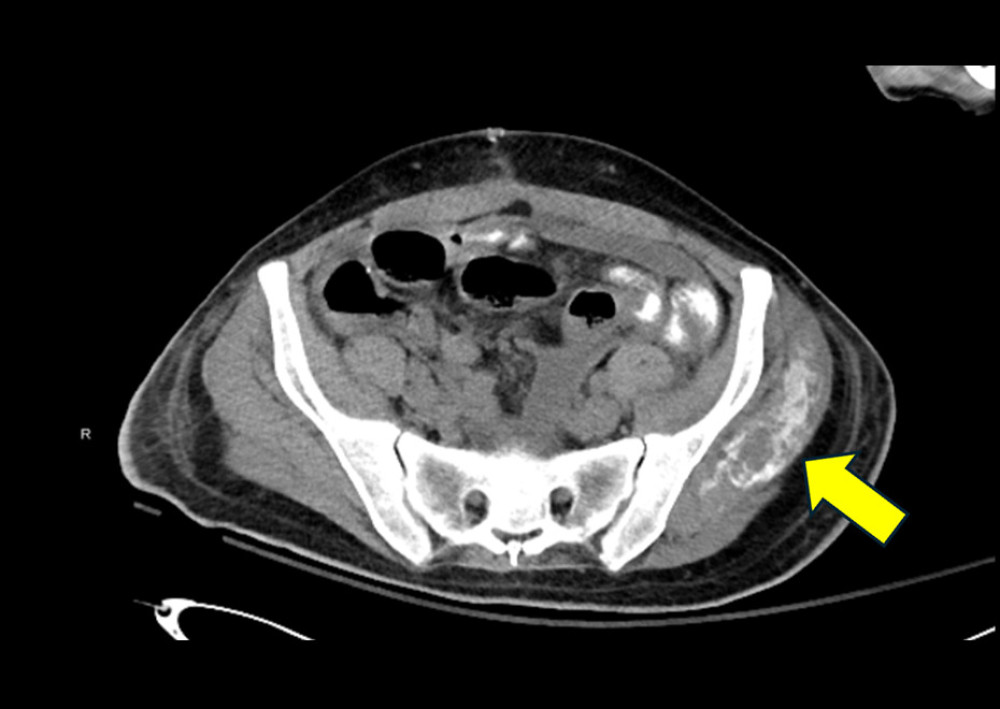 Figure 1. Abdominal computed tomography scan. Yellow arrow indicates substantial calcification in the left gluteal region. Note the mild calcification in the anterior abdominal wall musculature.
Figure 1. Abdominal computed tomography scan. Yellow arrow indicates substantial calcification in the left gluteal region. Note the mild calcification in the anterior abdominal wall musculature. 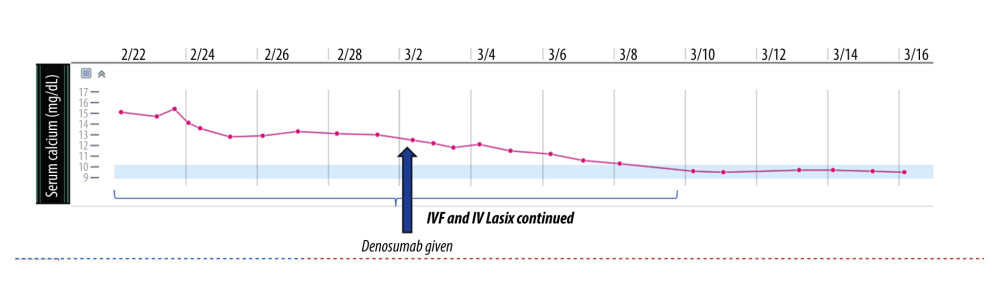 Figure 2. Serum calcium levels during hospitalization, showing gradual normalization. The arrow indicates the timing of denosumab administration. Intravenous fluids (IVF) and intravenous furosemide (IV Lasix) were continued during the indicated period.
