02 November 2021: Articles 
Glucocorticoids Induce Partial Remission of Focal Segmental Glomerulosclerosis but Not Interstitial Nephritis in COVID-19 Acute Kidney Injury in an APOL1 Low-Risk Genotype White Patient
Challenging differential diagnosis, Rare coexistence of disease or pathology
Piotr J. Nowak1ABCDEF*, Joanna Forycka2BCEF, Natalia Cegielska2BCEF, Karolina Harendarz2BCEF, Małgorzata Wągrowska-Danilewicz3BCD, Marian Danilewicz4BCD, Tomasz Płoszaj5BCD, Maciej Borowiec5CDG, Rafał Wlazeł6BCD, Michał Nowicki1DEGDOI: 10.12659/AJCR.933462
Am J Case Rep 2021; 22:e933462






Abstract
BACKGROUND: COVID-19 can be complicated by kidney disease, including focal segmental glomerulosclerosis (FSGS), interstitial nephritis, and acute kidney injury (AKI). Almost all known cases of COVID-19-associated glomerulonephritis have been in patients of African descent, with G1 or G2 apolipoprotein L1 (APOL1) risk alleles, and they presented collapsing type of FSGS.
CASE REPORT: We report a case of biopsy-confirmed non-collapsing FSGS with secondary acute interstitial nephritis and AKI in a young White man with APOL1 low-risk genotype, who had COVID-19 pneumonia. His past history included arterial hypertension, anabolic steroids, and high-protein diet. He fully recovered from type 1 respiratory failure and AKI after transfusion of COVID-19 convalescent plasma and intravenous treatment with dexamethasone administered for 16 days in a dose reduced from 16 to 2 mg/day. Due to progressing severe nephrotic proteinuria (22.6 g/24 h), intravenous methylprednisolone was administered (1500 mg divided in 3 pulses over 3 days) immediately followed by oral prednisone (0.6 mg/kg body weight), with dose reduced 19 weeks later and switched to cyclosporine A (4 mg/kg body weight). Kidney re-biopsy, at that time, showed a decrease in proportion of glomeruli affected with podocytopathy, but progression of interstitial lesions. After 23 weeks of therapy, partial remission of FSGS was attained and proteinuria dropped to 3.6 g/24 h. After 43 weeks, proteinuria decreased to 0.4 g/24 h and the serum creatinine concentration remained steady.
CONCLUSIONS: High-dose glucocorticoid therapy was effective in the initial treatment of COVID-19-related non-collapsing FSGS, but had no effect on interstitial changes. Introduction of cyclosporine A to the therapy contributed to remission of disease.
Keywords: Acute Kidney Injury, COVID-19, Cyclosporine, Glucocorticoids, nephrotic syndrome, Segmental Glomerulosclerosis, Apolipoprotein L1, COVID-19, Genotype, Glomerulosclerosis, Focal Segmental, Humans, Immunization, Passive, Male, Nephritis, Interstitial, SARS-CoV-2
Background
It is recognized that the SARS-CoV-2 virus can cause many adverse effects in organs other than the lungs, but it has been debatable whether these effects are directly mediated by presence of the virus or are secondary to immune system activation [1,2]. Acute kidney injury (AKI) can serve as an example of this. The details of the pathomechanism of its development in the course of COVID-19 have not been fully elucidated yet [2]. Data on its incidence vary considerably in different studies. One of the first observations was made in Wuhan, China and showed that AKI was present in 8.4% of infected patients and 3.6% of them required renal replacement therapy (RRT) [3]. Much higher numbers were presented in a retrospective study performed on a large cohort of 3993 patients with confirmed SARS-CoV-2 infection admitted to Mount Sinai Hospital; AKI was present in 46% of the patients and 19% required dialysis [4]. Regardless of its incidence, AKI greatly contributes to death in patients with COVID-19 [5,6]. Apart from a possible prerenal origin of AKI, more than half of patients with COVID-19-related AKI who required kidney biopsy were reported to have severe proteinuria, whereas hematuria was present in about 25% of cases [7]. These renal manifestations suggest the presence of glomerular injury in COVID-19-related AKI. The presence of glomerular disease was indeed confirmed in a series of patients, and most had podocytopathies. Focal segmental glomerulo-sclerosis (FSGS) with