27 July 2022: Articles 
Hypoprothrombinemia During Cefmetazole Treatment: A Case Report
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Adverse events of drug therapy, Educational Purpose (only if useful for a systematic review or synthesis)
Yuichiro Haba1ABCDEF*, Hikaru Akizuki2ABCDEF, Naoyuki Hashiguchi2ADEF, Toshio NaitoDOI: 10.12659/AJCR.936712
Am J Case Rep 2022; 23:e936712






Abstract
BACKGROUND: Cefmetazole (CMZ), containing an N-methyl-tetrazole-thiol (NMTT) side chain, is a therapeutic option for diverticulitis in Japan. Cephems containing an NMTT, a methyl-thiadiazol, and a thiadiazolethiol side chain are known to induce coagulation disorders.
CASE REPORT: A 76-year-old woman developed hypoprothrombinemia after receiving oral levofloxacin (LVFX) 250 mg q24h for 2 days followed by intravenous CMZ 2 g q8h for sigmoid diverticulitis. On day 5 of CMZ administration (after 12 doses in total), black stool was observed. On the following day (after 14 doses), prothrombin time (PT) prolongation was noted; PT and international normalized ratio (INR) were 37.1 s and 2.47, respectively. We diagnosed the patient with hypoprothrombinemia because of vitamin K deficiency caused by markedly elevated protein levels induced by vitamin K absence or antagonist-II on day 6 of CMZ administration. Intravenous vitamin K administration and CMZ cessation rapidly restored PT and led to the disappearance of black stool.
CONCLUSIONS: The causes of vitamin K deficiency were considered to be an impaired vitamin K cycle due to CMZ and decreased vitamin K intake because of malnutrition. These findings are consistent with CMZ’s reported adverse effects. Decreased vitamin K production due to alterations in the gut bacterial flora by LVFX and CMZ was also postulated as a cause. If a bleeding tendency is noted during diverticulitis treatment with NMTT-containing cephems, switching to intravenous quinolones or carbapenems is recommended. It remains unclear how this reaction can be avoided; however, prudent monitoring of bleeding signs and PT-INR is recommended.
Keywords: Cefmetazole, Hypoprothrombinemias, malnutrition, Vitamin K, Aged, Anti-Bacterial Agents, Blood Coagulation Disorders, diverticulitis, Female, Humans, Vitamin K Deficiency
Background
In Japan, cefmetazole (CMZ) is a good option for the treatment of patients with intra-abdominal infections because it is a cephamycin with activity against a multitude of gram-negative bacteria such as
Case report
A 76-year-old woman with a history of asthma but living in good health accidentally fell and developed a bruise on her right cheek, for which she was brought to the emergency room. On arrival at the hospital, she reported lower left abdominal pain. Furthermore, she had a fever of 38.9°C, blood pressure of 148/82 mmHg, heart rate of 80 beats/min, and respiratory rate of 20 breaths/min. She had no conjunctival anemia, heart murmur, or rales; soft and flat abdomen; normal bowel sounds; spontaneous pain and tenderness in the localized left lower quadrant but no rebound tenderness; and skinned right cheek and right knee. Plain computed tomography revealed inflammation around diverticula in the sigmoid colon (Figure 1). She was administered intravenous acetaminophen 1000 mg and sent home because the diverticulitis was assessed to be less severe and was prescribed oral LVFX 250 mg every 24 h, which was a considering dosage for her renal function. She was instructed to fast; she had already been exhibiting a loss of appetite for 2 weeks. Two days later, the patient revisited the emergency room with a concern of exacerbation of the lower left abdominal pain. She looked weaker and had a body temperature of 37.7°C, blood pressure of 106/60 mmHg, heart rate of 76 beats/min, and respiratory rate of 14 breaths/min. Her body weight and height were 62.6 kg and 144.5 cm, respectively. An examination revealed localized tenderness in the lower left quadrant but no evidence of any peritoneal signs. Oral LVFX was discontinued, and intravenous CMZ was started at a high dose of 2 g every 8 h, despite her renal impairment, for the management of exacerbated diverticulitis. Laboratory findings on the first visit and on admission are shown in Table 1. On day 4 of CMZ administration (the fourth hospital day), she had hypoprothrombinemia; prothrombin time (PT)-international normalized ratio (INR) was prolonged to 1.40. Watery stools were observed only on the fourth hospital day. Even with no use of antithrombotic