19 December 2025: Articles 
Primary Orbital Lymphoma Manifesting as Increased Intraocular Pressure: A Case Report
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment
Miaomiao Sun AEG 1, Zhaohui Xiong F 1, Yincong Xu B 1, Zhongyou Zhou F 1, Jiale Wu BC 1, Jiangzhou Han BC 1, Lina Zhao A 1*DOI: 10.12659/AJCR.951048
Am J Case Rep 2025; 26:e951048






Abstract
BACKGROUND: Lymphoma can involve any orbital soft tissue (excluding bone) and may mimic other orbital diseases, often leading to misdiagnosis. Early diagnosis improves both disease management and patient survival. This rare case provides insights into the early diagnosis and treatment of orbital lymphoma.
CASE REPORT: An 87-year-old Asian man presented with sudden swelling of the left eyelid, vision loss, and severe pain. His intraocular pressure increased, and vision eventually deteriorated to no light perception. Biopsy of the orbital mass revealed small cell malignancy. Immunohistochemistry showed CD20(+++), Bcl-6(+++), and other markers consistent with diffuse large B-cell lymphoma. The patient received combined chemotherapy and radiotherapy, which relieved swelling and pain but did not restore vision.
CONCLUSIONS: Orbital lymphoma may present with or without systemic symptoms. Its clinical and imaging features often overlap with other orbital diseases, contributing to misdiagnosis. Pathogenesis plays a critical role in prognosis, emphasizing the importance of early diagnosis to improve outcomes. This case is among the few reported in which initial presentation included elevated intraocular pressure.
Keywords: Intraocular Pressure, Lymphoma, Large B-Cell, Diffuse, Vision Disorders, Humans, Male, Orbital Neoplasms, Aged, 80 and over, Ocular Hypertension, Lymphoma, Diagnosis, Differential
Introduction
Primary ocular lymphoma, comprising primary intraocular lymphoma and primary orbital lymphoma, is a rare malignancy due to the limited presence of native lymphatic tissue in the orbit [1]. Orbital lymphoma represents approximately 10% of all orbital neoplasms and 2% of all lymphoid and extranodal lymphomas, making it the most common orbital malignancy in adults [2]. According to the conventional definition, primary orbital lymphoma is confined to orbital tissues such as the lacrimal gland, conjunctiva, or extraocular muscles, without initial involvement of intraocular structures. The main clinical manifestations include slow enlargement of painless or occasionally painful peri-orbital masses, peri-orbital swelling, ptosis, exophthalmos, decreased vision, diplopia, strabismus, and optic nerve compression. A characteristic “salmon patch” lesion on the conjunctiva is well documented but not pathognomonic. These nonspecific findings, which mimic various benign and malignant orbital conditions, together with the rarity of the disease, frequently result in delayed or incorrect diagnosis. Diagnostic challenges are most evident in atypical presentations that divert clinical suspicion from lymphoma. An important but underreported manifestation is elevated intraocular pressure, which can resemble refractory glaucoma and lead to inappropriate management. Because the pathogenesis of lymphoma is closely linked to its prognosis, early and accurate diagnosis is critical for appropriate treatment selection and improved survival.
This case report describes an unusual presentation of primary orbital lymphoma in which the initial and predominant symptom was substantially increased intraocular pressure. It emphasizes the diagnostic challenges associated with such cases and highlights the need for greater clinical vigilance. Furthermore, potential mechanisms underlying intraocular pressure elevation are discussed; we suggest inclusion of lymphoma in the differential diagnosis of unilateral ocular hypertension resistant to standard therapy. Recognition of this possibility may lead to earlier diagnosis and better patient outcomes.
Case Report
CHIEF COMPLAINTS:
An 87-year-old Asian man presented to a local hospital with sudden swelling of the left eyelid and vision loss in the same eye (Figure 1). Ophthalmic examination revealed visual acuities of 20/50 in the right eye and 20/80 in the left eye. The patient reported binocular diplopia. Examination of the left eye showed absence of the pupillary light reflex and complete restriction of ocular movement, resulting in a fixed forward gaze. Intraocular pressures were 13.5 mmHg in the right eye and 27 mmHg in the left eye. Notably, the initial presentation of substantially elevated intraocular pressure mimicking unilateral ocular hypertension is an exceedingly rare and diagnostically challenging manifestation of orbital lymphoma that often leads to misdiagnosis and treatment delay. Ocular hypertension in the left eye was suspected, and carteolol hydrochloride eye drops were prescribed to reduce intraocular pressure.
