24 December 2025: Articles 
Bronchial Arteriovenous Malformation Detection Prior to Catheter Ablation for Paroxysmal Atrial Flutter and Fibrillation: A Case Report
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Rare disease, Congenital defects / diseases
Alexandra ArvanitakiDOI: 10.12659/AJCR.949879
Am J Case Rep 2025; 26:e949879






Abstract
BACKGROUND: Catheter ablation for paroxysmal atrial flutter (PAFL) and atrial fibrillation (PAF) is a first-line treatment to maintain sinus rhythm. However, routine preprocedural imaging is not standardized, despite a high prevalence of incidental findings that may influence procedural planning. This report describes a case of a bronchial arteriovenous malformation (BAVM) detected on multidetector computed tomography prior to ablation in a patient with PAFL and PAF.
CASE REPORT: A 69-year-old woman who predominantly experienced episodes of PAFL, with occasional PAF, underwent pre-ablation multidetector computed tomography. Imaging demonstrated a serpiginous bronchial artery draining into the right pulmonary artery, with 2 aneurysms (approximately 1 cm proximal to the aortic origin and 4 cm proximal to the drainage site) in close proximity to the right pulmonary veins. Hemodynamic evaluation confirmed a non-significant left-to-right shunt, and a conservative approach was selected. Because of perioperative concerns about the BAVM’s location, the procedural plan was modified; rather than a combined procedure of pulmonary vein isolation with right isthmus ablation, only a typical PAFL ablation was performed. The patient had an uneventful post-procedural course, without arrhythmic recurrence or BAVM-related complications at 6 months. Annual follow-ups with contrast-enhanced computed tomography angiography were scheduled after joint cardiology and radiology consultation.
CONCLUSIONS: This case highlights the importance of systematic preprocedural imaging in PAF and PAFL ablation to detect unexpected intra- or extracardiac findings, such as a BAVM, that may affect procedural strategy and require a multidisciplinary approach.
Keywords: Ablation Techniques, Atrial Fibrillation, Atrial Flutter, Bronchial Fistula, computed tomography angiography, Humans, Female, Catheter Ablation, Aged, Arteriovenous Malformations, Bronchial Arteries, multidetector computed tomography
Introduction
Atrial fibrillation (AF) is the most prevalent sustained arrhythmia, affecting millions worldwide and strongly contributing to cardiovascular morbidity and mortality [1]. Although rate control and anticoagulation remain essential components of AF therapy, rhythm control through atrial fibrillation catheter ablation (AFCA) has demonstrated superior outcomes relative to antiarrhythmic agents in maintaining sinus rhythm, improving quality of life, and reducing long-term complications in selected groups [2].
Pre-procedural imaging is increasingly used to delineate pulmonary vein (PV) anatomy and left atrium size, and to exclude thrombi and structural abnormalities [3–5], as well as for integration into 3-dimensional mesh mapping models [6,7]. Multidetector computed tomography (MDCT) is often preferred over cardiac magnetic resonance imaging because of its faster acquisition time, higher spatial resolution, and compatibility with electroanatomical mapping integration [8,9]. Cardiac imaging modalities frequently reveal incidental findings (also reported as “collateral” findings) [10]; up to 69% of MDCT scans reportedly can identify incidental findings [11]. In addition to cardiac incidental findings, MDCT can detect extracardiac incidental findings in the lungs, abdomen, or chest wall, ranging from pulmonary nodules to vascular malformations, with important clinical and financial implications [12].
This report describes a 69-year-old woman with a bronchopulmonary arteriovenous malformation (BAVM) detected on MDCT prior to catheter ablation for paroxysmal atrial flutter (PAFL) and AF. This finding initiated a multidisciplinary discussion and ultimately modified the therapeutic approach.
