16 August 2021: Articles 
Pain Neuroscience Education Delivered by a Student Physical Therapist for a Patient with Persistent Musculoskeletal Pain
Unusual or unexpected effect of treatment
Michael O’Connor12ABCDEF, Rob Sillevis12ABDE*, Mark R. Erickson2AEDOI: 10.12659/AJCR.932212
Am J Case Rep 2021; 22:e932212






Abstract
BACKGROUND: Persistent pain is one of the most common reasons individuals seek healthcare in the United States, costing $635 billion annually. At present, the medical literature outlines many treatments for persistent pain. Pain neuroscience education (PNE) is described in the literature as an educational intervention for patients with persistent pain that can be applied by a physical therapist. There is limited research on the application of PNE by a student physical therapist; however, this case report offers a unique opportunity to examine outcomes for this intervention when applied by a student physical therapist in conjunction with manual therapy and therapeutic exercise.
CASE REPORT: This case report examined the outcomes of PNE for a 65-year-old patient with a long-standing history of low back, cervical, shoulder, knee, and foot pain. Interventions included 7 sessions of PNE over 4 weeks delivered by a student physical therapist, in combination with manual therapy and exercise prescribed by a licensed physical therapist. Outcomes measured were fear avoidance belief questionnaire, visual analog scale, Tampa scale of kinesiophobia, neurophysiology of pain questionnaire, neck disability index, and Oswestry disability index.
CONCLUSIONS: Outcomes included clinically significant decreases in subjective pain level, and kinesiophobia; however, there was only a minimal decrease in fear avoidance and no decrease in perceived disability. This case report provides preliminary evidence that positive outcomes can be achieved when PNE is delivered by a student physical therapist combined with manual therapy and therapeutic exercise from an expert clinician for patients with persistent musculoskeletal pain.
Keywords: chronic pain, Physical Therapy Modalities, Teaching, musculoskeletal pain, Pain Measurement, Physical Therapists, Students
Background
Persistent pain, also referred to as chronic pain, [1] contributes to a massive burden on the American population. Fifty million American adults report living with persistent pain and it is the number one reason that individuals seek healthcare [1,2]. The International Association for the Study of Pain (IASP) has defined pain as “an unpleasant sensory or emotional experience associated with, or resembling that associated with, actual or potential tissue damage” [3]. The IASP further defines chronic or persistent pain as pain that has persisted past the point of normal tissue healing, or longer than 3 months [4]. The biomedical model, which correlates tissue damage to pain level, does not adequately explain situations in which tissue damage is no longer present but pain persists [6]. Recent research in pain neurophysiology has advanced theories explaining persistent pain perception in the absence of pathology [1,7,8]. The primary theories cited in the literature emphasize peripheral sensitization, central sensitization, altered central processing of sensory stimuli, and inclusion of contextual factors such as psychosocial, environmental, and cognitive processes around the perception of pain [1,7,8]. Risks factors have been identified that may promote or facilitate or contribute to the development of persistent pain. These include female gender, higher body mass index, incidence of persistent pain in other areas of the body, and psychological factors such as anxiety, depression, and stress [9].
Current evidence-based recommendations for physical therapy management of patients with persistent musculoskeletal pain include patient-centered care, assessment of psychosocial factors, use of imaging with discretion, and incorporation of manual therapy, exercise, and education [10]. More specifically, the education should be intended to explain the neurophysiology of pain to a patient. Pain neuroscience education (PNE) as a modality to educate patients on persistent pain mechanisms has been reported to be useful for reducing pain level, kinesiophobia, and disability, and addressing cognitions related to healthcare use [10,11]. At present, it is difficult to comment on the format of PNE, as studies show heterogenous interventions and outcome measures, which tempers the strength of conclusions that can be drawn [12].
The first pain neuroscience education concepts appeared in the literature in 2002 by Lorimer Moseley [13] in a randomized controlled trial for patients with low back pain. PNE has been given various names, including but not limited to, pain biology education, pain neurophysiology education, and neuroscience education [14,15]. The intervention content varies from author to author, but the main concepts behind the content are uniform [12–15]. Overall, PNE is an educational intervention intended to explain to the patient the concepts of the neurophysiology of pain, nervous system sensitization, spinal inhibitory mechanisms, plasticity of the nervous system, and psychosocial factors that contribute to the persistent pain experience [12–15]. This is completed through a series of inter-treatment educational modules spread throughout an episode of care [12–15]. The modules include face-to-face contact with visual aids, examples, and metaphors to promote patient understanding [12–15]. The duration and frequency of the educational sessions is not uniform in the literature, varying from 30 min to 4 h [12–15].
Pain neuroscience education links the pathoanatomical model of tissue damage and the neurophysiological and psychosocial factors that are inherent in the persistent pain experience [12]. The goal is to help patients reconceptualize their pain experience by providing educational content which can decrease the focus on anatomical damage, reduce fear avoidance, reduce kinesiophobia, and improve self-efficacy [12]. PNE is combined with adjunct therapy treatments such as manual therapy, exercise, and neural mobilization [12]. There are varying opinions on the exact dosage, frequency, and content of a PNE intervention at this time [12].