glomerular capillary collapse was the most common [7,8]. This disease was strongly associated with Black race and presence of APOL1 high-risk genotypes [7–9]. G1 and G2 high-risk alleles encoding the apolipoprotein L1 involved in innate immunity were found most frequently among patients of African descent [9,10]. West African ancestry determines increased probability of having the APOL-1 high-risk genotype [10]. Several reports indicated, however, that the occurrence of COVID-19 related glomerulopathy is not limited to people of Black race. One person of Hispanic ethnicity was also revealed to have a high-risk G2/G2 APOL1 genotype and collapsing FSGS [7]. The other patient whose APOL1 status was undetermined presented with FSGS without capillary collapse but required dialysis despite having the more favorable non-collapsing FSGS variant [7]. There are only a few reports of COVID-19-related FSGS in patients not of African descent [7,11]. Collapsing glomerulopathy is mostly associated with but not limited to the APOL1 high-risk genotype [7,8,10]. There are other genetic causes or epigenetic risk factors associated with collapsing FSGS, such as mutations in Scavenger Receptor Class B Member 2 (SCARB2) gene or Decaprenyl Pyrophosphate Synthetase Subunit 2 (PDSS2) gene, which is more frequent among White Americans than African Americans, or a decreased content of coenzyme Q10 in lymphoblastoid cell lines [12,13], but the majority of known COVID-19-related FSGS cases were in African Americans and had relatively short follow-up [7,8]. Information on COVID-19-associated glomerulopathies among non-Black people is scarce, which may reflect a lower incidence of this complication of SARS-CoV-2 infection in non-Blacks but does not exclude its existence. A case of an Asian Indian man with COVID-19 who had collapsing FSGS was reported, but variants of his APOL1 genes were not investigated and the patient was lost to follow-up [11]. Another Asian Indian man with undetermined APOL1 gene variants was initially diagnosed with minimal change disease, but as his renal function deteriorated and he became dialysis-dependent, despite prednisone therapy, kidney re-biopsy revealed collapsing FSGS [14]. A White man with COVID-19 had diffused crescentic Henoch-Schonlein purpura-associated nephritis, but information about his treatment and outcome is unknown [8]. A White female was diagnosed with minimal change disease, but because of low probability of having the APOL1 high-risk genotype, she was not tested for it [7], and she recovered after treatment with prednisone [7].
As presence or absence of SARS-CoV-2 RNA copies in the kidney parenchymal cells of 27 autopsied deceased patients with COVID-19 did not directly correspond with presence or absence of renal symptoms [1], one may conclude that a pathomechanism other than a direct viral activity is involved in kidney injury development. An intense immune response to SARS-CoV-2 infection with IFN-γ secretion, macrophage activation syndrome, and cytokine storm is one of the proposed mechanisms that may affect podocytes and trigger FSGS [2,15]. Therefore, immunosuppression with glucocorticoids aiming at reduction of circulating proinflammatory cytokine levels [16] may help in restoring proper podocyte function if an inflammation-related pathomechanism dominates.
In this report we present a case of a young White male who was diagnosed with AKI, FSGS, and interstitial nephritis in the course of COVID-19, manifesting with nephrotic syndrome, despite having the APOL1 low-risk genotype. He responded to glucocorticoid therapy with resolution of AKI and reduction of nephrotic proteinuria. A follow-up biopsy conducted after 5 months showed less intense glomerular involvement but progression of interstitial fibrosis and tubular atrophy.
Case Report
ADDITIONAL STUDIES:
Two samples of urine and 2 fresh, mechanically homogenized specimens of kidney parenchyma taken during the first kidney biopsy (14 days after presentation) were examined with rRT-PCR (with the previously-mentioned detection kit) for the presence of SARS-CoV-2. All urine and tissue samples were negative for viral RNA.
