17 July 2024: Articles 
Incidental Diagnosis of Malignant Peritoneal Mesothelioma During Liver Transplantation Surgery: A Case Report
Challenging differential diagnosis, Unusual setting of medical care, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Spogmai Khan1E, Adnan Malik2E, Shahbaz Qureshi2E, Babak Cohen3E, Abdul Nadir2EF*DOI: 10.12659/AJCR.943787
Am J Case Rep 2024; 25:e943787






Abstract
BACKGROUND: Malignant peritoneal mesothelioma (MPM) is a rare, lethal tumor of serous membranes. The most common factor reported in association with MPM is asbestos exposure, while viral infections, genetic predisposition, paraneoplastic syndrome, and altered immunity have been described as well. The diagnosis can be challenging among those with lower tumor burden as well as nonspecific symptoms, and it is not unusual to discover the diagnosis incidentally.
CASE REPORT: A middle-aged woman with decompensated cirrhosis underwent extensive pre-transplant workup, showing no evidence of malignancy. She had a personal history of asbestos exposure and family history of MPM in the extended family. During transplant surgery, a few peritoneal nodules were noted, leading to termination of the procedure. Pathological analysis confirmed malignant MPM. A multidisciplinary discussion led to following a conservative treatment approach without any intervention, due to higher risk of worsening hepatic decompensation associated with peritonectomy and intraperitoneal chemotherapy. The patient’s hepatic decompensation resolved 6 months after the aborted liver transplant operation. Since the diagnosis of MPM, positron emission tomography scans have shown no recurrence of MPM for 3 consecutive years.
CONCLUSIONS: This is the first case of MPM diagnosed incidentally during a liver transplantation surgery. This case highlights the challenges in the diagnosis and management of MPM in a patient with decompensated liver disease. A multidisciplinary approach and following a consensus decision led to prolonged survival in the described patient.
Keywords: Incidental Findings, Liver Cirrhosis, Mesothelioma, Malignant, Humans, Liver Transplantation, Female, Peritoneal Neoplasms, Middle Aged, Mesothelioma, Malignant, Mesothelioma, lung neoplasms
Introduction
Malignant peritoneal mesothelioma (MPM) is an aggressive connective tissue tumor that arises from the peritoneum. MPM constitutes 10% to 15% of all new mesothelioma cases reported annually in the United States [1]. It predominantly affects male patients aged 50 to 69 years [2,3]. Asbestos, industrial mineral fiber, thorotrast, familial Mediterranean fever, simian virus 40, diffuse lymphocytic lymphoma, and BAP1 mutation are reported causal associations of MPM [2]. MPM is a clinical conundrum of nonspecific presentation, incidental diagnosis, and poor prognosis. We describe a case of MPM diagnosed during an aborted liver transplant operation, to inform our readers of the outcome of MPM in a patient with decompensated liver disease. A conservative approach based on the recommendation of the multidisciplinary team involved in the decision-making process has led to prolonged survival.
Case Report
A 44-year-old woman presented to the clinic with a 2-week history of tense ascites, jaundice, episodic confusion, and lethargy. Four weeks prior to her presentation, she had been prescribed ketoconazole for a positive coccidioidomycosis serology, which was obtained prior to starting her on a new immunosuppressive agent for plaque psoriasis. She had been previously treated with secukinumab, adalimumab, and methotrexate for plaque psoriasis, with moderate symptom control. She had a history of metabolic dysfunction associated with steatohepatitis cirrhosis, documented with a liver biopsy 10 years earlier. She had a family history of MPM and renal cell cancer. The patient’s maternal cousin received a diagnosis of MPM at the age of 70 years and was undergoing treatment. She reported that her college dormitories were found to have high asbestos levels in the walls.