Case Report
A 69-year-old woman with infrequent episodes of PAFL (Figure 1), occasionally alternating with paroxysmal atrial fibrillation (PAF), and arterial hypertension, was receiving oral rivaroxaban 20 mg once daily, amiodarone 200 mg once daily, nebivolol 2.5 mg once daily, and olmesartan/hydrochlorothiazide 20/12.5 mg once daily. She underwent an MDCT scan before planned PV ablation combined with a right isthmus procedure. The examination revealed normal coronary arteries without evidence of atherosclerotic lesions and identified a BAVM with the bronchial artery draining into the right pulmonary artery (Figure 2A, 2B). The bronchial artery had a prominent serpiginous course, and 2 aneurysms were present along its trajectory: a smaller aneurysm (1 cm in diameter) located immediately distal to its origin from the descending thoracic aorta, and a larger aneurysm (up to 4 cm in diameter) proximal to the drainage site into the right pulmonary artery. The larger aneurysm was positioned posteriorly and in close anatomical proximity to the right PVs (Figure 2C, 2D). A resting electrocardiogram did not reveal abnormalities (Figure 3), and transthoracic echocardiography performed after the BAVM diagnosis showed a left ventricle with normal size exhibiting preserved systolic and diastolic function (Figure 4).
Right and left heart catheterization was performed for hemodynamic evaluation of the shunt and for aortography to visualize the BAVM. Access was obtained through the right femoral vein and right femoral artery (7-Fr and 5-Fr catheters, respectively). The mean pulmonary artery pressure was 17 mmHg, with a pulmonary vascular resistance of 1.6 Wood units; pulmonary capillary wedge pressure was 12 mmHg. The indirect Fick method was used to calculate cardiac output. Blood samples were collected from the inferior and superior vena cava, right atrium, right and left pulmonary arteries, aorta, and PVs to determine oxygen saturation. The mean oxygen saturation value from left and right pulmonary arteries was used. The calculated Qp/Qs ratio was 1.4. During aortography, drainage of the bronchial artery into the pulmonary artery could not be visualized (Figure 5), likely because of contrast dilution within the pulmonary circulation.
Due to the hemodynamically non-significant left-to-right shunt, the absence of hemodynamic burden on the left ventricle, and the lack of symptoms, a conservative approach was selected for BAVM management. The close anatomical proximity of the aneurysmal segment to the PVs, as shown in Figure 2, led to concerns about increased procedural AFCA risk, specifically the potential for vascular injury or aneurysm-related complications during energy delivery. After completion of invasive and non-invasive diagnostic evaluation, the case was discussed in a multidisciplinary setting involving electrophysiologists, interventional cardiologists, adult congenital cardiologists, and radiologists. A shared decision was made to proceed only with right isthmus ablation and to monitor aneurysm size and morphology with annual computed tomography angiography (CTA); if the BAVM remained stable, scan repetition every 2–3 years was proposed. The low AF burden further supported postponement of AFCA.
After right isthmus ablation, the patient experienced an uneventful post-procedural course, without arrhythmic recurrence or BAVM-related complications at the 6-month follow-up. She remains under close follow-up by the electrophysiology team. The feasibility of PV ablation will be reassessed if PAF recurs. If AFCA is pursued, an interventional approach to occlude the BAVM (via transcatheter embolization) is likely to be a prudent step to assess subsequent PAF resolution and mitigate complications during PV isolation.
Discussion
A key takeaway from this case is that pre-ablative cardiac imaging, particularly with MDCT, can be essential for pre- and peri-procedural decision-making because it may reveal intra- or extracardiac incidental findings that require consideration. This report outlines an asymptomatic case of a primary BAVM, or “primary angioma arteriovenosum racemosum” (racemose hemangioma), identified during pre-procedural AFCA MDCT imaging [13]. The true incidence of BAVMs is unknown, and they are considered rare; no consistent sex predominance has been established, although several series have shown slightly higher rates in men [14,15]. The embryologic mechanisms underlying these anomalies remain unclear, but BAVMs generally represent abnormal direct connections between systemic bronchial arteries and PVs, bypassing the capillary bed network [16]. Progressive enlargement may occur with age as flow increases and the vessel walls weaken and stretch [17]. Although BAVMs most often present with hemoptysis, they may also remain clinically silent, as in the present case. Reported complications include hemomediastinum, hemothorax, and thromboembolism, primarily in the setting of rupture or aneurysm formation [14,18–23]. In our patient, the large aneurysm posed a theoretical risk of in situ thrombosis with subsequent pulmonary embolism, as well as the potential for embolic material migration during attempted occlusion.