Three days later, the patient exhibited minimal improvement, and his eye pain had worsened; thus, he sought treatment at our hospital. The patient expressed a strong desire for pain relief. Reevaluation showed visual acuity of 20/133 in the left eye and intraocular pressure between 30 and 40 mmHg. Swelling of the left eyelid had progressively worsened and was accompanied by ptosis. The patient received steroid pulse therapy, but improvement was minimal. Vision in the left eye gradually declined to complete loss of light perception, with persistent severe pain. At this stage, the patient had a 3-month history of symptoms in the left eye. Upon further evaluation at our hospital, the right eye appeared essentially normal. The left eye displayed pronounced eyelid swelling, increased skin tension, and stiffness of the skin and subcutaneous tissue, resulting in complete inability to open the eyelid. When the eyelid was partially opened manually, pronounced edema of the bulbar conjunctiva was observed. The cornea was transparent, and the anterior chamber depth was normal. The pupil measured approximately 4 mm in diameter and was nonreactive to light. The lens was cloudy, and fundus examination could not be performed.
HISTORY OF PAST ILLNESS:
The patient had no history of ocular trauma or surgery, and no history of systemic allergy. He had undergone surgical treatment for a small intestinal stromal tumor more than 10 years earlier. After the procedure, he received Gleevec (imatinib) therapy for approximately 11 months. Regular follow-up assessments confirmed that his condition was stable. Eosinophilia was detected 1 year prior to the present case; it improved after oral administration of prednisone acetate.
PERSONAL AND FAMILY HISTORY:
The patient’s parents had died of natural causes and had been in good health during their lifetimes. There was no family history of cancer, hypertension, diabetes, stroke, or myocardial infarction on either side. The patient’s children were alive and in good health.
PHYSICAL EXAMINATION ON ADMISSION:
Slit-lamp examination revealed no abnormalities in the right eye. The left eye showed prominent eyelid swelling and conjunctival edema without a distinct “salmon patch.” The conjunctival and episcleral vessels were thickened and engorged. The anterior chamber depth was normal; both the lens and vitreous were cloudy. Fundus examination of the left eye showed a reddish optic disc with a cup-to-disc ratio of approximately 0.5. Retinal vessels demonstrated a normal course, the retina appeared flat, and the macular fovea was normal. The patient exhibited a poor mental state and anemic appearance without systemic lymph node enlargement.
IMAGING EXAMINATIONS:
Orbital computed tomography (Figure 2) revealed deformation of the left globe with diffuse involvement of the intra- and extraconal regions, characterized by globe tenting and optic nerve stretching. Additional findings included soft tissue thickening along the left posterior nasopharyngeal wall and a nodule behind the right inferior turbinate. The left orbital mass was initially regarded as an inflammatory pseudotumor.
:
Blood test results were as follows: white blood cell count 5.4×109/L, red blood cell count 1.69×1012/L, hemoglobin 68 g/L, platelet count 300×109/L, albumin 25.2 g/L, lymphocyte percentage 41.1%, and neutrophil percentage 47.1%. Given these findings, ocular lymphoma was suspected. Computed tomography-guided orbital mass biopsy was performed; a single specimen (approximately 0.6 cm in length and 0.1 cm in diameter) was obtained from both the left orbital region and the left nasal region.
:
At low-power magnification (4×), a dense, infiltrative lesion with a diffuse growth pattern was observed. The lesion lacked well-defined margins and had invaded the surrounding tissue, consistent with a high-grade neoplasm. No organized structures such as follicles or glands were present. At high-power magnification (40×), clusters of large, atypical lymphoid cells were visible, characterized by irregular nuclear contours, prominent nucleoli, and dispersed chromatin. Numerous mitotic figures indicated rapid cellular proliferation. The absence of differentiation toward other hematologic lineages further supported a diagnosis of lymphoid malignancy.