or non-steroidal anti-inflammatory drugs, muddy black stool was observed on the fifth hospital day (after the 12th administration of CMZ). The patient also had mild stomachache. We started intravenous famotidine 20 mg every 12 h, but did not perform upper endoscopy because the symptom was mild and hemoglobin and blood urea nitrogen levels showed no changes from the time of admission. She was frailer, as evidenced by her weight loss of 1.4 kg. On the sixth hospital day (after the 14th administration of CMZ), her PT and PT-INR further increased to 37.1 s and 2.47, respectively, while her activated partial thromboplastin time (APTT) was 38.5 s (reference range in our hospital: 20.0–38.0 s), but her platelet count was 37.4×104/μL (reference range in our hospital: 15.3–34.6×104/μL) (Table 1, Figure 2). Based on the elevation of PIVKA-II level (27 802 mAU/mL: reference range in our hospital: 0–40 mAU/mL) on day 6 of CMZ administration, a diagnosis of vitamin K deficiency was made. Her renal function on the sixth hospital day did not worsen (Table 1). Therefore, vitamin K 20 mg every 12 h was promptly initiated intravenously, and CMZ was discontinued. On the seventh hospital day, PT-INR recovered to 1.10; furthermore, the black stool spontaneously disappeared. As the fever and abdominal pain subsided, the patient was discharged on the eighth hospital day.
Discussion
In the present case, disseminated intravascular coagulation (DIC) and hepatobiliary disease were considered among the causes of hypoprothrombinemia. DIC was ruled out because there were no changes in platelet count and fibrinogen or D-dimer levels. Hepatobiliary disease was also ruled out because the imaging examinations and hepatobiliary enzyme test showed no abnormalities. As the PIVKA-II level was markedly high, vitamin K deficiency was considered the cause of hypoprothrombinemia; this finding was consistent with that reported previously [8,9]. This assumption was supported by the success of vitamin K replacement therapy. Vitamin K is involved in the activation of coagulation factors II, VII, IX, and X, and causes both PT and APTT prolongation. However, most cases are limited to PT prolongation, as in the present case. This is because the deficiency of factor VII, which has the shortest half-life (3–6 h), precedes it [10]. The factors that cause vitamin K deficiency include the following, with multiple factors often being involved: impaired vitamin K cycle, decreased vitamin K intake, altered gut flora, defective vitamin K absorption due to impaired bile flow or malabsorption syndromes, and chronic kidney diseases [11,12].
Administration of cephems with an NMTT group can cause coagulation disorders associated with an impaired vitamin K cycle, similar to the effects of warfarin [5]. The incidence rate of coagulation disorders associated with CMZ was reported to be 5.7% among patients treated with CMZ for intra-abdominal infections [13]. Chen et al reported that the use of CMZ increased the risk of bleeding events by 2.8-fold, which is a conspicuous increase associated with NMTT-containing cephems, along with a 4.5-fold increase associated with cefoperazone [14]. Although vitamin K deficiency does not easily occur in healthy individuals on a normal diet, it can easily occur in undernourished patients. Fasting affects coagulation factors in some cephem users [15], and bleeding events among users of NMTT-containing cephems increased 1.4-fold under malnutrition conditions compared with those among other antibiotic users [14]. In the present case, the patient had a 21-day fasting period or an insignificant intake and was undernourished, as indicated by the loss of her body weight. Furthermore, her vitamin K stores may have finally been depleted. Coagulation disorders due to LVFX are rare. Mor et al described acquired hemophilia in which factor VIII was reduced by oral LVFX therapy [16]. Our patient was previously treated with oral LVFX; however, APTT prolongation was not observed, suggesting that factor VIII was intact. Gut flora remains an issue [17]. It is not clear whether our administration of broad-spectrum antibiotics, 2-day treatment with LVFX, or 4-day treatment with CMZ disturbed the gut flora because no stool cultures were performed before and after treatment. In short, the causes of hypoprothrombinemia in the present case were an impaired vitamin K cycle and decreased vitamin K intake, with altered gut flora being considered as a potential cause.