Only a few publications describe similar BAVM cases discovered as incidental findings [24–28], and even fewer document detection solely through non-invasive imaging (computed tomography/CTA) without fluoroscopy. To our knowledge, this is the first reported asymptomatic BAVM identified during preprocedural AFCA assessment; it raises several questions regarding optimal management.
The question of whether to intervene in the BAVM is multifactorial. Although prophylactic treatment, including transcatheter embolization with N-butyl-2-cyanoacrylate (NBCA) and coils or surgical resection, has been described [27,29], intervention is generally reserved for symptomatic cases or those with evidence of hemodynamic significance. Accordingly, in the absence of symptoms, functional impairment, or hemodynamic overload, an interventional approach was considered unwarranted in the present case. However, the presence of a sizable aneurysmal segment along the bronchial artery requires regular follow-up. Similar asymptomatic cases have been discharged without a structured follow-up plan [24] or advised to undergo computed tomography surveillance every 6 months [25], but no optimal strategy has been defined. In the present case, annual follow-up with contrast-enhanced CTA was selected after joint cardiology and radiology consultation. Compared with magnetic resonance imaging, CTA provides superior spatial resolution, faster acquisition, and standardized protocols that enhance reproducibility for detailed aneurysm and vascular assessment [9]. We consider the benefits of CTA to outweigh the risks associated with radiation exposure, which were mitigated by appropriate spacing of imaging intervals. Other asymptomatic BAVM cases – managed conservatively and monitored with computed tomography/CTA – have demonstrated stable anatomy for periods ranging from 16 months to 5 years after diagnosis, without hemorrhage or lesion enlargement reported [24,25].
A particularly compelling consideration, which could potentially alter the treatment strategy, is the possibility of a direct contribution of the BAVM to AF pathogenesis. From a pathophysiological perspective, PVs serve as primary trigger zones for paroxysmal AF and thus are principal targets during AFCA [30]. In the present case, the second and larger aneurysm was located immediately posterior to the left atrial dome and in close proximity to the right superior PV. This anatomical region, often referred to as the venous pole or posterior hilum, is a conduit for extracardiac neural structures, including components of the autonomic nervous system. Mechanical compression or traction exerted by the aneurysm on adjacent cardiac tissue and neural pathways could contribute to arrhythmogenesis through neuroregulatory mechanisms or creation of electrical irritability zones. Similar phenomena have been reported in thoracic interventions, such as lung or mediastinal surgery, during which manipulation of perihilar structures has been associated with new-onset atrial arrhythmias [31]. These observations imply that the aneurysm itself contributed to this patient’s PAF episodes and that surgical or endovascular reduction of the aneurysmal mass effect could decrease atrial ectopy or AF burden by removing the mechanical and/or neurogenic stimulus. A potential association between frequently diagnosed coronary arteriovenous malformations and AF has also been proposed [32,33]. Although such hypotheses are noteworthy, they must be weighed carefully against the risks of intervention involving an otherwise asymptomatic lesion, particularly in the absence of definitive causal evidence.