Figure 2. Serum calcium levels during hospitalization, showing gradual normalization. The arrow indicates the timing of denosumab administration. Intravenous fluids (IVF) and intravenous furosemide (IV Lasix) were continued during the indicated period. 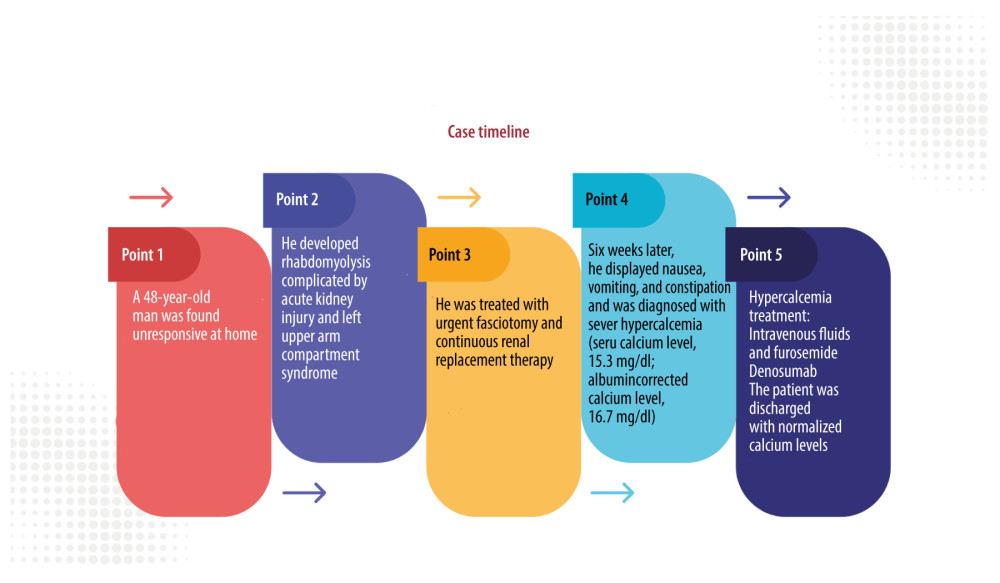 Figure 3. Timeline summarizing the patient’s key clinical events and treatments during hospitalization.
Figure 3. Timeline summarizing the patient’s key clinical events and treatments during hospitalization. References
1. Mirza ZB, Hu S, Amorosa LF, Bone scintigraphy of severe hypercalcemia following simvastatin induced rhabdomyolysis: Clin Cases Miner Bone Metab, 2016; 13(3); 257-61
2. Akmal M, Bishop JE, Telfer N, Hypocalcemia and hypercalcemia in patients with rhabdomyolysis with and without acute renal failure: J Clin Endocrinol Metab, 1986; 63(1); 137-42
3. Meneghini LF, Oster JR, Camacho JR, Hypercalcemia in association with acute renal failure and rhabdomyolysis. Case report and literature review: Miner Electrolyte Metab, 1993; 19(1); 1-16
4. Ikechi D, Koga Y, Harada K, A case of delayed hypercalcemia during diuretic phase of acute kidney injury due to rhabdomyolysis: Evaluation of heterotopic calcification by serial CT: J Jpn Soc Intensive Care Med, 2022; 29(2); 141-45
5. Feinstein EI, Akmal M, Telfer N, Massry SG, Delayed hypercalcemia with acute renal failure associated with nontraumatic rhabdomyolysis: Arch Intern Med, 1981; 141(6); 753-55
6. Hechanova LA, Sadjadi SA, Severe hypercalcemia complicating recovery of acute kidney injury due to rhabdomyolysis: Am J Case Rep, 2014; 15; 393-96
7. Omata K, Fukasawa H, Kaneko M, Hypercalcemia complicated by rhabdomyolysis and acute kidney injury: Cureus, 2025; 17(3); e80177