IMMUNOHISTOCHEMISTRY FINDINGS:
Cluster of differentiation (CD)45 (++), CD3 (−), CD45R0 (−), CD79a (−), CD20 (+++), B-cell lymphoma (Bcl)-2 (−), Bcl-6 (+++), multiple myeloma oncogene 1 (MUM-1; −), CD10 (−), and Cyclin D1 (−).
FINAL DIAGNOSIS:
Histopathological findings combined with immunohistochemical analysis confirmed the diagnosis of non-Hodgkin diffuse large B-cell lymphoma (DLBCL) with a germinal center B-cell phenotype. Strong CD20 and Bcl-6 positivity, together with negative staining results for CD3, CD10, and Cyclin D1, supported this diagnosis. This case is exceptionally rare and clinically significant because the initial presentation was characterized by a pronounced increase in intraocular pressure as the predominant symptom, mimicking refractory unilateral glaucoma. This atypical presentation deviated from the more common manifestations of orbital lymphoma, such as a palpable mass or proptosis, and directly contributed to the initial misdiagnosis and management as ocular hypertension. This report contributes meaningfully to the literature by emphasizing that orbital lymphoma, despite its rarity, should be included in the differential diagnosis of unexplained unilateral ocular hypertension, particularly when the symptoms are resistant to standard pressure-lowering therapy. The report also underscores the importance of comprehensive orbital imaging and early biopsy in atypical cases to prevent diagnostic delay and optimize patient outcomes.
TREATMENT, OUTCOME, AND FOLLOW-UP PLAN:
The patient expressed a strong desire for pain relief. After informed consent had been obtained from the patient and his family, radiotherapy was administered to the left orbital mass with a prescribed total dose of 40 Gy, delivered in 20 fractions of 2 Gy each. Concurrently, chemotherapy was initiated using the R-CHOP regimen, consisting of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone. After completion of 6 cycles of radiotherapy, considerable improvement in swelling (Figure 1) and pain in the left eye was observed. However, due to the prolonged course of the disease before treatment, the patient had already lost light perception upon admission, and visual function did not recover.
The follow-up plan for this older male patient with ocular non-Hodgkin DLBCL was designed to monitor treatment response, detect recurrence, and manage complications while maintaining quality of life. Initially, monthly assessments included ophthalmic examinations, systemic evaluations, and immunological monitoring; whole-body imaging was performed every 3 months. During the mid-term follow-up period (months 6–12), evaluations were conducted less frequently but continued to monitor visual function, systemic condition, and quality of life. Long-term follow-up was scheduled every 3 to 6 months, eventually transitioning to annual visits; these visits included ocular and systemic evaluations with an emphasis on preventing visual impairment, detecting recurrence, and managing immunosuppression-related risks. Any sudden visual decline or systemic symptoms warranted immediate re-evaluation. This follow-up strategy ensured dynamic treatment adjustments based on the patient’s evolving clinical condition.
Discussion
Orbital lymphomas represent approximately 1% to 2% of all non-Hodgkin lymphomas [2]. Most orbital lymphomas are of B-cell origin; extranodal marginal zone B-cell lymphoma is the most frequent subtype, followed by DLBCL, follicular lymphoma, and mantle cell lymphoma [3]. Follicular lymphoma is classified as a low-grade lymphoma, whereas DLBCL and Burkitt lymphoma constitute high-grade types. In a multicenter study from Asia, Savino et al [4] found that DLBCL was the second most common subtype of orbital lymphoma. More than half of affected patients showed systemic involvement, such as fever, night sweats, or weight loss. A large network study subsequently revealed that the median age at diagnosis of ocular lymphoma was approximately 64 years, and DLBCL cases were evenly distributed between the sexes [5].
