04 July 2024: Articles 
Rapid Progression of Acute Interstitial Pneumonia in a Patient with Low MDA-5 Antibody Titer
Unusual clinical course, Challenging differential diagnosis, Unusual setting of medical care
Sung Won ChangDOI: 10.12659/AJCR.943655
Am J Case Rep 2024; 25:e943655






Abstract
BACKGROUND: Melanoma differentiation associated gene-5 antibody (MDA-5 Ab) is one of the diagnostic autoantibodies that appears in idiopathic inflammatory myopathies (IIMs). Unlike when other autoantibodies are positive, when this antibody is positive, there is less characteristic muscle involvement. However, this MDA-5 Ab-positive myopathy presents extremely rapid progression of interstitial lung disease, resulting in a high mortality rate. Previous studies reported that the prognosis of this lung disease will be determined by the titer and suggest that low titers of MDA-5 antibody can indicate a good prognosis in associated interstitial lung disease.
CASE REPORT: Our case describes a 55-year-old woman who presented with acute respiratory symptoms and dyspnea. After hospitalization, symptoms and chest imaging worsened rapidly, and the radiology image of lung disease featured interstitial changes not seen in typical infections. We treated the patient with a high-flow oxygen nasal cannula, empirical antibiotics, and a systemic steroid. While treatment for a disease of unknown cause was continued, low titer of MDA-5 antibody was identified.
CONCLUSIONS: This case suggests 2 points to consider about non-infectious interstitial changes with acute respiratory distress syndrome. First, when treating rapidly progressing interstitial pneumonia of an unknown cause, it is recommended to consider lung involvement of MDA-5 Ab dermatomyositis. Second, a low titer of MDA-5 Ab can be associated with better prognosis in this MDA-5 Ab dermatomyositis-related lung disease.
Keywords: Lung Diseases, Interstitial, MDA5 protein,zebrafish, Female, Humans, Middle Aged, Acute Disease, Autoantibodies, Disease Progression, Interferon-Induced Helicase, IFIH1
Introduction
Idiopathic inflammatory myopathies (IIMs) are autoimmune disorders distinguished by muscle inflammation and involvement of various extra-muscular organ systems. In IIMs, lung involvement is frequently identified, mainly in the form of interstitial lung disease (ILD), with a rate ranging from 17% to 36%. The frequency and clinical manifestations of lung involvement varies depending on the autoantibodies. For examples, anti-Jo1 and anti-PL7, the autoantibodies known to frequently accompany lung involvement, occur in 66% and 84% of IIMs, respectively [1].
Melanoma differentiation associated gene-5 antibody (MDA-5 Ab) is also an autoantibody that frequently accompanies lung involvement and is identified in approximately 10% of IIMs in adults. Unlike in other antibody-positive cases, MDA-5 Ab muscle involvement is seen only in less than 20% of cases and shows aspects of amyopathic IIMs. This antibody also shows lung involvement in adult myositis, and lung involvement in this case is more common in Asian populations (60% in Europeans and 90% in Asians) [1–4].
The manifestation of lung involvement in MDA-5 Ab is also different from that seen with other autoantibodies. The predominant chest computed tomography (CT) finding is organizing pneumonia, followed by nonspecific interstitial pneumonia. About half of cases show rapid-progress ILD, which progresses to interstitial pneumonia within several weeks to months [4]. Empirically, MDA-5 Ab-positive interstitial pneumonia is treated like other connective tissue disease ILDs. However, to date, there are not sufficient evidences for additional management and treatment in MDA-5 Ab-positive rapid-progress ILD, and the mortality rate related to ILD is high.
Here, we report a 55 year-old female patient who presented with interstitial pneumonia of unknown etiology. A relatively low titer of MDA-5 antibody was confirmed during empirical antibiotic and immunosuppressive treatment, and this patient had a good prognosis, with full recovery without sequelae.