Ten cases of CMZ-induced hypoprothrombinemia are accessible on MEDLINE, and they have been summarized in Table 2 [4,8,9,13,18–20]. In these 10 cases, the average patient age was 74.7 (range: 57–93) years and the maximum PT and INR were 87.1 s [18] and 8.3 [19], respectively. The average duration from the start of CMZ treatment to the onset of events was 8.7 (range: 4–20) days. The dominant site of bleeding was the upper gastrointestinal tract, which is similar to a previous report regarding warfarin-associated bleeding [21]. These findings reported previously suggest that CMZ has the ability to cause gastrointestinal bleeding and can enhance the validity of our finding; that is, gastrointestinal bleeding is an adverse effect of CMZ. In our case, the Naranjo scale for adverse drug reaction score [22] was 7 points, indicating that the adverse reaction was probably attributable to CMZ (Table 3).
If a bleeding tendency is noted during the treatment of diver-ticulitis with NMTT-containing cephems and is not completely cured, we recommend switching to the following antibiotics as alternatives: intravenous quinolones such as ciprofloxacin or carbapenems such as imipenem and meropenem [23]. Piperacillin/tazobactam is suitable for diverticulitis management [23]; however, they should be avoided because hypoprothrombinemia has been noted in 6% of individuals who were administered piperacillin/tazobactam [24]. How to avoid this adverse effect in the clinical settings remains controversial. Breen et al recommended 2 approaches: administering prophylactic vitamin K and monitoring PT-INR daily or every other day [19].
Conclusions
Fortunately, bleeding was noticed at an early stage and CMZ administration was stopped in the present case. Although black stool was observed, rapid action, including checking the PTINR, avoided serious bleeding events. Clinicians should recognize coagulation disorders as adverse effects of antibiotics and should carefully monitor bleeding signs and coagulation test results, while distinguishing DIC when administering NMTT-, MTD-, and TDT-containing cephems to frail patients who are likely to have an alteration of the gut flora owing to factors such as malnutrition and past use of broad-spectrum antibiotics.