Overwhelmingly, B-cell lymphomas manifest as unilateral tumors because of the absence of lymphoid tissue connections between the bilateral orbits [3]. The unilateral presentation in our patient, accompanied by increased intraocular pressure and vision loss, is consistent with this pattern, although approximately 10% of cases present bilaterally [6]. Most B-cell lymphomas are located in the extraorbital space, and some arise in the retrobulbar region [3]. Clinical manifestations vary according to tumor location. Woolf et al [6] reported that conjunctival disease constituted nearly 40% of all cases and represented the most common site of orbital lymphoma. Early conjunctival lymphoma may appear as a painless “salmon patch” on the conjunctiva, typically without limitation of ocular movement. The present case was atypical because the patient presented with pronounced conjunctival edema and elevated intraocular pressure in the absence of a classic “salmon patch,” which initially diverted diagnostic consideration away from lymphoma. As the disease progressed and involved periocular and intraocular structures, symptoms such as eye pain, eyelid swelling, and ptosis developed, prompting computed tomography imaging that revealed a mass compressing the optic nerve.
The diagnosis of orbital lymphoma primarily relies on histopathologic confirmation via biopsy. In terms of classification, B-cell lymphoma is identified using markers such as Bcl-2, Bcl-6, CD10, CD23, CD30, Cyclin D1, MUM-1, and κ and λ light chains [7]. The immunohistochemical profile in the present case – CD20 (+++), Bcl-6 (+++), CD10 (−), and MUM-1 (−) – definitively confirmed DLBCL of the germinal center B-cell subtype, which guided subsequent therapeutic management [8].
A central and highly unusual feature of this case was the initial presentation with refractory ocular hypertension. Intraocular lymphoma is known to elevate intraocular pressure through multiple mechanisms, including neovascular glaucoma resulting from retinal infiltration, secondary glaucoma caused by central retinal vein occlusion, and secondary angle-closure glaucoma due to direct invasion of the ciliary body [9]. However, orbital lymphoma primarily manifesting as ocular hypertension is exceedingly rare. This atypical presentation posed a serious diagnostic challenge, leading to an initial misdiagnosis of unilateral ocular hypertension and a critical delay in recognizing the underlying malignancy. Our case is consistent with, and reinforces, the limited literature available regarding this phenomenon. Sears et al [10] and Kim et al [9] reported similar cases in which orbital lymphoma mimicked glaucoma by increasing episcleral venous pressure through a mass effect that impeded aqueous outflow. In our patient, prominent conjunctival edema was observed around the left ocular margin, with thickened and engorged superficial vessels. Although no “salmon patch” lesions were evident, conjunctival lymphoma had developed. On the scleral surface, anterior ciliary veins connect to Schlemm’s canal through intrascleral collector channels and aqueous veins. Consistent with previous findings, the mass effect and conjunctival infiltration by lymphoma likely increased pressure within the superficial scleral veins, reducing aqueous humor outflow and enhancing intraocular pressure. Consequently, intraocular pressure gradually decreased with lymphoma-directed treatment.
The decision to administer combined radiotherapy and R-CHOP chemotherapy to this 87-year-old patient required careful consideration. Despite the patient’s advanced age, the aggressive behavior of DLBCL and the favorable response of the germinal center B-cell subtype to immunochemotherapy warranted a definitive systemic approach. R-CHOP remains the global standard for DLBCL management, and its efficacy in orbital disease has been supported by studies demonstrating improved prognosis [3,11]. Radiotherapy at a total dose of 40 Gy was administered to achieve rapid local tumor control, addressing the mass effect responsible for pain and optic nerve compression. This combined modality treatment balanced curative intent with palliation of severe local symptoms. The decision was made collaboratively with the patient and his family, who prioritized pain relief. After 11 days of treatment, eyelid swelling had nearly resolved; conjunctival hyperemia and edema were substantially improved. However, due to delays regarding diagnosis and treatment initiation, visual function could not be restored.
The prognosis of primary orbital lymphoma is generally favorable; however, DLBCL is associated with worse outcomes. Negative prognostic factors include advanced age and non-mucosa-associated lymphoid tissue histology [12]. The diagnostic delay in the present case – resulting directly from the atypical presentation – contributed to irreversible vision loss and highlights the clinical consequences of diagnostic delay. Although combined modality therapy, including rituximab-based chemotherapy (R-CHOP), has greatly improved outcomes in orbital DLBCL [3,11], our experience indicates that success ultimately depends on early recognition. The present case provides an important insight for ophthalmic oncology: maintaining a high index of suspicion regarding malignancy in atypical glaucoma presentations is essential to prevent diagnostic delay, guide appropriate biopsy and imaging, and preserve vision while improving survival outcomes.