Case Report
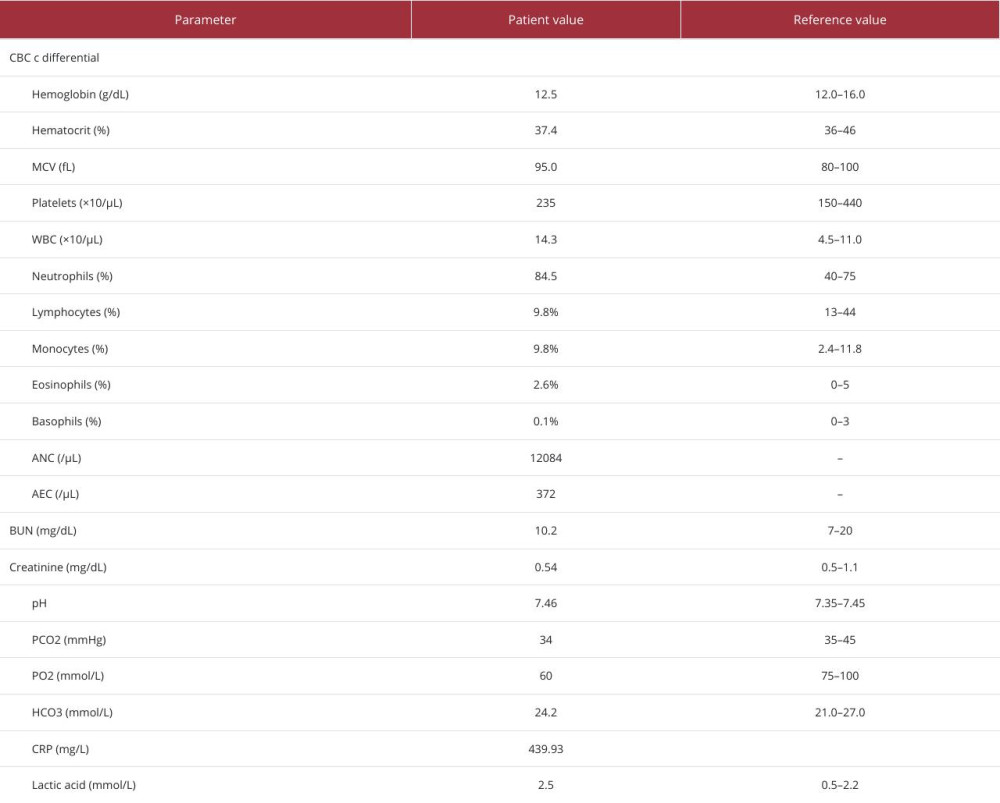
A 55-year-old female patient with a past history of diabetes mellitus, hypothyroidism after left thyroidectomy due to diagnosis of suspicious thyroid nodule, and post-menopausal osteopenia visited our Emergency Department (ED) for a sputum-producing cough that started a week prior and dyspnea that started the previous day. The patient’s initial vital signs showed tachycardia and low oxygen saturation in room air. Initial measurements were blood pressure, 110/70 mmHg (mean arterial pressure: 83 mmHg); body temperature, 37.2°C; respiratory rate, 21 breaths/min; heart rate, 106 beats/min; and oxygen saturation in room air, 93%. There were no specific findings in the nervous system, skin, muscle, or joints. Initial chest radiography revealed bilateral diffuse haziness, predominantly in the lower lung field. In laboratory findings, leukocytes were elevated, at 14.3×103/μL, with neutrophil dominance of 84.5%, and C-reactive protein level was elevated, at 364.56 mg/L (Table 1). Chest CT revealed multifocal ground-glass opacities (GGOs) and consolidations in both lungs, mainly in the lower lobes (Figures 1, 2).
Based on findings in the ED, it was thought to be pneumonia, and the patient was admitted to a general ward because her oxygen requirement was not high. However, on day 1 of hospitalization, pneumonia progressed rapidly, and the PaO2/ FiO2 ratio worsened to under 150 mmHg, such that a high-flow nasal cannula was needed. Shock was also confirmed. Vital signs were blood pressure, 90/55 mmHg (mean arterial pressure: 67 mmHg); body temperature, 38.2°C; respiratory rate, 28 breaths/min; and heart rate, 110 beats/min.
Suspecting acute respiratory distress syndrome (ARDS) with severe pneumonia, we transferred her to the Intensive Care Unit (ICU) and initiated antibiotics (ceftriaxone and levofloxacin) and systemic steroid therapy (initial dose: methylprednisolone 1 mg/kg). We performed bronchoscopy, and there were no specific endoscopic lesions. Because of hypoxemia, bronchial alveolar lavage could not be performed, and only bronchial washing was performed to obtain a specimen. Therefore, an appropriate sample capable of analyzing the white blood cell differential count could be obtained. In the specimen obtained through bronchial washing, the Gram stain and culture was negative; however,
In a multidisciplinary discussion with the Radiology Department, it was considered necessary to perform a workup for causes other than infection because of the initial chest CT finding of lower lobe dominant GGOs and consolidations with traction bronchiectasis in both basal lobes. Therefore, we conducted an additional workup, including serology.