Figures
References:
1.. Mazuski JE, Sawyer RG, Nathens AB, The Surgical Infection Society guidelines on antimicrobial therapy for intra-abdominal infections: An executive summary: Surg Infect (Larchmt), 2002; 3; 161-73
2.. Haden HT, Vitamin K deficiency associated with prolonged antibiotic administration: AMA Arch Intern Med, 1957; 100; 986-88
3.. Obata H, Iizuka B, Uchida K, Pathogenesis of hypoprothrombinemia induced by antibiotics: J Nutr Sci Vitaminol (Tokyo), 1992(Spec No); 421-24
4.. Shimada K, Matsuda T, Inamatsu T, Urayama K, Bleeding secondary to vitamin K defciency in patients receiving parenteral cephem antibiotics: J Antimicrob Chemother, 1984; 14(Suppl. B); 325-30
5.. Creedon KA, Suttie JW, Effect of N-methyl-thiotetrazole on vitamin K epoxide reductase: Thromb Res, 1986; 44; 147-53
6.. Angles E, Mouton C, Perino J, Hypoprothrombinemia and severe peri-operative haemorrhagic complications in cardiac surgery patients treated with high-dose cefazolin for infective endocarditis: Anaesth Crit Care Pain Med, 2018; 37; 167-70
7.. Yasuoka A, Mukae H, Kinoshita A: Chemother (Tokyo), 1989; 37; 1473-86 [Abstract in English, Text in Japanese]
8.. Nakano E, Fukuoka T, Takeuchi N, A case of alveolar bleeding from clotting abnormality by cefmetazole: Case Rep Med, 2019; 2019; 3574064
9.. Hishikawa H, Tokuhara K, Yoshida T, Yoshioka K, [A case of intraperitoneal bleeding due to vitamin K deficiency after laparoscopic total pelvic exenteration for advanced rectal cancer.]: Gan To Kagaku Ryoho, 2020; 47; 352-54 [Abstract in English, Text in Japanese]
10.. Monroe DM, Roberts HR, Molecular biology and biochemistry of the coagulation factors and pathways of hemostasis, 2010, New York, Williams Hematology
11.. Shirahata A, [9. Vitamin K deficiency in practice. In: Thrombosis and Hemostasis in clinical medicine-practical guidance for residents I.]: Jpn J Thromb Hemost, 2007; 18; 584-87 [Japanese]
12.. Fusaro M, Plebani M, Iervasi G, Gallieni M, Vitamin K Deficiency in chronic kidney disease: Evidence is building up: Am J Nephrol, 2017; 45; 1-3
13.. Holloway WJ, Winslow DL, Reinhardt JG, Cefmetazole treatment of the intra-abdominal infection: J Antimicrob Chemother, 1989(23 Suppl. D); 47-54