The literature on PNE has been focused on musculoskeletal pain syndromes in various body regions. The most prevalent research is on low back pain. Studies done by Malfliet et al [16] and King et al [17] indicate that PNE created positive improvements in kinesiophobia, fear avoidance, knowledge of pain neurophysiology, and pain ratings. In a systematic review of PNE for a variety of musculoskeletal pain syndromes, Louw et al [12] found that there are significant changes in fear avoidance, pain self-efficacy, and numeric pain rating with both short- and long-term measures. The literature also supports use of PNE for chronic fatigue syndrome [18].
There are some guidelines on identifying possible factors that indicate the need for PNE [21–23]. Nijs et al [21,22] report central sensitization (CS), rumination, hypervigilance, and high levels of perceived illness all help to determine patients that are likely to benefit from PNE. They also report that there are several markers that indicate the presence or increased risk of CS. This includes specific medical diagnoses such as chronic whip-lash disorders and persistent low back pain, patient reports of hypersensitivity, disproportional pain ratings, and psychosocial factors [21]. Finally, objective measures that indicate CS include hypersensitivity to temperature, sharp, dull, palpation, and pressure pain thresholds both at the site of injury and at remote sites. A survey by Louw et al [23] found that clinicians who regularly perform PNE identified characteristics such as high fear avoidance, CS, and multiple failed treatments as possible prognostic indicators of success with PNE.
The purpose of this case report was to describe the prescription of and outcomes following PNE interventions by a student physical therapist with a patient with multi-regional musculo-skeletal persistent pain.
Case Report
PATIENT HISTORY AND SYSTEMS REVIEW:
The patient was a 65-year-old, mesomorphic, English-speaking woman presenting to physical therapy with multi-regional pain involving the neck and left shoulder developing insidiously 6 weeks prior to initial examination and who had been receiving physical therapy management up to this point. The patient reported neck and shoulder pain that was 6/10 on the 11-point numerical pain rating scale (NPRS). The neck and shoulder pain, which at worst reached a 9/10 on an NPRS scale, had improved minimally over the last 6 weeks and varied in intensity, with a lowest reported pain level of 6/10 and an average pain level of 7/10. According to Smart et al [24], disproportional pain ratings have been implicated in states of CS. The patient reported aggravating factors for her neck and shoulder, included standing, walking for extended periods, transferring from sit to stand, turning the neck while operating a motor vehicle, and reaching overhead to high shelves. The patient had been functionally limited in her activities of daily living (ADL), including recreational gardening, and extended periods of activity such as exercise or cleaning the house. The patient’s level of function was limited based on multi-regional pain. The patient subjectively reported her pain often limited her from activities, and she was afraid to aggravate her condition with physical activity, indicating fear avoidance beliefs. Fear avoidance has been implicated in states of CS [24]. The patient also reported a history of low back and left hip pain starting in 1982, as well as left lateral foot pain. The patient rated her low back and left hip pain as 4/10 at the time of examination. Her left lateral foot pain was rated 4/10 at the time of examination.
Her past medical history included a motor vehicle accident that occurred in 1982 followed by multiple lumbar surgeries including laminectomy and fusion from L1 to S1, left anterior cruciate ligament reconstruction, osteoarthritis of bilateral knees, fibromyalgia, hypertension, asthma, and blepharospasm. The patient’s goal was to reduce pain, improve range of motion in her left shoulder, and be able to perform gardening for extended periods. Yellow flags included fear avoidance behaviors, high subjective pain ratings, and multiple regions of reported pain. A review of systems revealed no medical red flags.
EXAMINATION:
To obtain an objective measure of her upright posture, the craniovertebral angle (the angle between a line from the spinous process of C7 to the meatus of the ear and a horizontal line from C7) was determined, which was 48°. A craniovertebral angle below 53° is considered forward head posture [25]. She displayed an increased thoracic kyphosis and was not able to actively decrease the curve. Cervical active range of motion findings included limitations in all directions, with greatest deficits in left rotation (0–40°), left side bending (0–20°), and extension (0–15°). Active range of motion for left rotation and left side bending provoked pain. Cervical passive range of motion revealed similar limitations, with the greatest deficits in left rotation (0–48°), left side bending (0–25°), and extension (0–21°). Passive range of motion with overpressure revealed a painful end feel in left rotation, left side bending, and extension. Manual muscle testing of the muscles of the cervical spine and the muscles of the shoulder girdle showed strength of 4/5 in all directions. However, the patient was weak and painful in left shoulder abduction and external rotation was graded 3+/5. Passive intervertebral motion testing revealed hypomobility throughout the craniovertebral, lower cervical, and upper thoracic regions for forward bending, left side bending, bilateral rotation, and backward bending. Cervical quadrant, distraction, compression, and upper limb neural tension test for the median nerve were all positive, reproducing her familiar pain in the cervical spine and left arm. Smart et al [26] reported that positive neural tension tests and history of neurological tissue compromise are implicated in states of peripheral neurogenic pain. Palpation revealed tenderness and hypertonicity in the left cervical paraspinals, as well as tenderness of the supraspinatus and biceps long head tendons.