Conclusions
When patients present with increased intraocular pressure, conjunctival edema, and ocular swelling, the possibility of ocular lymphoma should be carefully considered. Timely diagnosis and appropriate treatment can substantially improve prognosis and visual outcomes.
Figures
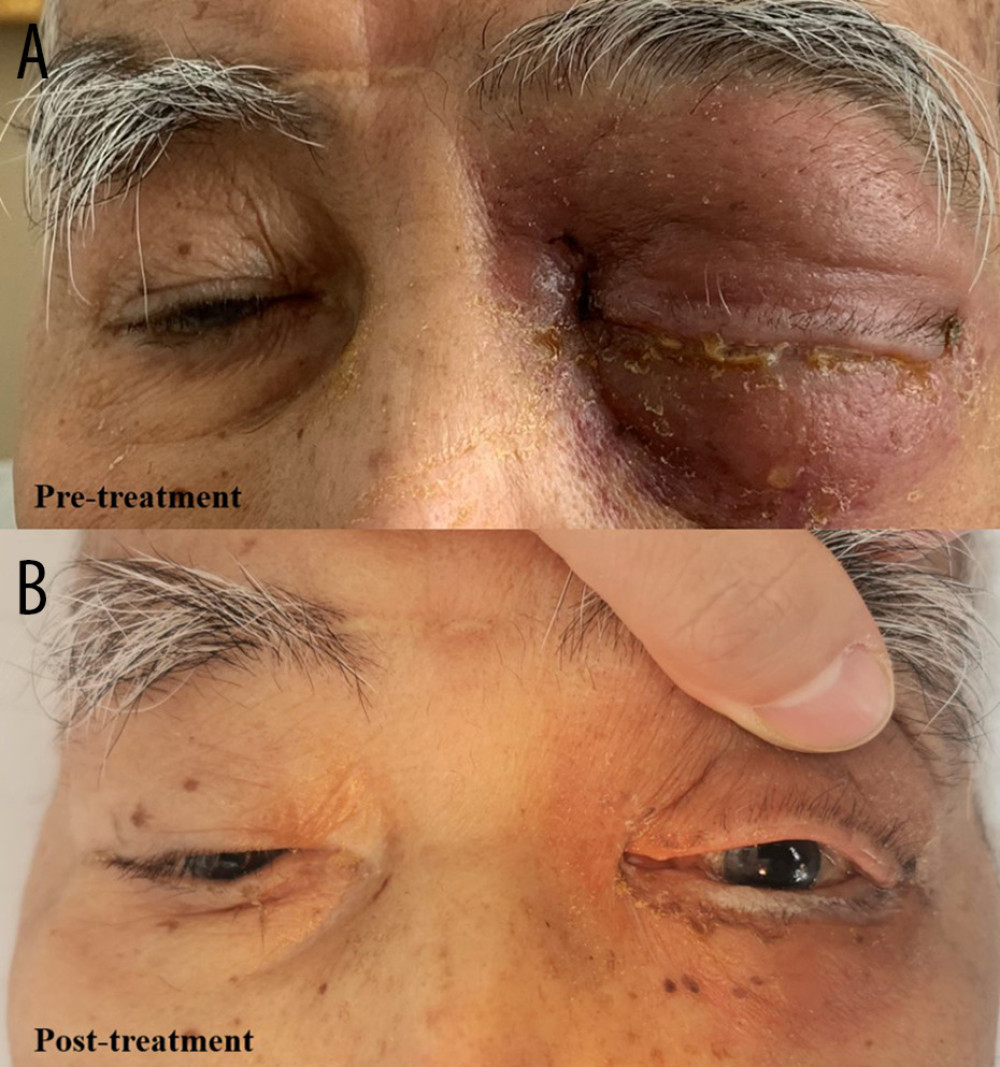 Figure 1. (A) The patient’s ocular condition at admission. The right eye appeared essentially normal; the left eye demonstrated severe eyelid swelling, increased skin tension, and rigidity of the skin and subcutaneous tissues, preventing voluntary eye opening. Ocular motility was completely restricted and fixed. (B) After chemoradiotherapy, there was a substantial reduction in eyelid edema within the left eye, as well as pronounced improvement in skin tension. The patient was able to open the eye with assistance.