14.. Chen LJ, Hsiao FY, Shen LJ, Use of hypoprothrombinemia-inducing cephalosporins and the risk of hemorrhagic events: a nationwide nested case-control study: PLoS One, 2016; 11; e0158407
15.. Moriwaki Y, Sugiyama M, Effect of fasting on coagulation factors in patients who undergo major abdominal surgery: Am Surg, 2010; 76; 168-71
16.. Mor LT, Holley K, A case report of anticoagulation management in acquired hemophilia associated with levofloxacin: J Pharm Pract, 2020; 33; 378-81
17.. Hooper CA, Haney BB, Stone HH, Gastrointestinal bleeding due to vitamin K deficiency in patients on parenteral cefamandole: Lancet, 1980; 1(8158); 39-40
18.. Kijima K, Ozawa K, Sakurai S, [Clinical study of coagulopathy in renal failure. 1. Vitamin K-deficient hemorrhage.]: Nihon Naika Gakkai Zasshi, 1984; 73; 986-94 [in Japanese]
19.. Breen GA, St Peter WL, Hypoprothrombinemia associated with cefmetazole: Ann Pharmacother, 1997; 31; 180-84
20.. Kodama N, Matsumoto S, Matsubayashi S, A suspicious case of cefmetazole-induced hypoprothrombinemia: J Gen Fam Med, 2017; 18; 258-60
21.. Guerrouij M, Uppal CS, Alklabi A, Douketis JD, The clinical impact of bleeding during oral anticoagulant therapy: assessment of morbidity, mortality and post-bleed anticoagulant management: J Thromb Thrombolysis, 2011; 31; 419-23
22.. Wilkins T, Embry K, George R, Diagnosis and management of acute diver-ticulitis: Am Fam Physician, 2013; 87; 612-20
23.. Naranjo CA, Busto U, Sellers EM, A method for estimating the probability of adverse drug reactions: Clin Pharmacol Ther, 1981; 30; 239-45
24.. Gluclu E, Kaya G, Ogutlu A, Karabay O, The effect of cefoperazone sulbactam and piperacillin tazobactam on mortality in gram-negative nosocomial infections: J Chemother, 2020; 32; 118-23
Errate
Figures
Tables
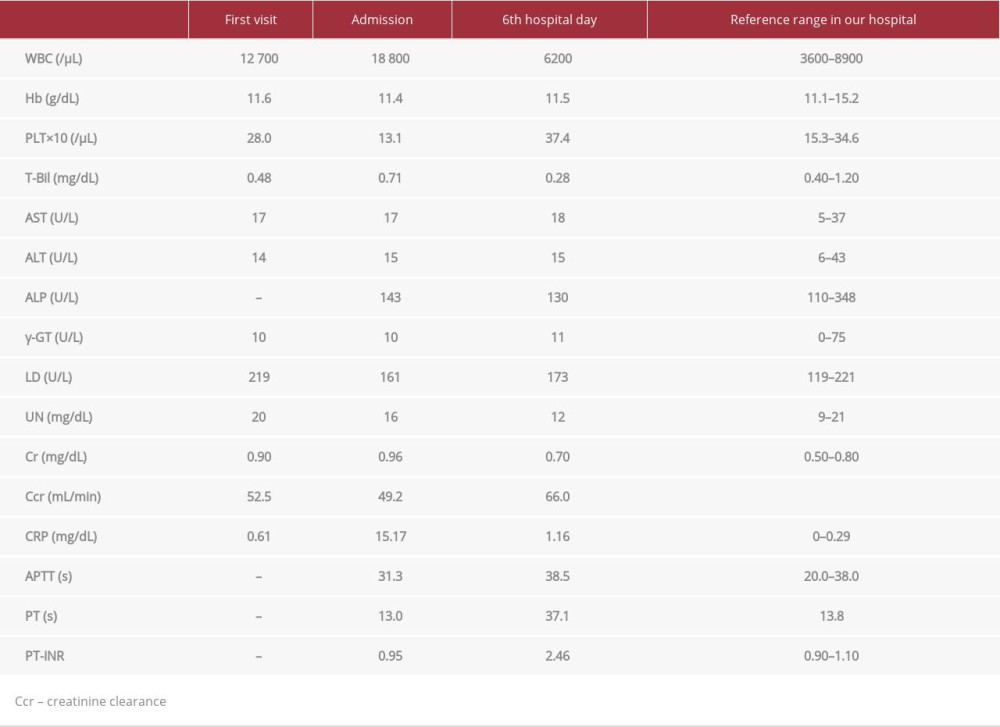 Table 1.. Laboratory findings on the first visit, on admission, and on the 6th hospital day.
Table 1.. Laboratory findings on the first visit, on admission, and on the 6th hospital day.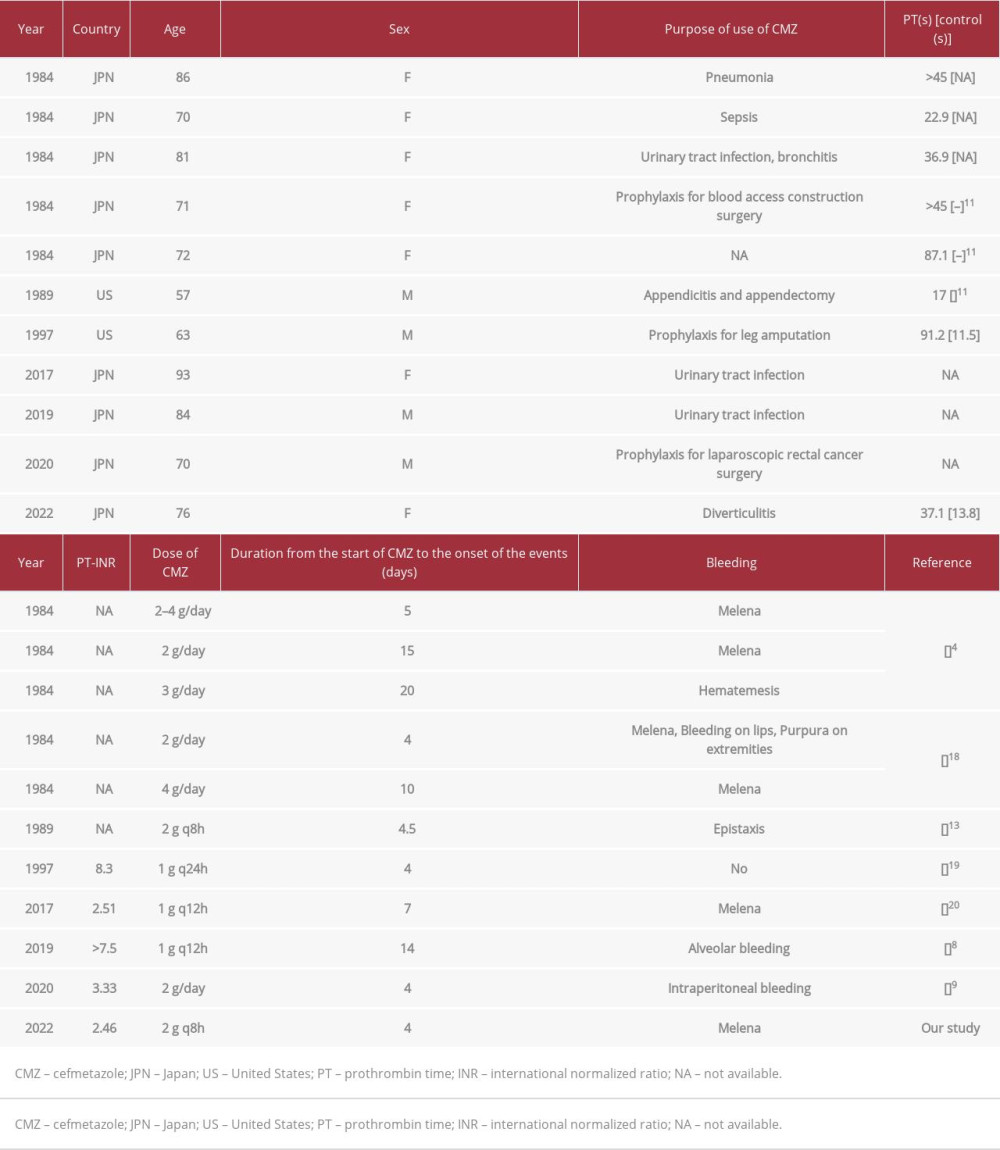 Table 2.. Summary of the previous reported cases of CMZ-induced hypoprothrombinemia on MEDLINE.