After obtaining the patient’s informed consent, genotyping for the apolipoprotein L1 (APOL1) G1 and G2 risk alleles was performed, as further described. Both risk alleles were absent and the gene sequence matched the hg19 reference sequence.
DNA was isolated from peripheral blood using a Maxwell® RSC instrument (Promega). Fragments of APOL1 gene (chr22: 36661747-36662448; 702bp) were amplified using forward GCCAGAGCCAATCTTCAGTC and reverse AATGTTTGCATTTGGGTCAA primer. PCR was performed in 25 μl with 1 μl of patient DNA, using standard reagents, including HotStarTaq DNA Polymerase (Qiagen), with a profile of 35 cycles and annealing at 59°C. Approximately 3 μl of the amplicons were visualized on 2.8% agarose gel. After enzymatic purification (EPPiC, A&A Biotechnology), PCR products were extended using the BigDye® 3.1 termination-ready reaction mix. Each sequencing reaction (20 μl) contained 4 μl of BigDye® mix, 30 ng of primer and 50 ng of the amplicon. The cycling conditions were as follow: initial denaturation at 95°C for 5 min was followed by 30 cycles at 95°C for 30 s, 58°C for 10 s, and 60°C for 4 min. Extension products were purified (BigDye XTerminator, Thermo Fisher Scientific) and analyzed using an ABI Prism 3130™ Genetic Analyzer. Sequences were edited and analyzed using BioEdit and MEGA 4: Molecular Evolutionary Genetics Analysis [17].
The patient was not tested for mutations in PDSS2 or SCARB2 genes since he had no neurological symptoms.
FOLLOW-UP:
The patient was followed up 6 times after discharge, at weeks 4, 12, 16, 19, 23, and 43. On the first visit to the clinic, he did not report any problems, and the physical examination was un-remarkable. The lungs were clear to auscultation at every visit. His arterial blood pressure, given as a mean of home self-measurements from the week preceding the visit, was satisfactory (Table 3). His 24-h proteinuria was 50% lower 4 weeks after discharge but remained the same after another 8 weeks, when trace leg edema and a slight increase in blood pressure became notable (Table 3). Since then, the enalapril dose was increased to 30 mg/day. Serum creatinine concentration and eGFR were relatively stable at all visits (Table 3). Urine sediment was bland every time. On the third visit, trace leg edema was still present, although 24-h proteinuria decreased by 40% compared to the previous measurement (Table 3). The patient reported clearly visible purple abdominal striae and elevated fasting glucose in his self-monitoring with a glucose meter. Glucose concentration controlled in fasting venous plasma was 5.5 mmol/L. After 16 weeks of prednisone therapy, the patient was concerned by its adverse effects, while only 1 criterion of partial remission was achieved, which was proteinuria reduction of more than 50% compared to discharge point, whereas it was still in the nephrotic range (Table 3). Therefore, kidney re-biopsy was considered to be helpful in making further therapeutic decisions, as an electron microscope evaluation was missing in the initial kidney biopsy. The patient was readmitted to the hospital 19 weeks after initial discharge, and kidney re-biopsy was performed. His leg edema had disappeared, 24-h proteinuria decreased again by 40% to 41 mg/kg of body weight, mean ACR from 2 morning spot urine samples were 16% less than on initial presentation and 60% smaller than on initial discharge, and serum albumin concentration increased by 43% compared to discharge level, but the patient still had hypoalbuminemia (Table 3). Oral glucose tolerance testing confirmed an impaired fasting glucose (IFG), likely secondary to steroid therapy. Besides abdominal striae, there was a marked weight gain and adipose tissue redistribution. Therefore, after re-biopsy, which showed remarkable podocytopathy and progression of chronic interstitial lesions, the patient was switched to 400 mg of cyclosporine A (4 mg/kg/day) in 2 divided doses. The prednisone dose was decreased by 10 mg/day, and further reduction by 5 mg every 2 weeks was advised. Nebivolol was increased to 5 mg/day for better blood pressure control, and a treatment with 500 mg of metformin twice a day was initiated for IFG. Four weeks later, the patient was seen again. His cyclosporine trough level was 107 ng/ml, and 24-h protein-uria decreased further by 10%. The patient reported no problems, and a physical examination was unremarkable, kidney function was stable, and arterial blood pressure was well controlled (Table 3). The prednisone dose was further gradually reduced. The last visit took place 43 weeks after the initial hospital discharge; the 24-h proteinuria was close to the criterion of complete remission, while serum creatinine was stable (Table 3). The residual dose of 5 mg/day of prednisone was maintained, while cyclosporine A was reduced to 300 mg/day in 2 divided doses. The immunosuppressive therapy during the entire follow-up included: 1) prednisone administered enterally in a dose of 60 mg/day for 19 weeks followed by reduction to 50 mg/day and further reductions by 5 mg/day every 2 weeks until the dose of 5 mg/day was reached at 38 weeks of follow-up; and 2) cyclosporine A, 400 mg/day from the 19th week and 300 mg/day from the 43rd week (Table 3).