At the onset of treatment using PNE, the visual analog scale (VAS) was used to determine subjective pain rating. This scale is valid and reliable for pain measurement for persistent musculoskeletal pain [27]. At the time of initial outcome measurement, the patient reported 61 mm out of a 100 mm scale on the VAS. Her fear avoidance beliefs questionnaire (FABQ) score was 35/96, indicating the patient was fear-avoidant of physical activity and work-related duties. Cleland and Fritz [28] determined the FABQ is valid for measurement of fear associated with musculoskeletal damage and is able to differentiate tissue damage from psychological processes of fear related to physical activity and work. The FABQ physical activity subsection score was 20/24, and the FABQ work subsection score was 12/42. The FABQ physical activity subsection score indicates the patient correlates high levels of fear avoidance behaviors with physical activity such as exercise or ADLs [28]. The patient had been retired for several years; therefore, the FABQ work subsection was not relevant. This could account for the low score in the work subsection in the initial measure, indicating a low level of fear avoidance. There is varying research on cut off scores using the FABQ. Recently, Williams [29] indicated patients with a score greater than 15/24 on the FABQ physical activity scale may benefit from cognitive behavioral approaches such as PNE. The Tampa Scale of Kinesiophobia (TSK) score was 49/68 with a cut off score of 35/68, indicating a high level of kinesiophobia as reported by Meier et al [30]. According to Lundberg et al [30], this scale measures fear associated with movement that is not region-specific. The Oswestry Disability Index (ODI) score was 62% disability, which placed her in the “crippled” category [32]. The ODI has been deemed valid and reliable for measuring perceived disability in populations with low back pain [33]. The Neck Disability Index (NDI) score was 58% perceived disability, which placed her in the “severely disabled” category [34]. The Neurophysiology of Pain Questionnaire (NPQ) score was 9/19. The NPQ measures the patients understanding of the biological process of pain. There is limited published research investigating NPQ validity, clinically meaningful change, or the relationship among pain, function, and score [35]. It has been validated in a Rasch analysis to assess patient understanding of the biological mechanisms of their pain and evaluate effects of cognitive behavioral interventions [35]. It has been described by Moseley as a useful measure of patients’ understanding of neurophysio-logical pain concepts [35].
CLINICAL IMPRESSION:
The patient presented with subjective reports that indicated fear avoidance, and a disproportional pain rating both described in the literature as related to CS and persistent pain [24]. The objective tests and measures showed positive test results with neural tissue tension techniques, indicating peripheral neuropathic pain as well [26]. The outcome measures indicated the patient had clinically significant levels of fear avoidance behaviors, kinesiophobia, and low knowledge of pain neurophysiology concepts, while also presenting with high levels of perceived disability from cervical and low back regional disability measures. Based on the information gathered, it was deemed appropriate to provide a PNE intervention for this patient. The rationale for this decision was based on research evidence [12,21,22] indicating that patients presenting with the above findings may benefit from a PNE intervention.
INTERVENTIONS:
The patient was seen for 7 visits over the course of 4 weeks. She was seen on Tuesday and Thursday in the first 3 weeks and on Tuesday in week 4. Each treatment involved a one-onone educational module lasting approximately 15 min with color visual aids to supplement examples given and aid in patient understanding (Table 1) [12]. The PNE content sequence was 1) peripheral sensitization 2) descending inhibition 3) central processing of pain 4) psychosocial overload 5) pain neuromatrix 6) neurogenic inflammation 7) somatosensory smudging 8) biological adaptability 9) threat perception. These modules and sequence were developed by the student physical therapist based on a review of prior literature on PNE interventions [12–15,36]. Each educational module was completed in conjunction with other physical therapy interventions provided by the same licensed clinician, who had 28 years of experience in manual therapy. Treatment interventions included manual therapy, neural mobilizations, trunk stabilization, and strengthening exercises for the upper and lower extremities (Table 1). At each follow-up visit the student physical therapist completed a short verbal review of the previous session’s material to reinforce previously covered material. The student physical therapist also asked about the progression of the patient’s symptoms since last treatment, using this time to reinforce prior concepts in reference to recent events in the patient’s subjective reports. The educational content in each visit was revisited several times during the course of that session, as appropriate.
At the first visit where PNE was applied, the patient was asked if she was interested in learning more about her pain. The patient reported she was interested and accepted the conversation. Analogies to explain the role of the peripheral nervous system and peripheral sensitization were introduced using the analogy of an alarm system with a decreased threshold for danger. Next, the analogy of the ion channels as sensors for different types of afferent information was used to explain how the nervous system receives information. The analogy compared these sensors to an automatic door that opens with motion. This module continued to explain how many factors can be involved in the sensitivity of the nervous system, including stress and movement. The patient responded that she understood the material but felt her situation was different. She cited her extensive past medical history and tissue damage as the reason for her persistent pain. The manual therapy treatment consisted of a supine thoracic manipulation at the T3–4 segments at a Maitland grade 5. Thoracic manipulation has been shown to have positive effects for patients with neck pain, reducing pain, improving dysfunction and posture, and increasing neck ROM [37,38]. Left rotational Sustained Natural Apophyseal Glide (SNAG) targeting C5–6 and C6–7 segments for increased range of motion were performed as well. SNAGs have been shown to be a safe and effective treatment method to restore cervical range of motion [39]. She underwent posterior and inferior glenohumeral joint manipulation at a Maitland grade 4. The patient participated in neural mobilization with a median nerve bias and strength exercises focusing on the deep neck flexors, shoulder abduction, and external rotation. She was instructed in an augmented home exercise program to carry over her treatment effects.