8. Zawada ET, Lee DB, Kleeman CR, Causes of hypercalcemia: Postgrad Med, 1979; 66(4); 91-97
9. Du Y, Ma C, Shang Z, Secular trends of vitamin D and calcium intake and their circulating levels in US adults from 2007 to 2018: Front Nutr, 2025; 12; 1538019
10. Motlaghzadeh Y, Bilezikian JP, Sellmeyer DE, Rare causes of hypercalcemia: 2021 update: J Clin Endocrinol Metab, 2021; 106(11); 3113-28
11. Frymoyer PA, Giammarco R, Farrar FM, Schroeder ET, Technetium Tc 99m medronate bone scanning in rhabdomyolysis: Arch Intern Med, 1985; 145(11); 1991-95
12. Patel R, Mishkin FS, Technetium-99m pyrophosphate imaging in acute renal failure associated with nontraumatic rhabdomyolysis: Am J Roentgenol, 1986; 147(4); 815-17
13. Kumar R, Kumar S, Kumar A, Exercise-induced rhabdomyolysis causing acute kidney injury: A potential threat to gym lovers: Cureus, 2022; 14(8); e28046
14. Subashri M, Sujit S, Thirumalvalavan K, Rhabdomyolysis-associated acute kidney injury: Indian J Nephrol, 2023; 33(2); 114-18
Figures
Figure 1. Abdominal computed tomography scan. Yellow arrow indicates substantial calcification in the left gluteal region. Note the mild calcification in the anterior abdominal wall musculature.Figure 2. Serum calcium levels during hospitalization, showing gradual normalization. The arrow indicates the timing of denosumab administration. Intravenous fluids (IVF) and intravenous furosemide (IV Lasix) were continued during the indicated period.Figure 3. Timeline summarizing the patient’s key clinical events and treatments during hospitalization. Tables
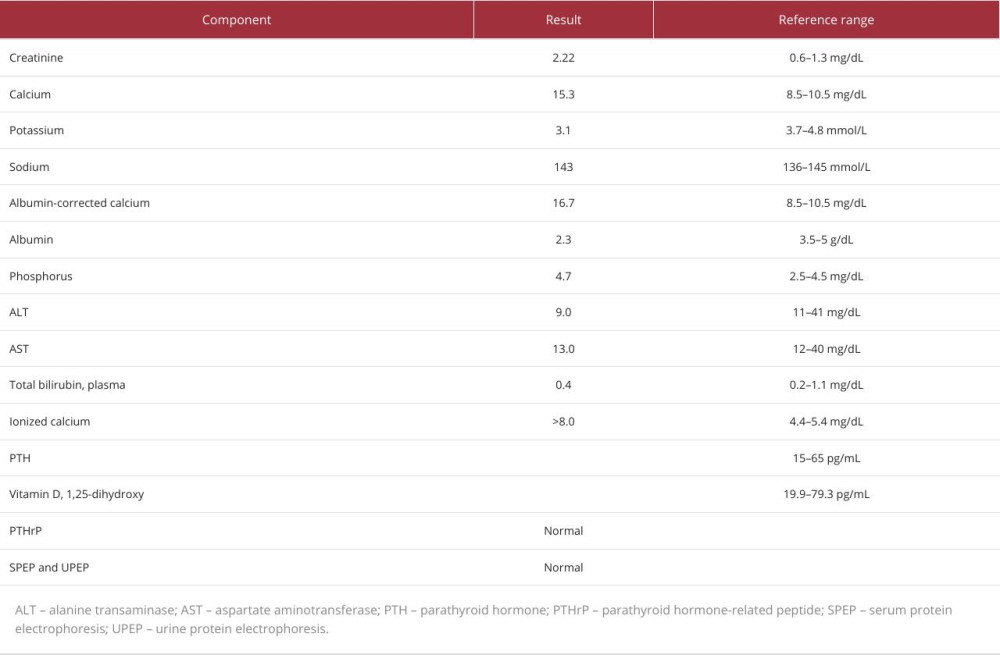 Table 1. Laboratory results during consultation.