Discussion
The patient was diagnosed with COVID-19 pneumonia, FSGS, and interstitial nephritis. We suspected that glomerular disease might have led to secondary tubulointerstitial nephritis, which in turn resulted in loss of kidney function and acute kidney injury. This pathomechanism is suggested by the clinical course, laboratory results, and kidney biopsy findings. FSGS complicating COVID-19 is not an unexpected finding in a proteinuric patient with severe infection; however, it has been previously reported nearly exclusively in Black patients and was often associated with presence of risk alleles G1 or G2 of a gene encoding apolipoprotein L1 [8,9,18–24]. Those alleles in homo-zygous or G1/G2 combination are thought to modify innate immune response in a way that predisposes to podocytopathy and collapsing variant of FSGS and is frequently complicated with acute kidney injury [7,9,18–24]. The presence of these alleles may serve as the “first hit”, while an intense immune response to SARS-CoV-2 infection can become the “second hit” triggering FSGS [8,21,22]. White patients, who very rarely have G1 and G2 alleles, and are not routinely screened for them, are unlikely to develop podocytopathy and FSGS in the course of COVID-19 and such cases have been very rare [7,11,14]. Our patient, who was genotyped and did not have the predisposing APOL1 alleles, might have other risk factors. Possibly, an episode of AKI and diagnosis of arterial hypertension 1 year earlier was a risk factor for COVID-19-related AKI, and until that time he had used anabolic steroids and was on a high-protein diet for body-building [25]. Anastrozole, which had been used by the patient, could have increased the risk for FSGS and arterial hypertension [26,27]. A variety of underlying diseases that predis-posed to COVID-19-dependent kidney injury were also reported by other authors [7,14]. The final triggering role of SARS-CoV-2 infection is suggested by a rapid increase of serum creatinine shortly before and after the patient’s admission to an emergency department, where a diagnosis of COVID-19 was made, and also by a marked decrease of serum albumin concentration and increase of urinary ACR and proteinuria during the 3-week hospitalization (Tables 1, 2). As the patient was not hypovolemic, prerenal AKI could be excluded. Instead, the intrarenal origin of the disease was indicated by active urine sediment on presentation, proteinuria, enlargement of both kidneys, and a decrease of kidney density in computed tomography. The patient was febrile on admission and had highly elevated acute phase markers such as serum CRP, ferritin, and fibrinogen concentration, without any marked increase of serum procalcitonin (Table 1), which is typical for virus-related cytokine storm. This could have an effect on podocytes, leading to their functional and ultrastructural changes, marked by the foot process effacement shown in electron microscopy. The good effects of immunosuppressive therapy support this theory. Other, earlier-reported cases of FSGS in COVID-19, although in APOL1 high-risk genotype patients, also suggested the immune reaction-related etiology of glomerulopathy. In most of these cases, SARS-CoV-2 was not found in renal parenchymal cells, which was verified by rRT-PCR, in situ hybridization for viral mRNA, or ultrastructural examination [7,8,18-24]. Based on these analyses, the probability of a direct viral infection is very low. In addition, in our case no viral material was found in homogenized samples of renal parenchyma and urine. In most FSGS cases in COVID-19 patients associated with the presence of G1 or G2 APOL1 risk alleles, biopsies