During the second session there was a short review of the initial visit concepts. The patient reported she was feeling sorer today and stated she felt it may be because her nervous system was more sensitive. The session then proceeded with an explanation of the reasons behind spreading pain and a sensitive nervous system, using a similar alarm metaphor. In this case, the alarm cannot be shut off; therefore, nearby areas may become more sensitive as a result. The educational module next focused on the use of exercise as a modality to calm a sensitized nervous system. The patient was educated on the rating of perceived exertion scale and the use of a numerical pain rating scale as a guide for activity. The patient was encouraged to maintain daily physical activity, with the understanding that pain may not correlate to tissue damage [5]. The patient had similar verbal responses to the initial treatment, also citing inflammation as the cause of her persistent pain. The manual therapy treatment this visit consisted of a supine thoracic grade 5 manipulation at the T3–4 segments, left rotational SNAG targeting C5–6 and C6–7 segments, and posterior and inferior glenohumeral joint grade 4 manipulations for the glenohumeral joint. The patient again participated in neural mobilization with a median nerve bias and strengthening exercises focusing core stabilization, deep neck flexor strengthening, left shoulder abduction, and external rotation. Her augmented home exercise program was reviewed and upgraded.
Prior to the third treatment, the patient completed the original outcome measures to track changes in function. At this session, an introduction to the brain’s role in pain was provided. The analogy used explained the brain as the CEO of the body, as it is critical in monitoring afferent information and may become hypersensitive to sensory signals. Next, the concept of descending inhibition was explained, using a wet brain analogy. This analogy explained the role of the endogenous opioid theory and how physical therapy and daily activity is intended to activate this system to modulate the pain experience. The patient reported she understood the concept but felt that her extensive lumbar surgical history changed her situation. She also stated she enjoys physical activity but feels some days she overdoes it and has debilitating soreness in the following days. The therapist took time to encourage activity to create changes in nervous system sensitivity and activation of endogenous mechanisms [40]. The manual therapy interventions during the third visit were the same as in visit 2.
Session 4 began with a discussion of emotional overload and the pain experience. The analogy of a measuring cup was used to explain how emotions such as fear, stress, and anxiety can contribute to the musculoskeletal pain experience. The patient cited her seemingly failed surgical procedures and prior treatments as sources of stress and possibly a source for increased pain perception. Next, an explanation of prolonged stress response and its role in persistent pain occurred. The analogy of a snake entering the patient’s home and following her around was used to explain how elevation of stress-related hormones can alter the perception of sensory information in an adverse way. The example of failed treatments and persistent pain as stressors was used to tie the analogy into the patient’s life experiences. The patient replied that she fully understands how stress can contribute to pain, as she gave recent examples where she found this to be true. The manual therapy intervention was the same as in visit 3, with the addition of a supine thoracic grade 5 manipulation at the T2–3 segments and a seated grade 5 manipulation to the 1st rib on the left. She received her strengthening exercises, and static standing balance activities were added to her program. She was received an augmented home exercise program
The educational module in session 5 focused on neurogenic inflammation and the pain neuromatrix theory. Neurogenic inflammation was explained using the analogy of inflammatory soup at the site of injury. The patient was educated on the mechanisms of neurologically mediated inflammation that may occur with stress and the ability of these inflammatory chemical to induce afferent signals at a level sufficient to reproduce pain [41]. Next, the pain neuromatrix was explained using the analogy of memory. Visual aids demonstrated how the brain creates connections based on previous information that represent the brain’s understanding of stimuli. The comparison of a memory of a loved one and the pain experience as an output from the brain was used. The patient stated she understands the brain must be involved in pain but does not feel she understands how it can be an output. The secondary example of an optical illusion was used to further compare the vision to somatosensory input and compare the role of the brain in these experiences. The manual therapy interventions were the same as in visit 4.
The sixth treatment session made connections of the pain neuro-matrix theory and the motor cortex using the analogy of a road map. The analogy explains how central nervous system centers related to movement may become connected to an individual’s pain neuromatrix signature via neuroplasticity causing the activation of a painful experience in non-threatening motions [41]. The second analogy explained was to reiterate the pain neuromatrix theory and the output of pain experiences from the brain. This analogy used phantom limb pain as an example of the absence of tissue damage can still produce a painful experience. The patient reported she understands the information but is having a hard time staying active at home because of her persistent pain. The manual therapy interventions remained the same. Her augmented home exercise program was reviewed.