Figure 1. (A) The patient’s ocular condition at admission. The right eye appeared essentially normal; the left eye demonstrated severe eyelid swelling, increased skin tension, and rigidity of the skin and subcutaneous tissues, preventing voluntary eye opening. Ocular motility was completely restricted and fixed. (B) After chemoradiotherapy, there was a substantial reduction in eyelid edema within the left eye, as well as pronounced improvement in skin tension. The patient was able to open the eye with assistance. 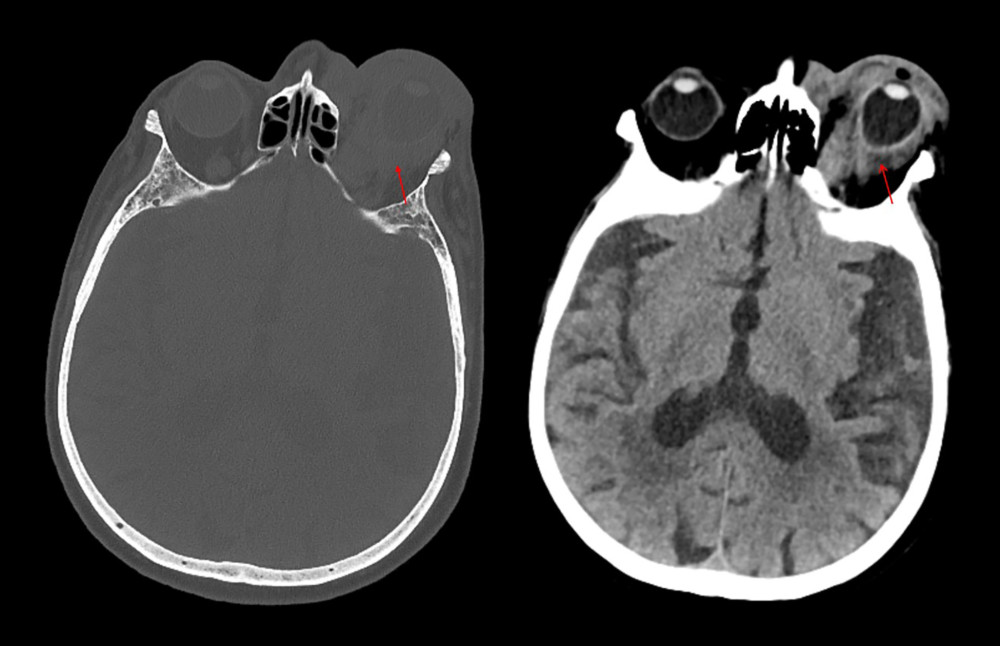 Figure 2. Orbital computed tomography scans revealed deformation of the left globe, indicating structural pathology. Images showed diffuse involvement of both intra- and extraconal spaces, suggesting extensive lesions possibly due to inflammatory or neoplastic processes. The tent-shaped configuration of the globe suggested increased tension, likely resulting from an internal mass or edema. Evidence of optic nerve traction was also present, possibly secondary to elevated intraocular pressure or direct compression. Soft tissue thickening along the posterior wall of the left nasopharynx was noted, which may represent inflammation or a mass.
