02 August 2024: Articles 
Voriconazole-Induced Periostitis: A Mimicker of Skeletal Coccidioidomycosis
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Adverse events of drug therapy, Educational Purpose (only if useful for a systematic review or synthesis)
Priyal J. ShahDOI: 10.12659/AJCR.944102
Am J Case Rep 2024; 25:e944102






Abstract
BACKGROUND: Coccidioidomycosis is caused by the fungi Coccidioides immitis and Coccidioides posadasii, which are endemic to the southwestern United States and other countries of the Western Hemisphere. Pulmonary coccidioidomycosis is the most common form of coccidioidomycosis. Rarely, coccidioidal infection disseminates to meninges, bones, skin, and soft tissues. While fluconazole remains the first line of treatment and is used for most patients, voriconazole is used in selected refractory cases of coccidioidomycosis. Voriconazole has more fluorine molecules than other azoles, and over time the fluorine molecules in voriconazole can cause disorganized bone formation in the periosteal region (periostitis), causing generalized bony pain, and radiographically can mimic skeletal coccidioidomycosis. While voriconazole-induced periostitis has been noted in aspergillosis and other infections, it has not been reported commonly in patients with coccidioidomycosis.
CASE REPORT: We present a case of a 50-year-old female patient with a diagnosis coccidioidal meningitis who was refractory to fluconazole and was treated with voriconazole. She presented with bony pain, which was initially radiographically attributed to multifocal skeletal coccidioidal infection. Reflecting upon the patient’s history and serum levels of fluoride and bone alkaline phosphatase, a diagnosis of voriconazole-induced periostitis was made. Discontinuation of the voriconazole resulted in resolution of the periostitis.
CONCLUSIONS: Voriconazole-induced periostitis should be considered in patients with musculoskeletal pain with a history of voriconazole treatment or with laboratory abnormalities, such as elevated fluoride levels and/or bone alkaline phosphatase. Discontinuation of voriconazole reverses the condition promptly.
Keywords: Coccidioidomycosis, Periostitis, voriconazole, Humans, Middle Aged, Female, Antifungal Agents, Diagnosis, Differential
Introduction
Coccidioidomycosis is a common endemic fungal infection in the southwest United States, and primary pulmonary coccidioidomycosis is the most common presentation of coccidioidal infections [1]. In addition to pulmonary and systemic symptoms, musculoskeletal pain due to arthralgias and myalgias is common in patients with primary pulmonary coccidioidomycosis [2]. The first-line treatment for coccidioidal infections (including meningitis) is fluconazole [3]. In patients with coccidioidomycosis, voriconazole can be a therapeutic option when patients cannot tolerate first-line treatments or first-line treatments fail [4].
Voriconazole-induced periostitis was first reported in 2009 in 5 lung transplant patients who were treated with voriconazole for long-term prophylaxis. Diffuse extremity pain with elevated alkaline phosphatase levels was reported, without an alternate explanation [5]. The fluorine molecules in voriconazole stimulate osteoblasts, which initiate disorganized bone development in periosteal regions, causing inflammation of the periosteum (periostitis) [6]. Such skeletal periostitis is not a rare condition; we are aware of 90 cases in the literature reported in various formats [6,7]. However, this periostitis can have delayed recognition due to other conditions with similar clinical presentations, such as hypertrophic osteoarthropathy, venous stasis, thyroid acropachy, and hypervitaminosis [8]. We present a case of voriconazole-induced periostitis that was initially radiographically attributed to multifocal skeletal coccidioidal infection.