At the beginning of the last treatment session, the patient was asked if she had any questions regarding the information that was discussed over the last 6 sessions. The patient replied that she understands how the brain is involved in persistent pain but cited direct tissue damage and inflammation as the 2 main drivers of her pain. The concept of pain as a multisystem experience was reiterated and the goal of this intervention was to give the patient tools to navigate her pain experience and promote function in spite of the seemingly somatic experience she was perceiving. The final analogies included the concept of biological adaptability through the example of callused hands. It was explained that the nervous system adapts to the stresses placed on it with the goal of reducing sensitivity over time with movement-based therapy. Following this, a review of the education provided over the last 7 treatments was completed. The patient reported she understands that pain is complicated, and she feels her situation is different than that of the average person, as she again cites her extensive past medical history, tissue damage, and inflammation as the main drivers of her persistent pain. The manual therapy treatment this visit consisted of a supine thoracic grade 5 manipulation at the T2–4 segments, and posterior and inferior glenohumeral joint grade 4 manipulations for the glenohumeral joint. The patient underwent neural mobilization with a median nerve bias and strengthening exercises focusing on core stabilization, deep neck flexor strengthening, and left shoulder abduction and external rotation. She was instructed to continue participating in her augmented home exercise program.
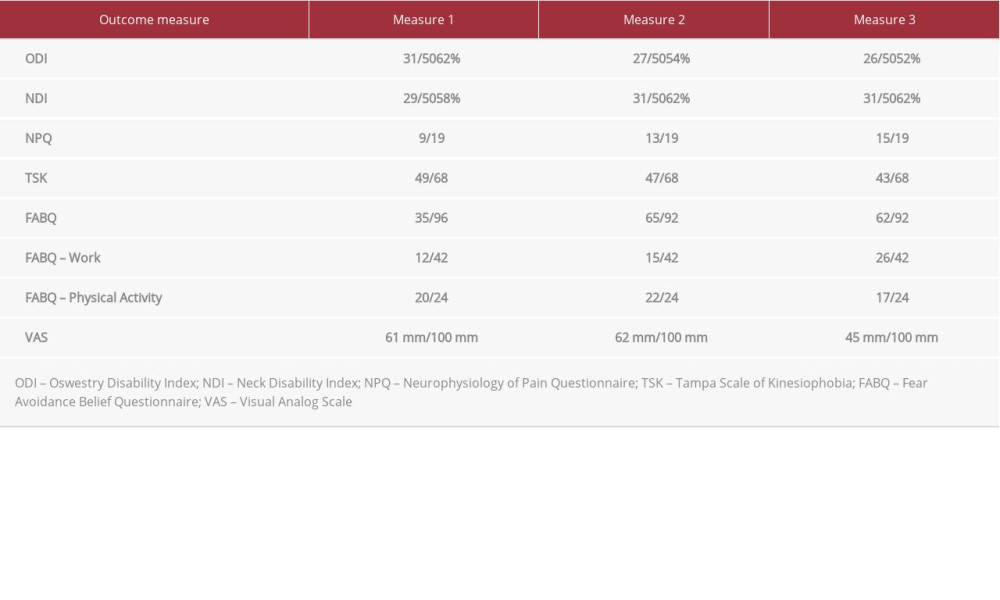
Results
The outcome measures were completed at the beginning of the treatment period, at visit 3 midway through the treatment period, and at the final treatment session (Table 2). Overall, there were clinically meaningful changes in VAS and TSK scores. The ODI, FABQ, and NDI showed no clinically significant changes. The NPQ showed a steady improvement; however, it is difficult to determine whether this change is significant because MCID has not been determined for the NPQ [35]. Visual analog scale pain rating decreased 26%, or 16 millimeters, which meets the minimal clinical important difference (MCID) threshold of 7 millimeters as reported by Carlsson [27]. The ODI decreased from 62% to 52%, which does not meet the MCID as reported by Vianin [33]. The FABQ decreased by 4.6% which does not meet the MCID of 30% as reported by Vernon et al [34]. There was a clinically significant change in the TSK measure of 12%, or 6 points, which is beyond the threshold of 5.5 points considered a minimal detectable change as reported by Lundberg, indicating a significant change in kinesiophobia [30]. There was steady improvement of pain neurophysiology concepts, from 13 out of 19 to a final measure of 15 out of 19. Again, it is difficult to determine whether this change is significant because MCID has not been determined for the NPQ [35]. NDI score increased for recreational activities and decreased with lifting objects, for no net NDI change overall. Subjective reports indicated the patient maintains thoughts that tissue damage is associated with pain despite indicating changed knowledge of persistent pain mechanisms on the pain neuro-physiology questionnaire.
Discussion
The purpose of this case report was to describe the use of a PNE intervention prescribed by a student physical therapist in combination with manual therapy applied by an experienced clinician with a patient with persistent musculoskeletal pain. PNE has been shown to be helpful in the management of persistent musculoskeletal pain [15,21,20]; however, its effectiveness when applied by a student physical therapist is unreported to date. The patient presented with high levels of kinesiophobia, fear avoidance, and self-perceived disability demonstrated in the subjective history and with more formal outcome measures. She also had an extended history of prior trauma and medical management that may have contributed to the development of persistent pain [42]. Objectively, the patient had diffuse tenderness to palpation at multiple regions, and positive neural tension tests. Hypersensitivity attributes indicate a CS mechanism of pain, which been shown to respond well to PNE [24]. There also appears to be peripheral neurogenic mechanisms of pain indicated with positive upper limb neurological tension test results [26]. The clinical presentation of this patient prompted the student physical therapist to provide a PNE intervention in consultation with the treating physical therapist based on previous literature describing its efficacy [15,21,22,24].