showed glomerular capillary collapse and epithelial hypertrophy and hyperplasia in the Bowman space [18–23]. This subtype of FSGS is regarded as related to poor prognosis of renal survival. In our case, the patient was diagnosed with non-collapsing type of FSGS, but a single glomerulus in the first biopsy presented segmental capillary collapse and slight epithelial hypertrophy and hyperplasia in the Bowman space (Figure 2B). The intensity of lesions was low and not sufficient to diagnose a collapsing glomerulopathy. We may speculate that if glucocorticoid therapy had not been quickly introduced, this subtype of FSGS would have spread to most of the glomeruli and patient’s renal function could have rapidly worsened. Although the initial dexamethasone therapy based on the findings of the RECOVERY trial was given for the treatment of severe pneumonia and type 1 respiratory failure [28], it allowed a restoration of kidney function. The patient also received 2 units of COVID-19 convalescent plasma, which might have also contributed to the good effect of the therapy [29]. Despite the acute course of disease on presentation, we should keep in mind the other possible situation, where a patient could have had asymptomatic FSGS before SARS-CoV-2 infection, which remained undiagnosed until its aggravation was triggered by severe COVID-19. The available data do not lead us to completely reject this theory. Nevertheless, a rapid deterioration of renal function together with the morphological changes of the kidneys and onset of nephrotic syndrome have a strong relation to COVID-19. Glucocorticoid therapy, however, most probably would exert its effects in both scenarios. We can also speculate that even if the patient had high-risk APOL1 genotype, the same treatment, as applied, would be able to mitigate the progression of FSGS.
After the results of the first kidney biopsy became available and respiratory symptoms of COVID-19 subsided, the patient re-tested negative for SARS-CoV-2. The virus was absent in nasopharyngeal swab, samples of urine, and kidney parenchyma; nevertheless, extensive nephrotic proteinuria remained remarkable and life-threatening. Therefore, we considered FSGS in this case to be a primary disease, which needs an immunosuppressive treatment. SARS-CoV-2 infection appeared only as a trigger for FSGS, and since the virus was eliminated from body but nephrotic syndrome persisted, glomerulopathy should not have been considered as secondary to viral infection. Therefore, we initiated therapy with intravenous methylprednisolone followed by oral prednisone. After 19 weeks of treatment, serum creatinine remained normal and a more than 50% reduction of proteinuria was achieved (Table 3). Moreover, adverse effects of glucocorticoid therapy became a concern, especially glucose intolerance. Because the ultrastructural examination of glomeruli was not performed, we decided to perform a re-biopsy to confirm the diagnosis and to look for some prognostic and therapeutic hints. Taking into account the adverse effects of prednisone, laboratory results, and the re-biopsy findings, we concluded that a better cost/benefit ratio for the patient would come from further treatment with cyclosporine than with prednisone. Four weeks from the initiation of cyclosporine, proteinuria further decreased and eGFR remained stable (Table 3). The patient’s outcome was satisfactory, in contrast to many cases of COVID-19-associated FSGS, where patients had to initiate maintenance hemodialysis [7,8,14,18,21–23]. One study reported better prognosis related to less advanced interstitial fibrosis and tubular atrophy covering <30% of examined parenchyma [8]. The outcome in our patient, who had interstitial lesions covering 5% of parenchyma in the first biopsy and 15% in the re-biopsy, is in agreement with this observation. The progression of nonspecific tubulointerstitial changes after 19 weeks of glucocorticoid therapy may suggest reconsideration of the fact if this was only a case of tubulointerstitial nephritis secondary to FSGS or other concomitant tubulointerstitial disease. We cannot exclude the possibility that during the acute phase of COVID-19, cytokine storm, and hypoxia, before the first kidney biopsy was conducted, our patient had an acute tubular necrosis which led to the later aggravation of inflammation in the interstitium and enhanced fibrosis [30]. Autosomal dominant tubulointerstitial kidney disease (ADTKD) is the other possible condition which goes with interstitial fibrosis and tubular atrophy and, occasional, with microcystic dilatations. ADTKD, however, is an ultra-rare genetic disorder. It is confined to renal tubules and initially does not affect glomeruli. Glomerular secondary scarring is a relatively late symptom; therefore, proteinuria is minimal or mild, the opposite to the case of our patient. It tends to occur in families whereas our patient has a negative family history for kidney disease. On imaging studies, the kidneys are normal or small in size, while our patient had enlarged kidneys on presentation. In case of ADTKD, a slow progression of kidney disease is expected, whereas our patient presented a relatively steady serum creatinine concentration during follow-up visits [31]. Perhaps the third biopsy, if had been done after 43 weeks of follow-up (when the patient was close to complete remission), including 24 weeks of cyclosporine and slowly reduced glucocorticoid therapy, would have brought definitive information about disease activity and ultimate response to therapy, but it was not accepted by the patient.
Conclusions
The case presented shows that COVID-19 can evoke symptomatic non-collapsing subtype of FSGS in patients with risk factors for kidney disease other than the presence of G1 and G2 APOL1 alleles. It can manifest with nephrotic syndrome, interstitial nephritis, and AKI. Immunosuppressive treatment including glucocorticoids can induce partial remission of FSGS but not improve interstitial changes. The introduction of cyclosporine A to the therapy probably contributed to the remission of disease in this patient.
Figures
References:
1.. Puelles VG, Lütgehetmann M, Lindenmeyer MT, Multiorgan and renal tropism of SARS-CoV-2: N Engl J Med, 2020; 383(6); 590-92
2.. Kellum JA, van Till JWO, Mulligan G, Targeting acute kidney injury in COVID-19: Nephrol Dial Transplant, 2020; 35(10); 1652-62
3.. Hansrivijit P, Qian C, Boonpheng B, Incidence of acute kidney injury and its association with mortality in patients with COVID-19: A meta-analysis: J Investig Med, 2020; 68(7); 1261-70
4.. Chan L, Chaudhary K, Saha A, AKI in hospitalized patients with COVID-19: J Am Soc Nephrol, 2021; 32(1); 151-60
5.. Cheng Y, Luo R, Wang K, Kidney disease is associated with in-hospital death of patients with COVID-19: Kidney Int, 2020; 97(5); 829-38
6.. Fisher M, Neugarten J, Bellin E, AKI in hospitalized patients with and without COVID-19: A Comparison Study: J Am Soc Nephrol, 2020; 31(9); 2145-57
7.. Akilesh S, Nast CC, Yamashita M, Multicenter clinicopathologic correlation of kidney biopsies performed in COVID-19 patients presenting with acute kidney injury or proteinuria: Am J Kidney Dis, 2021; 77(1); 82-93.e1
8.. Nasr SH, Alexander MP, Cornell LD, Kidney biopsy findings in patients with COVID-19, kidney injury, and proteinuria: Am J Kidney Dis, 2021; 77(3); 465-68