Finally, in the context of a potential future need for AFCA, several periprocedural risks must be considered, requiring careful selection of the energy delivery strategy and extent of lesion formation. Conventional thermal ablation modalities, such as point-by-point radiofrequency ablation and cryoballoon ablation, have shown efficacy but may pose additional risk in this anatomical setting [34]. Radiofrequency ablation relies on resistive heating and has been associated with complications such as tamponade, PV stenosis, and thromboembolism, particularly when lesion depth or continuity is inadequate. Cryoballoon ablation – a simplified single-shot technique – may lack the necessary myocardial selectivity in a patient with adjacent vascular malformations. In contrast, pulsed field ablation, a nonthermal modality utilizing irreversible electroporation, may offer a distinct safety advantage because it preferentially ablates myocardial tissue while sparing adjacent non-cardiac structures (e.g., esophageal, neural, and vascular tissues). This characteristic could reduce the risk of aneurysm thrombosis or rupture, outcomes that are difficult to predict given the variable response of aneurysmal tissue to thermal injury [35]. Regarding lesion set selection, more extensive approaches – such as wide posterior wall isolation or box lesions – would increase procedural duration and inflammatory burden on the left atrium and surrounding structures.
Conclusions
This case highlights the importance of systematic preprocedural imaging in PAF/PAFL ablation to detect unexpected intra- or extracardiac findings, such as a BAVM, that may influence procedural strategy. BAVMs, although rare and often incidental, can pose substantial procedural risks during cardiac interventions. Key messages include: a) a multidisciplinary approach involving cardiologists, radiologists, and, when appropriate, thoracic or vascular surgeons is essential in complex cases without clear guidelines; b) the decision to intervene should be guided by a comprehensive risk–benefit assessment; and c) a standardized stratification approach would help to determine whether watchful surveillance is sufficient for asymptomatic BAVMs. Further research is needed to better estimate the frequency and clinical impact of intra- and extracardiac incidental findings prior to AFCA and to clarify whether routine non-invasive screening improves procedural outcomes.
Figures
 Figure 1. Electrocardiogram of paroxysmal anticlockwise re-entry atrial flutter, indicating right isthmus dependenceA “sawtooth” pattern of inverted flutter waves is present in leads II, III; an augmented vector foot and upright flutter waves are present in lead V1 (red circle).
Figure 1. Electrocardiogram of paroxysmal anticlockwise re-entry atrial flutter, indicating right isthmus dependenceA “sawtooth” pattern of inverted flutter waves is present in leads II, III; an augmented vector foot and upright flutter waves are present in lead V1 (red circle). 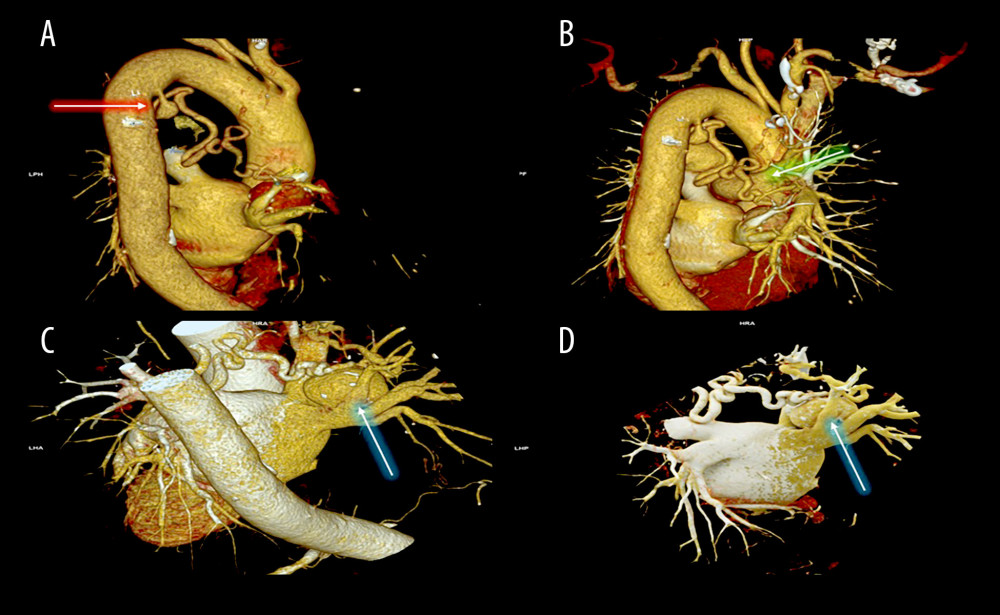 Figure 2. Three-dimensional computed tomography volume-rendering technique reconstruction of the bronchial arteriovenous malformation(A) Meandering course of the bronchial artery with a small aneurysm indicated near its origin from the thoracic aorta (red arrow). (B) The bronchial artery drains into the right pulmonary artery through a small branch (green arrow). (C, D) A larger saccular aneurysm with mural calcifications is noted distally along the bronchial artery near the left atrium (blue arrows).