The goal of PNE is to provide patients with tools to reconceptualize their persistent experience and decrease the focus on anatomical damage, reduce fear avoidance, reduce kinesiophobia, and improve self-efficacy [12]. This patient continued to reports pathoanatomical mechanisms of pain, citing inflammation and damaged tissue as the main sources of her persistent pain throughout the PNE treatment sessions. Subjective reports indicated the patient understood and tried to apply the concepts being taught, but did not believe they fit her condition. Despite these reports, there was a clinically significant improvement in kinesiophobia and pain rating after 7 sessions as measured with the TSK and VAS. Based on these results, there seems to be a disconnect between subjective reports and objective measures. PNE represents a modality to create behavior change by encouraging the patient to reconceptualize persistent pain as a sensitive nervous system and attempt to engage in physical activity in spite of subjective reports. In this case, the patient might be showing behavior change in objective measures without demonstrating them in subjective reports.
The transtheoretical model of behavior change is the model used to describe health-related behavioral change [43]. This model was developed by Dr. James Prochaska and Dr. John Norcross in 1977 [43]. They described 5 stages that individuals progress through when creating change in their life. The stages include precontemplation, contemplation, preparation, action, and maintenance. This model has been useful in areas such as smoking cessation, heart disease management, and physical activity in chronic disease states [44]. In the pre-contemplation and contemplation stages, individuals have yet to attempt to make behavior changes and are unlikely to apply PNE concepts to their physical activity. The patient described was likely progressing through the first 2 stages of this model and may have not been ready to make changes to her health habits.
There are many possible reasons that contribute to the lack of results in perceived disability and fear avoidance. It may have been useful for the student physical therapist to have an understanding of behavior change techniques in order to facilitate the progression through these stages of change. This may be an area where research in PNE can expand in order to assist clinicians in understanding which behavioral change methods can be combined with PNE to facilitate the greatest change in health behavior.
Chronic pain is a multifactorial and complex condition that requires multimodal treatment [45]. PNE represents one portion of this patient’s overall care, which also included care from other health care providers outside of physical therapy. If the education a patient receives from all providers includes concepts similar to those outlined in pain neuroscience education, the patient may have contradictory information, leading to limited results in pain severity, kinesiophobia, perceived disability, and behavior change. There is also the limit of the patient’s beliefs of the mechanisms of pain, their perception of health care, biological influences, and psychosocial influences, as these attributes have been linked to persistent musculoskeletal pain [9]. It may be argued that all health care providers should be comfortable with and able to provide pain neuroscience education to possibly improve outcomes and patient knowledge of pain physiology.
The intervention in this case report followed a predetermined progression that was intended to cover all portions of PNE concepts described in other studies [15,21,22]. This limits the intervention, as it was more regimented and may not have fit what the patient specifically needed at each session. In order to better fit each education module, it may be useful to apply the biopsychosocial model as well to better tailor the intervention to each patient. The biopsychosocial model is intended to account for factors outside of body structure and function, activity limitations, and participation restrictions to include contextual aspects such as personal factors and the patient environment [46]. In this case report, the interventions were predetermined in order to ensure that all topics were covered according to the literature [14]. This may have caused the student therapist to miss the implications of the patient’s contextual factors. There may have also been topics that were not readily applicable to the patient’s scenario. In hindsight, a closer examination of the patient’s contextual factors and development of patient specific education modules may have assisted in creating greater change in outcomes.
The PNE literature has delineated the topics that should be covered including concepts of the neurophysiology of pain, nervous system sensitization, spinal inhibitory mechanisms, plasticity of the nervous system, and psychosocial factors that contribute to the persistent pain experience [12]. The analogies used in other reports are inconsistent in description and dosage [12]. This report delineates specific PNE examples, exact number of treatments, and a unique treatment dosage that may be useful in a PNE intervention, and it provides some evidence that PNE can be applied by a novice clinician.
It has been demonstrated that PNE is more beneficial in combination with other interventions [47]. The patient in this case received a combination of PNE with manual therapy and she participated in an active exercise program. The benefit of manual therapy for patients with neck and shoulder pain has been identified in several studies [48,49]. It is not possible to determine in this case to what extend the different interventions resulted in the therapeutic effect. The PNE intervention, manual therapy, or the combination could have contributed to the positive changes in outcome measures.
There are limitations to this case report worth noting. The patient found the questions related to work difficult to answer in the outcome measure questions as she was retired. This might have led to inappropriate measure of change in fear avoidance and perceived disability related to her neck. This case report describes the progression and intervention given to one patient. One must also account for changes in outcome measures that may have been a result of the manual therapy, and exercise interventions. Therefore, the results gained in this study should be interpreted with caution.