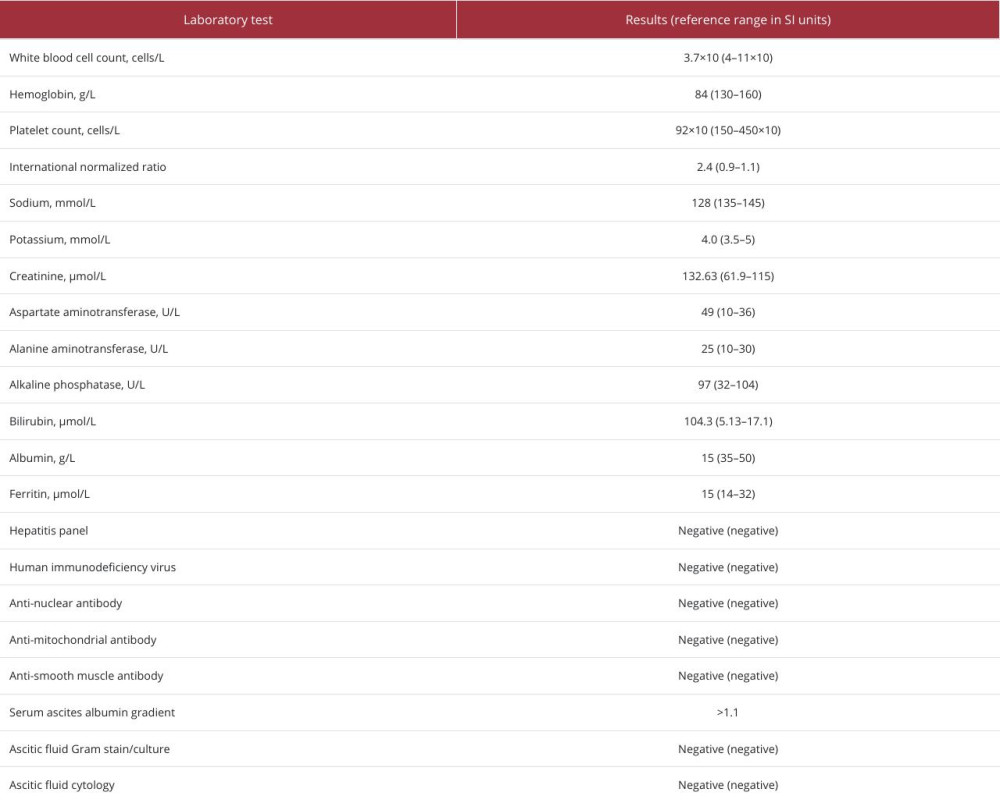
She had a height of 162.5, weight of 116.7 kg, and body mass index of 44.1. Scleral icterus, reduced breath sounds in the left lung field posteriorly, moderate ascites, and psoriatic patches on the extensor surfaces of the skin were documented on physical examination. A complete blood count, comprehensive metabolic panel, hepatitis serologies, autoantibodies, and ascitic fluid analysis are summarized in Table 1. Her model for end-stage liver disease-sodium on initial presentation was 31. An abdominal computed tomography (CT) scan with contrast showed cirrhosis, mild splenomegaly, left-sided pleural effusion, and ascites. Her clinical presentation was consistent with decompensation of the underlying cirrhosis, most likely due to ketoconazole hepato-toxicity. All medications were discontinued, and a liver transplant referral was initiated. Low-salt diet and diuretics were started for the management of fluid overload, and lactulose was started for hepatic encephalopathy.
She underwent a pre-transplant workup, including a CT scan of the abdomen with contrast 2 months before the liver transplant operation, showing cirrhosis, splenomegaly, and no evidence of tumor. Five months after the patient’s initial presentation, a liver transplant was attempted but aborted when several peritoneal nodules (the largest measuring <0.5 cm) were found under the right diaphragm (Figure 1). Biopsy of the nodules was diagnostic for MPM of the epithelioid subtype. Immunohistochemistry showed cytokeratin 7+, calretinin+, WT1+, and p53 reactivity, with loss of nuclear staining in the cancerous epithelioid cells (BAP1) (Figures 2, 3). The peritoneal cancer index was 1 for our patient, representing a very low tumor load.