Case Report
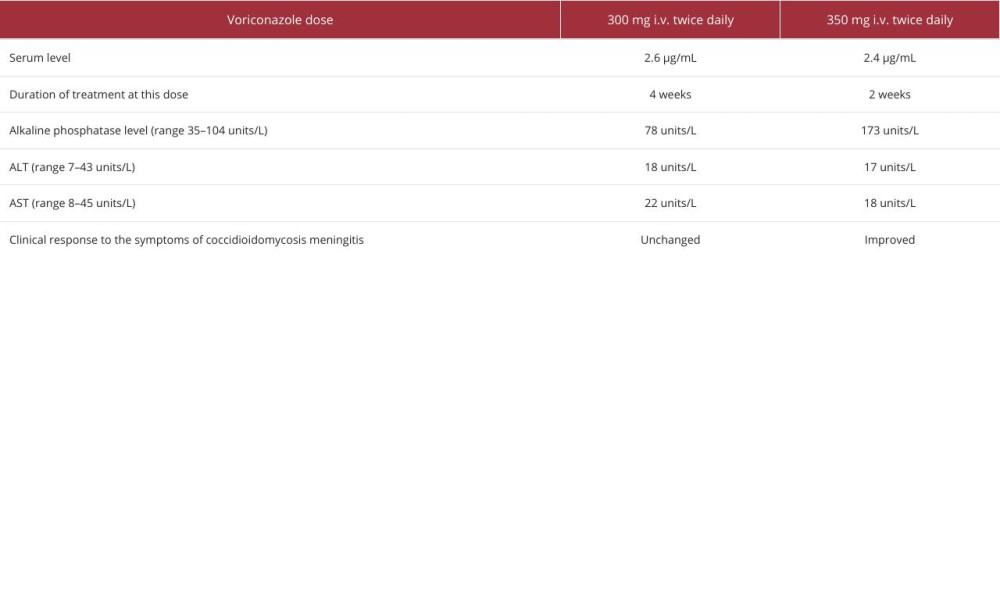
A 50-year-old female patient had a weight of 62 kg and a past medical history of hypertension, gastric band surgery for morbid obesity, several motor vehicle accidents requiring extensive rehabilitation, and multiple knee surgeries requiring multiple steroid injections for pain. She was in her usual health, until she presented for medical attention with headaches, protracted nausea, and vomiting and received a diagnosis of coccidioidal meningitis, after multiple hospital admissions. She was treated with oral fluconazole 800 mg daily (12.9 mg/kg). After several months, she developed generalized body aches, prompting a nuclear bone scan, which was consistent with degenerative changes (Figure 1). She also developed fluconazole-related hair loss and cheilitis. She was switched to posaconazole 400 mg daily. Although her serology results temporally improved with posaconazole, her subsequent clinical course was notable for biochemical progression of meningitis, increasing leptomeningeal enhancement at C6-C7, and cerebellar infarction. She was then switched to intravenous voriconazole 300 mg twice daily (4.8 mg/kg twice daily) with intravenous liposomal amphotericin, with documentation of a therapeutic voriconazole trough of 2.6 µg/mL (reference range 1.0–5.5). Her alkaline phosphatase level rose from 78 to 173 units/L (reference range 35–104). Despite these treatments, magnetic resonance imaging (MRI) of the spine suggested that the infection progressed to spinal myelitis, involving the central cord at T1-T3. In light of the progressing MRI and a decreased cerebrospinal fluid glucose level, her voriconazole was cautiously increased to 350 mL intravenously (5.6 mg/kg) twice daily, with a resulting voriconazole trough level of 2.4 µg/mL. Liposomal amphotericin was continued at thrice weekly dosing for 6 weeks, then stopped. Table 1 shows changes in clinical and laboratory parameters with the changes in voriconazole dose. She slowly began to clinically improve. Within a month after initiating the voriconazole-liposomal amphotericin regimen, she was admitted to the hospital for chest pain, which was diagnosed as movement-associated rib pain. At that time, she also reported rapidly progressive severe pain in the back, neck, bilateral shoulders, arms, and hand; all pain was rated at 9/10 on a pain scale, which responded transiently to hydrocodone. A technetium-99 nuclear medicine bone scan showed multi-focal skeletal lesions (Figure 2). The initial radiology report identified these abnormalities to be consistent with multi-focal skeletal (disseminated) coccidioidomycosis, but after a careful review of her history, a suspicion for voriconazole-associated periostitis was raised (Figure 2). Her serum fluoride level was 12.1 μmol/L (upper limit of 3.0 μmol/L), and the alkaline phosphatase level was 296 units/L. Within 20 days of stopping the voriconazole, the alkaline phosphatase blood level had improved to 185 units/L, and subsequently normalized. Voriconazole was stopped and replaced with isavuconazonium 372 mg daily. At a follow-up visit 8 days after change of medication, her pain had entirely resolved. A bone scan 4 months after voriconazole withdrawal showed resolving boney abnormalities (Figure 3). After a few years, she had clinical and biochemical remission of her infection. At the time of this report, she remains on isavuconazonium 372 mg daily indefinitely.