Figure 2. Three-dimensional computed tomography volume-rendering technique reconstruction of the bronchial arteriovenous malformation(A) Meandering course of the bronchial artery with a small aneurysm indicated near its origin from the thoracic aorta (red arrow). (B) The bronchial artery drains into the right pulmonary artery through a small branch (green arrow). (C, D) A larger saccular aneurysm with mural calcifications is noted distally along the bronchial artery near the left atrium (blue arrows). 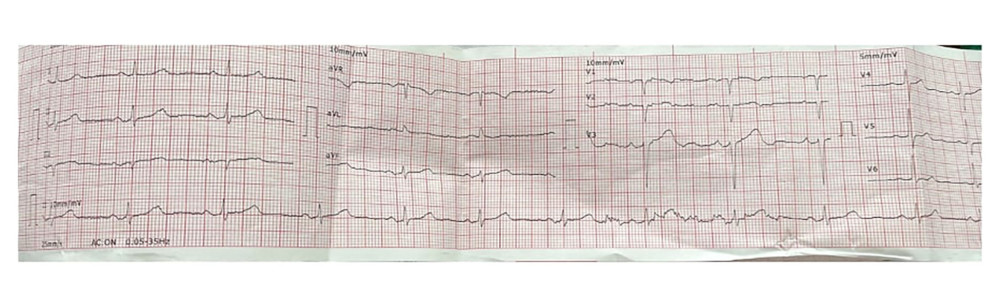 Figure 3. Resting electrocardiogram in sinus rhythm (55 beats/min)No cardiac pathology is present.
Figure 3. Resting electrocardiogram in sinus rhythm (55 beats/min)No cardiac pathology is present. 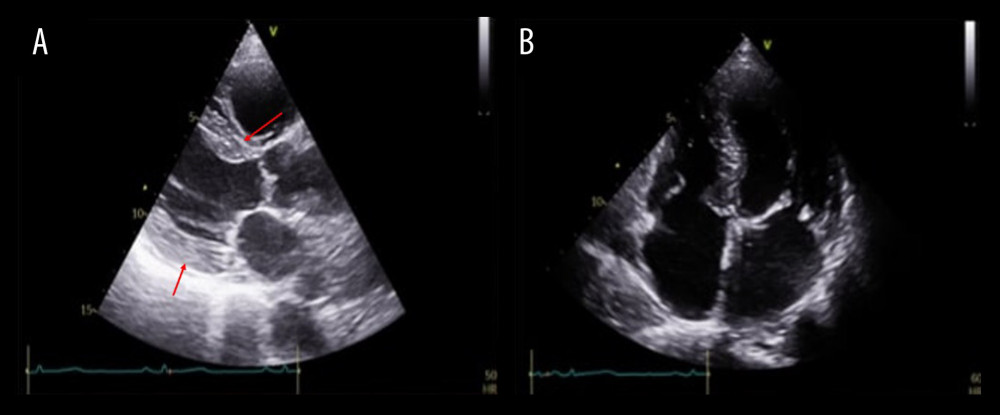 Figure 4. Transthoracic echocardiography(A) Parasternal long-axis view shows mild left ventricular hypertrophy (red arrows indicate interventricular septum and posterior wall of the left ventricle) due to arterial hypertension, with normal left ventricular size. (B) Apical 4-chamber view depicts normal biatrial size. Left ventricular function is within normal range.