Figure 2. Orbital computed tomography scans revealed deformation of the left globe, indicating structural pathology. Images showed diffuse involvement of both intra- and extraconal spaces, suggesting extensive lesions possibly due to inflammatory or neoplastic processes. The tent-shaped configuration of the globe suggested increased tension, likely resulting from an internal mass or edema. Evidence of optic nerve traction was also present, possibly secondary to elevated intraocular pressure or direct compression. Soft tissue thickening along the posterior wall of the left nasopharynx was noted, which may represent inflammation or a mass. 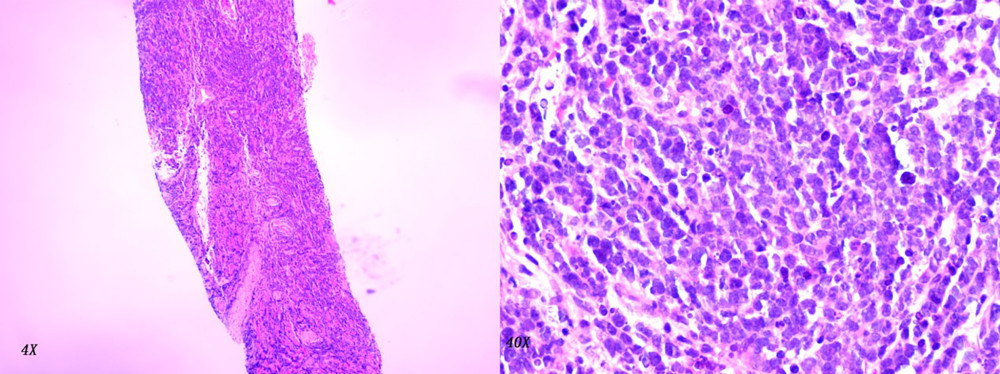 Figure 3. At low-power magnification (4×), a dense, infiltrative lesion with a diffuse growth pattern was observed. The lesion lacked distinct margins and invaded adjacent tissues, consistent with a high-grade neoplasm. No organized structures such as follicles or glands were present. At high-power magnification (40×), clusters of large, atypical lymphoid cells were visible, characterized by irregular nuclear contours, prominent nucleoli, and dispersed chromatin. Numerous mitotic figures indicated rapid cellular proliferation. The absence of differentiation toward other hematologic lineages further supported a diagnosis of lymphoid malignancy.
Figure 3. At low-power magnification (4×), a dense, infiltrative lesion with a diffuse growth pattern was observed. The lesion lacked distinct margins and invaded adjacent tissues, consistent with a high-grade neoplasm. No organized structures such as follicles or glands were present. At high-power magnification (40×), clusters of large, atypical lymphoid cells were visible, characterized by irregular nuclear contours, prominent nucleoli, and dispersed chromatin. Numerous mitotic figures indicated rapid cellular proliferation. The absence of differentiation toward other hematologic lineages further supported a diagnosis of lymphoid malignancy. 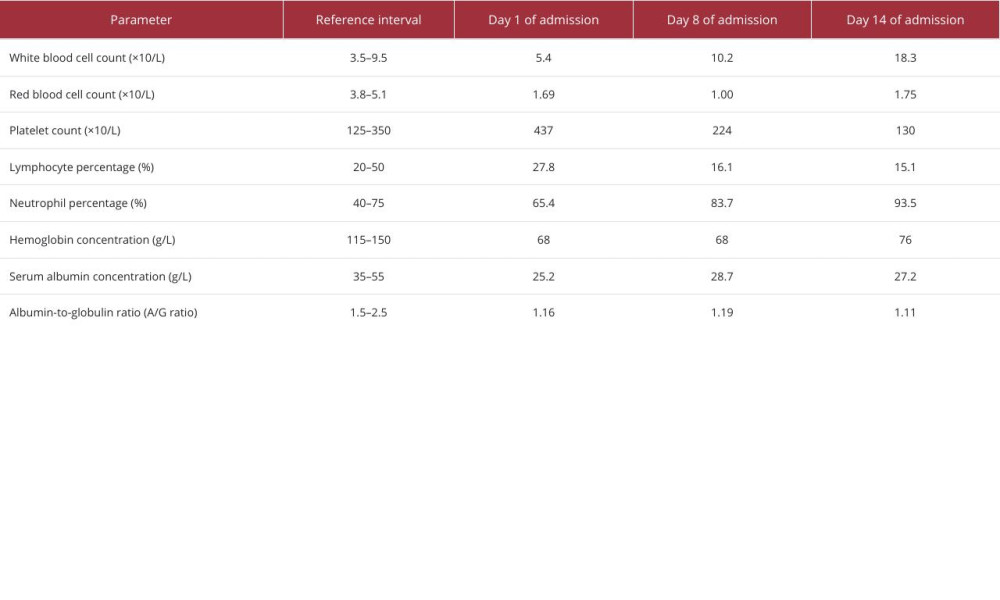
References
1. Rubinstein TJ, Aziz HA, Bellerive C, Ocular/adnexal lymphoma: Dissimilar to systemic lymphoma: Surv Ophthalmol, 2018; 63(3); 381-88
2. Eckardt AM, Lemound J, Rana M, Gellrich NC, Orbital lymphoma: Diagnostic approach and treatment outcome: World J Surg Oncol, 2013; 11; 73
3. Olsen TG, Heegaard S, Orbital lymphoma: Surv Ophthalmol, 2019; 64(1); 45-66
4. Savino G, Midena G, Blasi MA, Orbital and eyelid B-cell lymphoma: A multicenter retrospective study: Cancers (Basel), 2020; 12(9); 2538
5. Olsen TG, Holm F, Mikkelsen LH, Orbital lymphoma-an international multicenter retrospective study: Am J Ophthalmol, 2019; 199; 44-57
6. Woolf DK, Ahmed M, Plowman PN, Primary lymphoma of the ocular adnexa (orbital lymphoma) and primary intraocular lymphoma: Clin Oncol (R Coll Radiol), 2012; 24(5); 339-44