Discussion
Certain triazoles, such as fluconazole, posaconazole, and voriconazole, have fluoride molecules that are integral components of their molecular structure [6]. Itraconazole has no fluoride molecule, whereas voriconazole has one extra fluoride molecule. With triazole treatment, the fluoride molecule can dissociate from the azole structure and can incorporate into the bony matrix as fluorapatite, which causes a disorganized osteoblastic reaction, manifested as skeletal fluorosis, a condition characterized by periosteal thickening, exostosis, and osteosclerosis [6]. Symptomatic patients experience generalized bone pain, bone brittleness, exostosis, higher total serum and bony alkaline phosphatase levels, and elevated plasma fluoride levels. The periosteal reaction is focal, nodular, dense, and irregular [9,10]. The clinical presentation can potentially mimic skeletal coccidioidomycosis.
Skeletal coccidioidomycosis can also show as multiple and symmetrical, with a predilection for boney prominences and metaphyseal regions. The most common site of involvement is the axial skeleton, but any bone can be involved. Lesions are usually lytic with well demarcated borders but can present with an ill-defined border. However, in contrast to voriconazole-induced periostitis, skeletal coccidioidomycosis does not typically have a periosteal component and would be considered an unusual finding [11,12].
Li et al compiled a case series of patients with voriconazole-induced periosteitis, including case reports from 1998 to the end of 2021, which included 34 studies, retrospectively analyzing 44 patients, out of which 26 were female. The median time of onset of symptoms was 6 months from the start of voriconazole treatment [13]. Another study involving 59 patients indicated that the median daily dose of voriconazole was 600 mg [6]. Our patient was initially on 600 mg daily, and later her dose was increased to 700 mg daily. More studies are needed to determine the daily dose and duration of voriconazole, which seems to be the risk factor.
The optimal treatment for voriconazole-induced periostitis is not known. For most patients described, discontinuation of voriconazole resulted in prompt resolution of symptoms [6]. One case described a 64-year-old man who was treated for chronic lymphocytic leukemia, later complicated by coccidioidal meningitis. The patient continued the voriconazole treatment, but denosumab was added for its antiresorptive properties. The institution of denosumab was associated with symptomatic relief, although it was uncertain whether the denosumab reversed the periostitis process [14]. Other options tried at different institutions include reduction of the voriconazole by 50% to symptom relief, which might take a longer duration, and urinary alkalization with sodium bicarbonate [15,16]. More studies are required to develop a treatment method for the cases in which voriconazole discontinuation is not an option.
Following the withdrawal of the voriconazole, alkaline phosphatase levels can take 3 to 4 months to normalize [8,17]. In the situation of our patient, the alkaline phosphatase level was 296 units/L while taking voriconazole, and within 20 days of voriconazole discontinuation, a repeat level was 185 units/L and eventually normalized. Similarly, fluoride levels can take up to 3 to 8 weeks to show decline after the cessation [16,18]. For most patients described, pain usually improves by 2 weeks to 4 months after discontinuation of the medication [19]. Our patient had a startlingly rapid symptomatic improvement within 8 days of discontinuation of the voriconazole. Only 1 study in the literature mentions the time to a complete resolution of bone scan, at 6 months [20]. In our case, the bone scan done at 4 months of voriconazole discontinuation showed improvement.
Conclusions
Voriconazole-induced periosteitis should be considered in patients with musculoskeletal pain with a history of voriconazole treatment or elevated fluoride or bone alkaline phosphatase levels. Serum fluoride levels can be used as a cost-effective first-line test for patients taking voriconazole and presenting with skeletal pain. Discontinuation of the voriconazole results in rapid resolution of symptoms.