Figure 4. Transthoracic echocardiography(A) Parasternal long-axis view shows mild left ventricular hypertrophy (red arrows indicate interventricular septum and posterior wall of the left ventricle) due to arterial hypertension, with normal left ventricular size. (B) Apical 4-chamber view depicts normal biatrial size. Left ventricular function is within normal range. 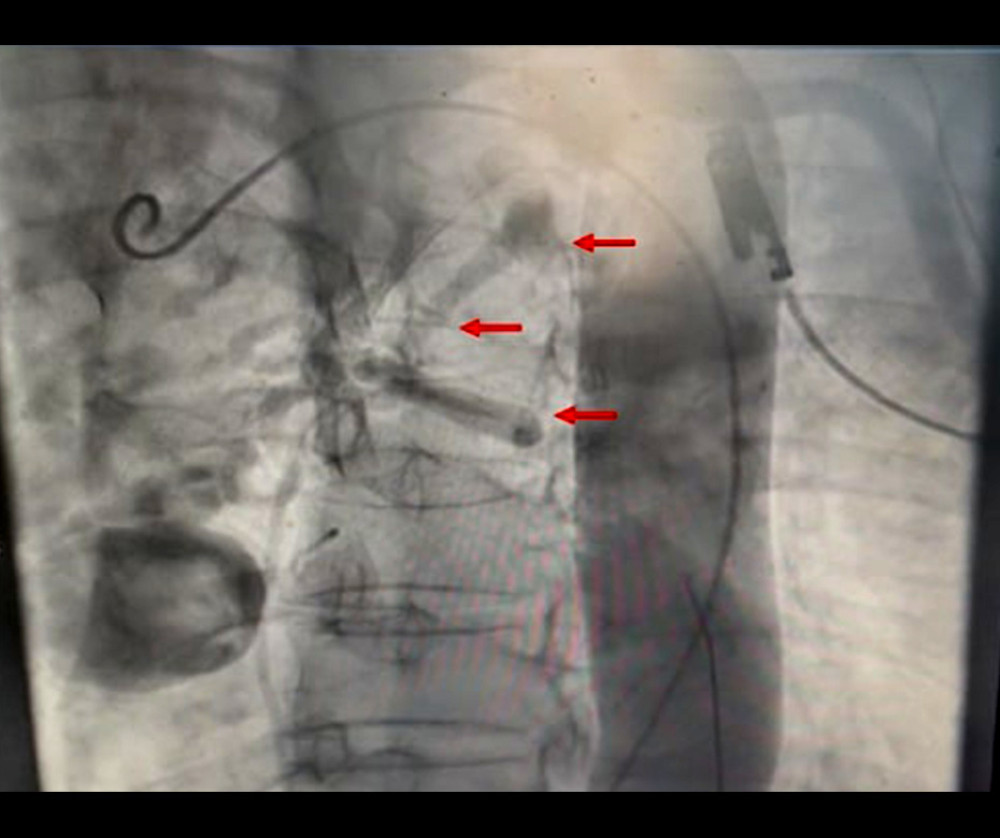 Figure 5. Invasive aortography assessment of the bronchial arteriovenous malformation (BAVM)Selective aortography demonstrates the BAVM arising from the descending thoracic aorta (red arrows). Opacification of drainage into the pulmonary artery is limited, likely due to contrast dilution within the pulmonary circulation.