Conclusions
This case report describes the use of a PNE intervention applied by a student physical therapist in combination with manual therapy and therapeutic exercise for a patient with multi-regional chronic pain, showing beneficial outcomes. Based on this case report, no determination can be made whether the positive treatment effect was the result of the PNE intervention, manual therapy, or the combination of these two. There were clinically significant improvements in kinesiophobia and visual analog pain rating. There was also an improvement in the patient’s knowledge of pain neurophysiology concepts over the course of treatment. There were no changes in fear avoidance beliefs or in self-perceived disability related to neck and low back pain. Understanding of a patient’s stage of behavior change and biopsychosocial factors is useful in tailoring a PNE intervention to fit a patient’s needs. This case also illustrates the need for further research to determine a clinically beneficial dosage of PNE.

References:
1.. : National Pain Strategy Report: A Comprehensive Population Health-Level Strategy For Pain, 2016, Washington, DC, US Department of Health and Human Services, National Institutes of Health https://www.iprcc.nih.gov/national-pain-strategy-overview/national-pain-strategy-report
2.. Gaskin D, Richard P, The economic cost of chronic pain in the united states: J Pain, 2012; 13; 715-24
3.. Raja S, Carr D, Cohen M, The revised international association for the study of pain definition of pain: Concepts, challenges, and compromises: J Pain, 2020; 161; 1976-82
4.. Merskey H, Bogduk N: Classification of chronic pain, 1994, Seattle (WA), IASP Press
5.. Okada E, Matsumoto M, Fujiwara H, Toyama Y, Disc degeneration of cervical spine on MRI in patients with lumbar disc herniation: A comparison study with asymptomatic volunteers: Eur Spine J, 2011; 20; 585-91
6.. Setchell J, Costa N, Ferreira M, Individuals’ explanation for their persistent or recurrent low back pain: A cross-sectional survey: BMC Musculoskelet Disord, 2017; 18(1); 466
7.. Dubin A, Patapoutian A, Nociceptors: The sensors of the pain pathway: J Clin Invest, 2010; 120; 3760-72
8.. Melzack R, Wall PD, Pain mechanisms: A new theory: Science, 1965; 150; 971-79
9.. McGreevy K, Bottros M, Raja S, Preventing chronic pain following acute pain: Risk factors, preventative strategies, and their efficacy: Eur J Pain Suppl, 2011; 5; 365-76
10.. Lin I, Wiles L, Waller R, What does the best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high quality clinical practice guidelines: Systematic review: Br J Sports Med, 2020; 54(2); 79-86
11.. Wenger S, Drott J, Fillipo R, Reducing opioid use for patients with chronic pain: An evidence based perspective: Phys Ther, 2018; 98; 424-33
12.. Louw A, Zimney K, Puentedura E, Diener I, The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature: Physiother Theory Pract, 2016; 32; 332-55
13.. Mosely L, Combined physiotherapy and education is efficacious for chronic low back pain: Aust J Physiother, 2002; 48; 297-302
14.. King R, Robinson V, Ryan CG, Martin DJ, An exploration of the extent and nature of reconceptualisation of pain following pain neurophysiology education: A qualitative study of experiences of people with chronic musculoskeletal pain: Patient Educ Couns, 2016; 99(8); 1389-93
15.. Meeus M, Nijs J, Oosterwijk J, Pain physiology education improves pain beliefs in patients with chronic fatigue syndrome compared with pacing and self management education: A double blind randomized control trial: Arch Phys Med Rehabil, 2010; 91; 1153-59
16.. Malfliet A, Kregel J, Coppieters I, Effect of pain neuroscience education combined with cognition targeted motor control training on chronic spinal pain a randomized clinical trial: JAMA Neurol, 2018; 75(7); 808-17
17.. King R, Robinson V, Elliott-Button H, Watson J, Pain reconceptualization after pain neurophysiology education in adults with chronic low back pain: A qualitative study: Pain Resear Manag, 2018; 2018; 3745651
18.. Meeus M, Nijs J, Oosterwijk J, Pain physiology education improves pain beliefs in patients with chronic fatigue syndrome compared with pacing and self management education: A double blind randomized control trial: Arch Phys Med Rehabil, 2010; 91; 1153-59
19.. Baert I, Lluch E, Mulder T, Nijs J, Does pre-surgical central modulation of pain influence outcome after total knee replacement? A systematic review: Osteoarthritis Cartilage, 2016; 24; 213-23
20.. Enrique L, Lirios D, Deborah F, Preoperative pain neuroscience education combined with knee joint mobilization for knee osteoarthritis: Clin J Pain, 2018; 34(1); 44-52