Table 1. Laboratory results during consultation.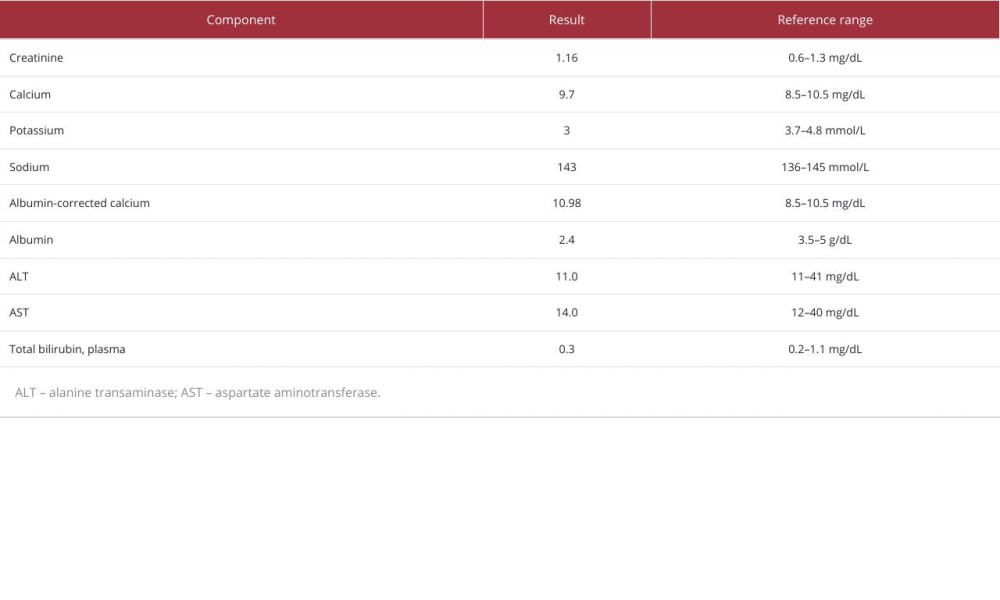 Table 2. Laboratory results at discharge.
Table 2. Laboratory results at discharge.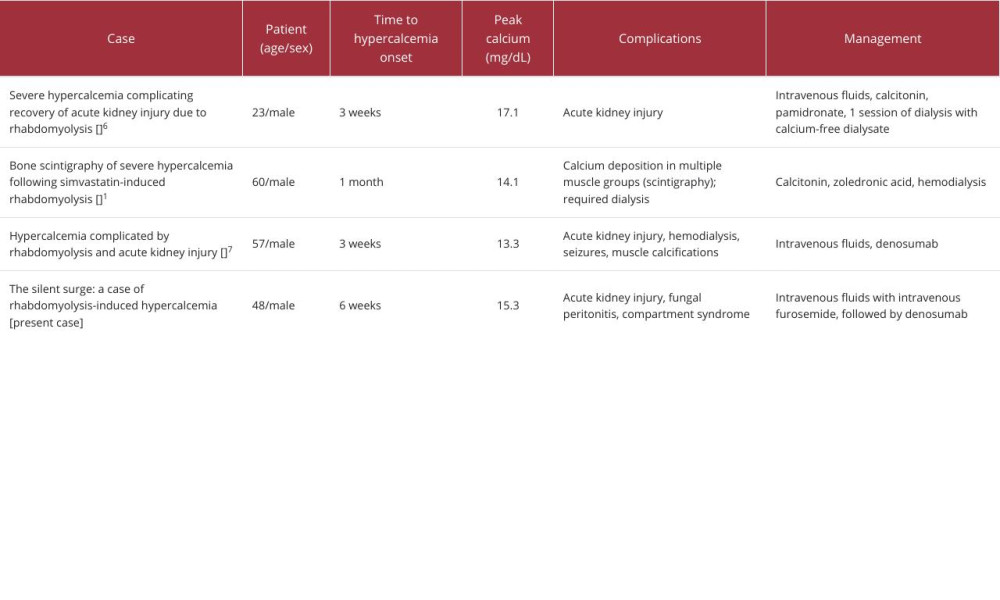 Table 3. Reported cases of delayed hypercalcemia after rhabdomyolysis.Table 1. Laboratory results during consultation.Table 2. Laboratory results at discharge.Table 3. Reported cases of delayed hypercalcemia after rhabdomyolysis.
Table 3. Reported cases of delayed hypercalcemia after rhabdomyolysis.Table 1. Laboratory results during consultation.Table 2. Laboratory results at discharge.Table 3. Reported cases of delayed hypercalcemia after rhabdomyolysis. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133