Table 2.. Summary of the previous reported cases of CMZ-induced hypoprothrombinemia on MEDLINE.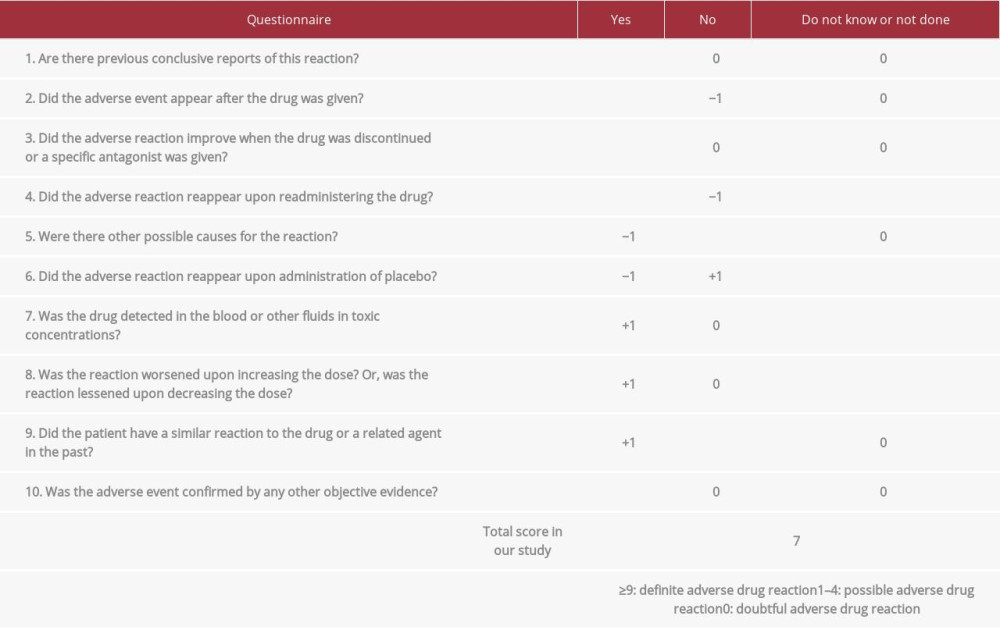 Table 3.. Naranjo scale of adverse drug reaction probability. Underlining is applied for our study.Table 1.. Laboratory findings on the first visit, on admission, and on the 6th hospital day.Table 2.. Summary of the previous reported cases of CMZ-induced hypoprothrombinemia on MEDLINE.Table 3.. Naranjo scale of adverse drug reaction probability. Underlining is applied for our study.
Table 3.. Naranjo scale of adverse drug reaction probability. Underlining is applied for our study.Table 1.. Laboratory findings on the first visit, on admission, and on the 6th hospital day.Table 2.. Summary of the previous reported cases of CMZ-induced hypoprothrombinemia on MEDLINE.Table 3.. Naranjo scale of adverse drug reaction probability. Underlining is applied for our study. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133