Figure 5. Invasive aortography assessment of the bronchial arteriovenous malformation (BAVM)Selective aortography demonstrates the BAVM arising from the descending thoracic aorta (red arrows). Opacification of drainage into the pulmonary artery is limited, likely due to contrast dilution within the pulmonary circulation. References
1. Chugh SS, Havmoeller R, Narayanan K, Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study: Circulation, 2014; 129; 837-47
2. Van Gelder IC, Rienstra M, Bunting KV, 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): Eur Heart J, 2024; 45; 3314-414
3. Mansour M, Holmvang G, Sosnovik D, Assessment of pulmonary vein anatomic variability by magnetic resonance imaging: Implications for catheter ablation techniques for atrial fibrillation: J Cardiovasc Electrophysiol, 2004; 15; 387-93
4. Hunter RJ, Ginks M, Ang R, Impact of variant pulmonary vein anatomy and image integration on long-term outcome after catheter ablation for atrial fibrillation: Europace, 2010; 12; 1691-97
5. Ohana M, Bakouboula B, Labani A, Imaging before and after catheter ablation of atrial fibrillation: Diagn Interv Imaging, 2015; 96; 1113-23
6. Kistler PM, Rajappan K, Jahngir M, The impact of CT image integration into an electroanatomic mapping system on clinical outcomes of catheter ablation of atrial fibrillation: J Cardiovasc Electrophysiol, 2006; 17; 1093-101
7. Richmond L, Rajappan K, Voth E, Validation of computed tomography image integration into the EnSite NavX mapping system to perform catheter ablation of atrial fibrillation: J Cardiovasc Electrophysiol, 2008; 19; 821-27
8. Quintana RA, Dong T, Vajapey R, Preprocedural multimodality imaging in atrial fibrillation: Circ Cardiovasc Imaging, 2022; 15; e014386
9. Bardo DME, Brown P, Cardiac multidetector computed tomography: Basic physics of image acquisition and clinical applications: Curr Cardiol Rev, 2008; 4; 231-43
10. Perna F, Casella M, Narducci ML, Collateral findings during computed tomography scan for atrial fibrillation ablation: Let’s take a look around: World J Cardiol, 2016; 8; 310-16
11. Schietinger BJ, Bozlar U, Hagspiel KD, The prevalence of extracardiac findings by multidetector computed tomography before atrial fibrillation ablation: Am Heart J, 2008; 155; 254-59
12. Machaalany J, Yam Y, Ruddy TD, Potential clinical and economic consequences of noncardiac incidental findings on cardiac computed tomography: J Am Coll Cardiol, 2009; 54; 1533-41
13. Cain H, Spanel KEtiology and morphogenesis of the so-called bronchial arterioma: Klin Wochenschr, 1980; 58; 347-57 [in German]
14. Nabeta M, Koganemaru M, Takasu O, Ruptured aneurysm associated with bronchial arteriovenous malformation: Intern Med, 2016; 55; 849-50
15. Danyalian A, Sankari A, Hernandez F, Pulmonary arteriovenous malformation: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing
16. Walker CM, Rosado-de-Christenson ML, Martínez-Jiménez S, Bronchial arteries: Anatomy, function, hypertrophy, and anomalies: Radiographics, 2015; 35; 32-49
17. Burke CM, Safai C, Nelson DP, Pulmonary arteriovenous malformations: A critical update: Am Rev Respir Dis, 1986; 134; 334-39
18. Gorsi U, Sharma M, Jugpal TS, Bronchopulmonary arteriovenous malformation presenting as cryptogenic hemoptysis in a patient with bicuspid aortic valve: Lung India, 2020; 37; 257-59
19. Chen A-P, Li H-M, Yu H, Bronchopulmonary arteriovenous malformation – demonstrated by multidetector computed tomography angiography: Eur J Cardiothorac Surg, 2010; 37; 484
20. Vincze B, Lázár I, Mezei P, Spontaneous haemothorax – thoracic surgeon and intervention radiologist successful cooperation: Magy Seb, 2018; 71; 155-62
21. Seo Y-H, Kwak JY, Spontaneous hemomediastinum and hemothorax caused by a ruptured bronchial artery aneurysm: Korean J Thorac Cardiovasc Surg, 2011; 44; 314-17
22. Lococo F, Cafarotti S, Margaritora S, Hemomediastinum and hemothorax after dissecting bronchial artery aneurysm: The limit of the surgical option: Interact Cardiovasc Thorac Surg, 2011; 12; 621