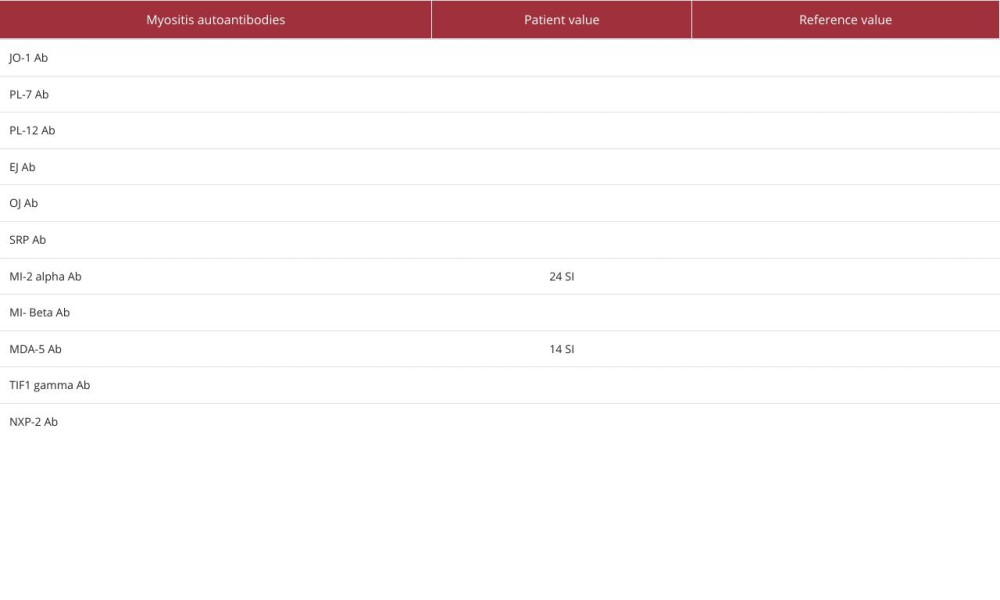
After 10 days of ICU treatment, the oxygen supply was reduced to a PaO2/FiO2 ratio above 300, and we transferred the patient to the general ward. During treatment with steroids and antibiotics, MDA-5 (14 SI) and Mi-2a (24 SI) antibodies were detected (Table 2). We performed follow-up chest CT to confirm the changes in progress. Compared with the initial chest CT, there were increased GGOs in both upper lobes. In the bilateral lower lobes, there were decreased GGOs and consolidations; however, there was new multifocal fibrosis and air trapping (Figure 3).
We stopped using antibiotics but continued steroid treatment while the patient was in the general ward, owing to high suspicious of interstitial pneumonia with autoimmune features and radiological findings suggestive of acute interstitial pneumonia. We gradually reduced the steroid dose to prednisolone 12.5 mg. At the time of discharge, her oxygen requirement and other vital signs were normal: blood pressure, 130/80 mmHg (mean arterial pressure: 97 mmHg); body temperature, 36.8°C; respiratory rate, 18 breaths/min; heart rate, 85 beats/min; and oxygen saturation in room air, 98%. She was discharged with administration of oral steroids. In 3 months of outpatient follow-up, she continued steroid therapy, while we carefully observed symptoms and radiologic findings. She showed no new skin, muscle, and joint involvement; therefore, we did not add treatment other than steroids, in consultation with the Rheumatology Department. On chest X-ray after 2 months of steroid therapy, the diffuse haziness was markedly decreased, and on chest CTs, bilateral diffuse GGOs and consolidations were decreased (Figure 4). At the 6-month follow-up, respiratory symptoms also recovered almost fully, and chest CT showed a more recovered status, with improvement of previous air trapping (Figure 5).