21.. Nijs J, Van Houdenhove B, Oostendorp R, Recognition of central sensitization in patients with musculoskeletal pain: Application of pain neurophysiology in manual therapy practice: Man Ther, 2010; 15; 135-41
22.. Nijs J, Paul van Wilgen C, Van Oosterwijck J, How to explain central sensitization to patient with ‘unexplained’ chronic musculoskeletal pain: practice guidelines: Man Ther, 2011; 16; 413-18
23.. Louw A, Puentedura E, Zimney K, The clinical implementation of pain neuroscience education: A survey study: Physiother Theory Pract, 2017; 33; 869-79
24.. Smart K, Blake C, Staines A, Mechanisms-based classifications of mus -culoskeletal pain: part 1 of 3: Symptoms and signs of central sensitization in patients with low back pain (+/−) leg pain: Man Ther, 2012; 17; 336-44
25.. Kim E, Kim J, Correlation between rounded shoulder posture, neck disability indices, and degree of forward head posture: J Phys Ther Sci, 2016; 28(10); 2929-32
26.. Smart K, Blake C, Staines A, Mechanisms-based classifications of musculoskeletal pain: part 2 of 3: Symptoms and signs of peripheral neuropathic pain in patients with low back pain (+/−) leg pain: Man Ther, 2012; 17; 345-51
27.. Carlsson A, Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale: Pain, 1983; 16; 87-101
28.. Cleland J, Fritz J, Childs J, Psychometric properties of the Fear-Avoidance Beliefs Questionnaire and Tampa Scale of Kinesiophobia in patients with neck pain: Am J Phys Med Rehabil, 2008; 87; 109-17
29.. Williamson E, Fear Avoidance Beliefs Questionnaire (FABQ): Aust J Physiother, 2006; 52(2); 149
30.. Lundberg M, Styf J, Carlsson S, A psychometric evaluation of the Tampa Scale for Kinesiophobia – from a physiotherapeutic perspective: Physiother Theory Pract, 2004; 20; 121-33
31.. Meier M, Stämpfli P, Vrana A, Neural correlates of fear of movement in patients with chronic low back pain vs. pain-free individuals: Front Hum Neurosci, 2016; 10; 386
32.. Fairbank JC, Pynsent PB, The Oswestry Disability Index: Spine, 2000; 25; 2940-52
33.. Vianin M, Psychometric properties and clinical usefulness of the Oswestry Disability Index: J Chiropr Med, 2008; 7; 161-63
34.. Vernon H, Mior S, The neck disability index: A study of reliability and validity: J Manip Physiol Ther, 1991; 14; 409-41
35.. Catley M, O’Connell N, Moseley G, How good is the neurophysiology of pain questionnaire? A rasch analysis of psychometric properties: J Pain, 2013; 14; 818-27
36.. Louw A, Schmidt S, Puentedura E, Zimney K: Pain neuroscience education: Teaching people about pain, 2018, Minneapolis (MN), Orthopedic Physical Therapy Products
37.. Dunning JR, Butts R, Mourad F, Upper cervical and upper thoracic manipulation versus mobilization and exercise in patients with cervicogenic headache: A multi-center randomized clinical trial: BMC Musculoskeletal Disorders, 2016; 17; 64
38.. Racicki S, Gerwin S, DiClaudio S, Conservative physical therapy management for the treatment of cervicogenic headache: A systematic review: J Man Manip Ther, 2013; 21(2); 113-24
39.. Reid SA, Rivett DA, Katekar MG, Callister R, Sustained natural apophyseal glides are an effective treatment for cervicogenic dizziness: J Man Ther, 2008; 13(1); 357-66
40.. Koltyn K, Brellenthin A, Cook D, Mechanisms of exercise-induced hypoalgesia: J Pain, 2014; 15; 1294-304
41.. Chiu I, von Hehn C, Woolf C, Neurogenic inflammation and the peripheral nervous system in host defense and immunopathology: Nat Neurosci, 2012; 15; 1063-67
42.. van Hecke O, Torrance N, Smith B, Chronic pain epidemiology – where do lifestyle factors fit in?: Br J Pain, 2013; 7; 209-17
43.. Prochaska J, Norcross J: Systems of psychotherapy: A transtheoretical analysis; 2019, Boston (MA), Cengage Learning
44.. Hashemzadeh M, Rahimi A, Zare-Farashbandi F, Transtheoretical model of health behavioral change: A systematic review: Iran J Nurs Midwifery Res, 2019; 24; 83-90
45.. Garg R, Joshi S, Mishra S, Bhatnagar S, Evidence based practice pf chronic pain: Indian J Palliat Care, 2012; 18; 155-61
46.. Susan R, Sharby N, Disability reconsidered: the paradox of physical therapy: Phys Ther, 2011; 91; 1715-27
47.. Louw A, Diener I, Butler DS, Puentedura EJ, The effect of neuroscience education on pain, disability, anxiety, and stress in chronic musculoskeletal pain: Arch Phys Med Rehabil, 2011; 92(12); 2041-56
48.. Sillevis R, Cleland J, Hellman M, Beekhuizen K, Immediate effects of a thoracic spine thrust manipulation on the autonomic nervous system: A randomized clinical trial: J Man Manip Ther, 2010; 18(4); 181-90
49.. Ghan GM, Babu VS, Immediate effect of cervico-thoracic mobilization on deep neck flexors strength in individuals with forward head posture: A randomized controlled trial: J Man Manip Ther, 2021; 29(3); 147-57
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133