23. Shimizu H, Tanabe N, Tatsumi KRacemose hemangioma of the bronchial artery: Nihon Rinsho, 2009; 67; 1038-41 [in Japanese]
24. Uchiyama D, Fujimoto K, Uchida M, Bronchial arteriovenous malformation: MDCT angiography findings: Am J Roentgenol, 2007; 188; W409-11
25. Ito A, Takao M, Shimamoto A, Primary racemose hemangioma with bronchial-pulmonary arterial fistula: Respirol Case Rep, 2018; 6; e00314
26. Tsukahara Y, Kurozumi M, Matsuda J, Successful embolization of a primary bronchial artery racemose hemangioma by the ingenious use of a microballoon catheter: Radiol Case Rep, 2024; 19; 4260-65
27. Yachi T, Nishida Y, Saito NRacemose hemangioma of the bronchial artery with pulmonary artery fistula: Kyobu Geka, 2022; 75; 1083-87 [in Japanese]
28. Takano R, Matsutani T, Hagiwara N, Racemose hemangioma of the bronchial artery mimicking esophageal submucosal tumor: A case report: Clin J Gastroenterol, 2020; 13; 1022-27
29. Saiga A, Sugiura T, Higashide T, Multiple enlarged aneurysms in primary racemose hemangioma of the bronchial artery: Successful prophylactic transcatheter arterial embolization using N-butyl-2-cyanoacrylate and coils: Cardiovasc Intervent Radiol, 2018; 41; 811-15
30. Bizhanov KA, Abzaliyev KB, Baimbetov AK, Atrial fibrillation: epidemiology, pathophysiology, and clinical complications (literature review): J Cardiovasc Electrophysiol, 2023; 34; 153-65
31. Bagheri R, Yousefi Y, Rezai R, Atrial fibrillation after lung surgery: Incidence, underlying factors, and predictors: Kardiochir Torakochirurgia Pol, 2019; 16; 53-56
32. Jamali HK, Raza U, Waqar F, Idiopathic atrial fibrillation and coronary arteriovenous fistulae: Is there a link?: Cardiology, 2016; 134; 433-35
33. Rämö OJ, Tötterman KJ, Harjula AL, Thrombosed coronary artery fistula as a cause of paroxysmal atrial fibrillation and ventricular arrhythmia: Cardiovasc Surg, 1994; 2; 720-72
34. Buist TJ, Zipes DP, Elvan A, Atrial fibrillation ablation strategies and technologies: Past, present, and future: Clin Res Cardiol, 2021; 110; 775-88
35. Shaheen N, Shaheen A, Ramadan A, Efficacy and safety of novel pulsed field ablation (PFA) technique for atrial fibrillation: A systematic review and meta-analysis: Health Sci Rep, 2023; 6; e1079
Figures
Figure 1. Electrocardiogram of paroxysmal anticlockwise re-entry atrial flutter, indicating right isthmus dependenceA “sawtooth” pattern of inverted flutter waves is present in leads II, III; an augmented vector foot and upright flutter waves are present in lead V1 (red circle).Figure 2. Three-dimensional computed tomography volume-rendering technique reconstruction of the bronchial arteriovenous malformation(A) Meandering course of the bronchial artery with a small aneurysm indicated near its origin from the thoracic aorta (red arrow). (B) The bronchial artery drains into the right pulmonary artery through a small branch (green arrow). (C, D) A larger saccular aneurysm with mural calcifications is noted distally along the bronchial artery near the left atrium (blue arrows).Figure 3. Resting electrocardiogram in sinus rhythm (55 beats/min)No cardiac pathology is present.Figure 4. Transthoracic echocardiography(A) Parasternal long-axis view shows mild left ventricular hypertrophy (red arrows indicate interventricular septum and posterior wall of the left ventricle) due to arterial hypertension, with normal left ventricular size. (B) Apical 4-chamber view depicts normal biatrial size. Left ventricular function is within normal range.Figure 5. Invasive aortography assessment of the bronchial arteriovenous malformation (BAVM)Selective aortography demonstrates the BAVM arising from the descending thoracic aorta (red arrows). Opacification of drainage into the pulmonary artery is limited, likely due to contrast dilution within the pulmonary circulation. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133