A multidisciplinary discussion with medicine, surgery, and oncology departments did not recommend aggressive interventions, such as intraperitoneal chemotherapy and peritoneal stripping, due to the potential risk of hepatic decompensation and increased mortality. Three years later, after the aborted liver transplantation, her liver disease had compensated spontaneously. She was prescribed supportive medicines, including furosemide 40 mg, spironolactone 100 mg, lactulose titrated to having 3 bowel movements daily, multivitamins, calcium, and vitamin D supplements daily. To date, 4 positron emission tomography (PET) scans have documented no abnormal up-take of glucose in the peritoneum.
Discussion
This unique case highlights an unusual presentation of MPM, diagnosed incidentally during a liver transplant attempt for hepatic decompensation, and a 3-year survival without any documented recurrence on traditional imaging. Historically, MPM is reported to have a very short symptom-to-survival time, with a median survival time of approximately 6 to 12 months [4]. Long-term survival with MPM has been reported in several cases, the longest being 19 years but after aggressive chemotherapy was used [5]. Three histological subtypes of MPM including epithelioid, sarcomatoid, and biphasic have been reported. Epithelioid MPM is considered less aggressive, with favorable outcomes due to milder cellular atypia, lower mitotic activity, smaller tumor size, and low proliferating cell nuclear antigen (Ki67) [6]. Women have better prognosis due to the higher incidence of the epithelioid subtype and protective role of circulating estrogens and estrogen receptor-beta expression [7]. Early-stage malignancy, with low a peritoneal cancer index of 1 on Gilly classification and smaller lesion size (<0.5 cm), also followed an indolent course and better prognosis [8].
MPM is typically diagnosed incidentally on abdominal imaging or during a surgical procedure [9]. The clinical presentation is non-specific. Abdominal pain/distension, intestinal obstruction, ascites, fever, diarrhea, vomiting, weight loss, hernia formation, and paraneoplastic syndromes, consisting of thrombocytopenia, thrombosis, hemolytic anemia, and nephrotic syndrome, have all been described [8]. A family history of germline mutation of BAP1 (a tumor suppressor gene), uveal melanoma, clear cell renal carcinoma, and cholangiocarcinoma has been associated with MPM [10,11].
Despite extensive pre-transplant evaluation, the diagnosis of MPM did not surface on any imaging studies, leading to an incidental diagnosis during the aborted liver transplant attempt. Standard abdominal imaging can reveal peritoneal thickening, but ascites can preclude the visualization [10]. Our patient is undergoing fluorine-18 fluorodeoxyglucose PET (FDGPET) every 6 months, last performed in October 2023, showing no evidence of the recurrence of MPM. FDG-PET/contrast-enhanced CT are reported to be 86% sensitive and 89% specific for MPM [6,12]. However, it is reported that approximately 12% of falsely negative FDG-PET in mesothelioma are associated with epithelioid histology and early cancer stage [13].
Peritonectomy (cytoreductive surgery) with hyperthermic intraperitoneal chemotherapy is the standard of care for MPM. Chemotherapeutic agents, including cisplatin, doxorubicin, and paclitaxel, are preferred [1,2]. Angiokinase inhibitors, such as nintedanib, and humanized anti- vegetative endothelial growth factor (VEGF) antibodies, such as bevacizumab, have improved progression-free survival and overall survival [9,14]. Trials with CTLA-4 inhibitor including tremelimumab and darvalumab have showed promising results as well [15,16].
Owing to multiple comorbidities and the risk of hepatic decompensation, our patient’s treatment consisted of close follow-up in the outpatient clinic, where complications of portal hypertension were managed with supportive medicine, deemed most suitable for her. MPM is a rare tumor, reported to have chronic insidious course in rare instances. The decision to choose an observational approach was based on the basic principle of primum non nocere (first do no harm), as any aggressive therapy could have possibly led to poor outcome, particularly with underlying cirrhosis.
Looking with a retrospective lens, she had prior asbestos exposure and a family history of mesothelioma, highlighting that detailed history remains the most important kit in the toolbox of a physician, even though it is unlikely that the diagnosis could have been concluded prior to the liver transplant surgery.