Figures
References:
1.. Bays DJ, Thompson GR, Coccidioidomycosis: Infect Dis Clin North Am, 2021; 35(2); 453-69
2.. Saubolle MA, McKellar PP, Sussland D, Epidemiologic, clinical, and diagnostic aspects of coccidioidomycosis: J Clin Microbiol, 2007; 45(1); 26-30
3.. Galgiani JN, Ampel NM, Blair JE, Infectious Diseases Society of America (IDSA) clinical practice guideline for the treatment of coccidioidomycosis: Clin Infect Dis, 2016; 63(6); e112-46
4.. Kim MM, Vikram HR, Kusne S, Treatment of refractory coccidioidomycosis with voriconazole or posaconazole: Clin Infect Dis, 2011; 53(11); 1060-66
5.. Wang TF, Wang T, Altman R, Periostitis secondary to prolonged voriconazole therapy in lung transplant recipients: Am J Transplant, 2009; 9(12); 2845-50
6.. Guarascio AJ, Bhanot N, Min Z, Voriconazole-associated periostitis: Pathophysiology, risk factors, clinical manifestations, diagnosis, and management: World J Transplant, 2021; 11(9); 356-71
7.. Nguyen QP, Wooten D, Voriconazole-induced periostitis in a patient with HIV treated for coccidioidomycosis meningitis: BMJ Case Rep, 2024; 17(1); e257884
8.. Tan I, Lomasney L, Stacy GS, Lazarus M, Mar WA, Spectrum of voriconazole-induced periostitis with review of the differential diagnosis: Am J Roentgenol, 2019; 212(1); 157-65
9.. Khokher MA, Dandona P, Fluoride stimulates [3H]thymidine incorporation and alkaline phosphatase production by human osteoblasts: Metabolism, 1990; 39(11); 1118-21
10.. Stefan S, Altork N, Alzedaneen Y, Voriconazole-induced diffuse periostitis: AACE Clin Case Rep, 2022; 8(5); 191-93
11.. Armbuster TG, Goergen TG, Resnick D, Catanzaro A, Utility of bone scanning in disseminated coccidioidomycosis: case report: J Nucl Med, 1977; 18(5); 450-54
12.. Zeppa MA, Laorr A, Greenspan A, Skeletal coccidioidomycosis: Imaging findings in 19 patients: Skeletal Radiol, 1996; 25(4); 337-43
13.. Li Z, Wu C, Wang C, Deng Z, Spectrum of voriconazole-associated periostitis in clinical characteristics, diagnosis and management: Infection, 2022; 50(5); 1217-24
14.. Rausch CR, Kontoyiannis DP, Prolonged voriconazole treatment in a patient with chronic lymphocytic leukemia resulting in a litany of chronic overlapping toxicities: J Oncol Pharm Pract, 2019; 25(3); 747-53
15.. Moon WJ, Scheller EL, Suneja A, Plasma fluoride level as a predictor of voriconazole-induced periostitis in patients with skeletal pain: Clin Infect Dis, 2014; 59(9); 1237-45
16.. Bennett MJ, Balcerek MI, Lewis EA, Voriconazole-associated periostitis: New insights into pathophysiology and management: JBMR Plus, 2022; 6(2); e10557
17.. Rossier C, Dunet V, Tissot F, Voriconazole-induced periostitis: Eur J Nucl Med Mol Imaging, 2012; 39(2); 375-76
18.. Gerber B, Guggenberger R, Fasler D, Reversible skeletal disease and high fluoride serum levels in hematologic patients receiving voriconazole: Blood, 2012; 120(12); 2390-94
19.. Tailor TD, Richardson ML, Case 215: voriconazole-induced periostitis: Radiology, 2015; 274(3); 930-35
20.. Türkkan S, Başaran FC, Tekçe YT, Yekeler E, Voriconazole-induced periostitis in a lung transplant recipient: Eurasian J Pulmonol, 2024; 26(1); 66-69
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133