Discussion
We reported interstitial pneumonia with ARDS, with a low MDA-5 titer. In this case, the patient had no noticeable findings other than respiratory symptoms. Therefore, we did not consider autoimmune antibodies, including IIMs, as a cause of ARDS from the beginning. In addition to the MDA-5 Ab-positive finding,
MDA-5 Ab is known to have a lower prevalence of muscle involvement, compared with other myositis autoantibodies [7]. Similar to our case, there are reports of patients progressing to ARDS, with insufficient evidence of myositis. In the case of previous reports, myositis could not be suspected at first, because the patients did not show any extra pulmonary symptoms other than joint pain [8,9]. Even in our report, there were no signs of suspected myositis other than respiratory symptoms. Therefore, in pneumonia with rapid exacerbation of hypoxia of unknown cause, anti-MDA5 should be considered.
The current therapy is an empirical immunosuppressive agent consisting of corticosteroids, calcineurin inhibitors, and cyclophosphamide in MDA-5 Ab-positive ILD [10]. Fortunately, our patient had a good response of interstitial pneumonia with only corticosteroid treatment, and no respiratory sequelae were observed. A previous study reported that a low positive titer of the MDA-5 antibody indicated a good prognosis in patients with MDA-5 Ab-positive ILD, and the suggested cutoff value was 100 SI [11,12]. In our case, the titer of MDA-5 Ab was as low as 14 SI, which may be related to the treatment response. Therefore, not only the presence of antibodies but also the confirmation of the titer of antibodies are thought to be important in lung disease.
Conclusions
In ARDS, in which radiologic imaging shows interstitial damage of unclear cause, the presence of MDA-5 antibodies should be considered. In addition, as the prognosis can vary depending on the titer of MDA-5, it is necessary to check the antibody titer if atypical pulmonary invasion with rapid progressive hypoxemia is identified. Furthermore, observation of the interstitial lung damage by follow-up MDA-5 antibody testing will be necessary.
Figures
References:
1.. Lega JC, Reynaud Q, Belot A, Idiopathic inflammatory myopathies and the lung: Eur Respir Rev Jun, 2015; 24(136); 216-38 [Erratum in: Eur Respir Rev. 2015;24(137)545]
2.. Ceribelli A, Fredi M, Taraborelli M, Prevalence and clinical significance of anti-MDA5 antibodies in European patients with polymyositis/dermatomyositis: Clin Exp Rheumatol, 2014; 32(6); 891-97
3.. So H, Ip RW, Wong VT, Yip RM, Analysis of anti-melanoma differentiation-associated gene 5 antibody in Hong Kong Chinese patients with idiopathic inflammatory myopathies: Diagnostic utility and clinical correlations: Int J Rheum Dis, 2018; 21(5); 1076-81
4.. Chen X, Jiang W, Jin Q, Clinical, radiological and pathological features of anti-MDA5 antibody-associated interstitial lung disease: RMD Open, 2023; 9(2); e003150
5.. Anderle K, Machold K, Kiener HP, COVID-19 as a putative trigger of anti-MDA5-associated dermatomyositis with acute respiratory distress syndrome (ARDS) requiring lung transplantation, a case report: BMC Rheumatol, 2022; 6(1); 42
6.. Hoey J, Solomon JL, Kim B: J Med Case Rep, 2022; 16; 401
7.. Kurtzman DJB, Vleugels RA, Anti-melanoma differentiation-associated gene 5 (MDA5) dermatomyositis: A concise review with an emphasis on distinctive clinical features: J Am Acad Dermatol, 2018; 78(4); 776-85
8.. Aissaoui H, Alsibai KD, Khayath N, Fast-onset diffuse interstitial lung disease in anti-MDA5 antibodies-associated amyopathic dermatomyositis: Clin Pract, 2021; 11(2); 235-40
10.. McPherson M, Economidou S, Liampas A, Management of MDA-5 antibody positive clinically amyopathic dermatomyositis associated interstitial lung disease: A systematic review: Semin Arthritis Rheum, 2022; 53; 151959
11.. Matsushita T, Mizumaki K, Kano M, Antimelanoma differentiation-associated protein 5 antibody level is a novel tool for monitoring disease activity in rapidly progressive interstitial lung disease with dermatomyositis: Br J Dermatol, 2017; 176(2); 395-402
12.. Sakamoto S, Okamoto M, Kaieda S, Low positive titer of anti-melanoma differentiation-associated gene 5 antibody is not associated with a poor long-term outcome of interstitial lung disease in patients with dermatomyositis: Respir Investig, 2018; 56(6); 464-72
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133