Conclusions
This case reports an unusual presentation of a rare disease. Ultimately, our patient has done well over a period of 3 years since the diagnosis of MPM, in the background of decompensated liver disease. Multidisciplinary input, close clinical follow-up, and keeping up the hopes to beat the odds have given her 3-year survival since her diagnosis, emphasizing that sometimes careful observation can accomplish better results than aggressive therapies, with their inherent complications, which could possibly result in early mortality. A balanced team effort, devised by healthcare providers, remains the best approach in planning care for any patient, particularly for those who have rare diseases and unusual presentations. This is a unique case of MPM with an insidious course found incidentally during liver transplant surgery. Being a single occurrence, this anecdotal case report should not be generalized to the overall care of MPM.
Figures
References:
1.. Kim J, Bhagwandin S, Labow DM, Malignant peritoneal mesothelioma: A review: Ann Transl Med, 2017; 5; 236
2.. Helm JH, Miura JT, Glenn JA, Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: A systematic review and meta-analysis: Ann Surg Oncol, 2015; 22; 1686-93
3.. Zhai Z, Ruan J, Zheng Y, Assessment of global trends in the diagnosis of mesothelioma from 1990 to 2017: JAMA Netw Open, 2021; 4; e2120360
4.. Mollaoğlu MC, Karabacak U, Bostancı ME, Is extereme cytoreductive surgery beneficial to survival ın malignant peritoneal mesothelioma?: Acta Chir Belg, 2024 [Online ahead of print]
5.. de Boer NL, van Kooten JP, Damhuis RAM, Malignant peritoneal mesothelioma: patterns of care and survival in the Netherlands: A population-based study: Ann Surg Oncol, 2019; 26; 4222-28
6.. Karpes JB, Shamavonian R, Dewhurst S, Malignant peritoneal mesothelioma: An in-depth and up-to-date review of pathogenesis, diagnosis, management and future directions: Cancers (Basel), 2023; 15; 4704
7.. Van Gerwen M, Alpert N, Wolf A, Prognostic factors of survival in patients with malignant pleural mesothelioma: An analysis of the National Cancer Database: Carcinogenesis, 2019; 40; 529-36
8.. Sun L, Li C, Gao S, Diffuse malignant peritoneal mesothelioma: A review: Front Surg, 2023; 9; 1015884
9.. Broeckx G, Pauwels P, Malignant peritoneal mesothelioma: A review: Transl Lung Cancer Res, 2018; 7; 537-42
10.. Testa JR, Cheung M, Pei J, Germline BAP1 mutations predispose to malignant mesothelioma: Nat Genet, 2011; 43; 1022-25
11.. Pena-Llopis S, Vega-Rubin-de-Celis S, Liao A, BAP1 loss defines a new class of renal cell carcinoma: Nat Genet, 2012; 44; 751-59
12.. Dubreuil J, Giammarile F, Rousset P, The role of 18F-FDG-PET/ceCT in peritoneal mesothelioma: Nucl Med Commun, 2017; 38; 312-18
13.. Ma J, Zhang S, Prognostic factors of malignant peritoneal mesothelioma: A retrospective study of 52 female patients: World J Surg Oncol, 2022; 20; 219
14.. Disselhorst MJ, Quispel-Janssen J, Lalezari F, Ipilimumab and nivolumab in the treatment of recurrent malignant pleural mesothelioma (INITIATE): Results of a prospective, single-arm, phase 2 trial: Lancet Respir Med, 2019; 7; 260-70
15.. Sugarbaker PH, Acherman YI, Gonzalez-Moreno S, Diagnosis and treatment of peritoneal mesothelioma: The Washington Cancer Institute experience: Semin Oncol, 2002; 29; 51-61
16.. Gregory SN, Sarvestani AL, Blakely AM, Malignant peritoneal mesothelioma literature review: past, present, and future: Dig Med Res, 2022; 5; 29
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133