7. Sjö LD, Ophthalmic lymphoma: Epidemiology and pathogenesis: Acta Ophthalmol, 2009; 87(Thesis 1); 1-20
8. Coupland SE, Molecular pathology of lymphoma: Eye (Lond), 2013; 27(2); 180-89
9. Kim WI, Larar JG, Cheson BD, Resolution of lymphoma-associated open-angle glaucoma by rituximab: J Glaucoma, 2011; 20(6); 398-400
10. Sears NC, Singh A, Singh AD, Ocular adnexal lymphoma presenting as refractory unilateral open-angle glaucoma: J Glaucoma, 2016; 25(8); e741-44
11. Martinet S, Ozsahin M, Belkacémi Y, Outcome and prognostic factors in orbital lymphoma: A Rare Cancer Network study on 90 consecutive patients treated with radiotherapy: Int J Radiat Oncol Biol Phys, 2003; 55(4); 892-98
12. Kalicińska E, Giza A, Zaucha JM, A survey across orbital lymphoma in Poland: Multicenter retrospective study of Polish Lymphoma Research Group (PLRG): Cancer Med, 2023; 12(3); 3036-45
Figures
Figure 1. (A) The patient’s ocular condition at admission. The right eye appeared essentially normal; the left eye demonstrated severe eyelid swelling, increased skin tension, and rigidity of the skin and subcutaneous tissues, preventing voluntary eye opening. Ocular motility was completely restricted and fixed. (B) After chemoradiotherapy, there was a substantial reduction in eyelid edema within the left eye, as well as pronounced improvement in skin tension. The patient was able to open the eye with assistance.Figure 2. Orbital computed tomography scans revealed deformation of the left globe, indicating structural pathology. Images showed diffuse involvement of both intra- and extraconal spaces, suggesting extensive lesions possibly due to inflammatory or neoplastic processes. The tent-shaped configuration of the globe suggested increased tension, likely resulting from an internal mass or edema. Evidence of optic nerve traction was also present, possibly secondary to elevated intraocular pressure or direct compression. Soft tissue thickening along the posterior wall of the left nasopharynx was noted, which may represent inflammation or a mass.Figure 3. At low-power magnification (4×), a dense, infiltrative lesion with a diffuse growth pattern was observed. The lesion lacked distinct margins and invaded adjacent tissues, consistent with a high-grade neoplasm. No organized structures such as follicles or glands were present. At high-power magnification (40×), clusters of large, atypical lymphoid cells were visible, characterized by irregular nuclear contours, prominent nucleoli, and dispersed chromatin. Numerous mitotic figures indicated rapid cellular proliferation. The absence of differentiation toward other hematologic lineages further supported a diagnosis of lymphoid malignancy. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133