9.. Shetty AA, Tawhari I, Safar-Boueri L, COVID-19-associated glomerular disease: J Am Soc Nephrol, 2021; 32(1); 33-40
10.. Genovese G, Friedman DJ, Pollak MR, APOL1 variants and kidney disease in people of recent African ancestry: Nat Rev Nephrol, 2013; 9(4); 240-44
11.. Deshmukh S, Zhou XJ, Hiser W, Collapsing glomerulopathy in a patient of Indian descent in the setting of COVID-19: Ren Fail, 2020; 42(1); 877-80
12.. Fogo AB, Causes and pathogenesis of focal segmental glomerulosclerosis: Nat Rev Nephrol, 2015; 11(2); 76-87
13.. Gasser DL, Winkler CA, Peng M, Focal segmental glomerulosclerosis is associated with a PDSS2 haplotype and, independently, with a decreased content of coenzyme Q10: Am J Physiol Renal Physiol, 2013; 305(8); F1228-38
14.. Gupta RK, Bhargava R, Shaukat AA, Spectrum of podocytopathies in new-onset nephrotic syndrome following COVID-19 disease: A report of 2 cases: BMC Nephrol, 2020; 21(1); 326
15.. Wright RD, Beresford MW, Podocytes contribute, and respond, to the inflammatory environment in lupus nephritis: Am J Physiol Renal Physiol, 2018; 315(6); F1683-94
16.. Liberman AC, Budziñski ML, Sokn C, Regulatory and mechanistic actions of glucocorticoids on T and inflammatory cells: Front Endocrinol (Lausanne), 2018; 9; 235
17.. Tamura K, Dudley J, Nei M, Kumar S, MEGA4: Molecular Evolutionary Genetics Analysis (MEGA) software version 4.0: Mol Biol Evol, 2007; 24(8); 1596-99
18.. Larsen CP, Bourne TD, Wilson JD, Collapsing glomerulopathy in a patient with COVID-19: Kidney Int Rep, 2020; 5(6); 935-39
19.. Kissling S, Rotman S, Gerber C, Collapsing glomerulopathy in a COVID-19 patient: Kidney Int, 2020; 98(1); 228-31
20.. Magoon S, Bichu P, Malhotra V, COVID-19-related glomerulopathy: A report of 2 cases of collapsing focal segmental glomerulosclerosis: Kidney Med, 2020; 2(4); 488-92
21.. Wu H, Larsen CP, Hernandez-Arroyo CF, AKI and collapsing glomerulopathy associated with COVID-19 and APOL1 high-risk genotype: J Am Soc Nephrol, 2020; 31(8); 1688-95
22.. Sharma Y, Nasr SH, Larsen CP, COVID-19-associated collapsing focal segmental glomerulosclerosis: A report of 2 cases: Kidney Med, 2020; 2(4); 493-97
23.. Peleg Y, Kudose S, D’Agati V, Acute kidney injury due to collapsing glomerulopathy following COVID-19 infection: Kidney Int Rep, 2020; 5(6); 940-45
24.. Couturier A, Ferlicot S, Chevalier K, Indirect effects of severe acute respiratory syndrome coronavirus 2 on the kidney in coronavirus disease patients: Clin Kidney J, 2020; 13(3); 347-53
25.. Herlitz LC, Markowitz GS, Farris AB, Development of focal segmental glomerulosclerosis after anabolic steroid abuse: J Am Soc Nephrol, 2010; 21(1); 163-72
26.. Kalender ME, Sevinc A, Camci C, Anastrozole-associated sclerosing glomerulonephritis in a patient with breast cancer: Oncology, 2007; 73(5–6); 415-18
27.. Lew R, Komesaroff P, Williams M, Endogenous estrogens influence endothelial function in young men: Circ Res, 2003; 93(11); 1127-33
28.. Horby P, Lim WS, Emberson JR, Dexamethasone in Hospitalized Patients with COVID-19: N Engl J Med, 2021; 384(8); 693-704
29.. Gupta A, Kute VB, Patel HV, Feasibility of convalescent plasma therapy in kidney transplant recipients with severe COVID-19: A single-center prospective cohort study: Exp Clin Transplant, 2021; 19(4); 304-9
30.. Wen Y, Yang C, Menez SP, A systematic review of clinical characteristics and histologic descriptions of acute tubular injury: Kidney Int Rep, 2020; 5(11); 1993-2001
31.. Devuyst O, Olinger E, Weber S, Autosomal dominant tubulointerstitial kidney disease: Nat Rev Dis Primers, 2019; 5(1); 60
Figures
Tables
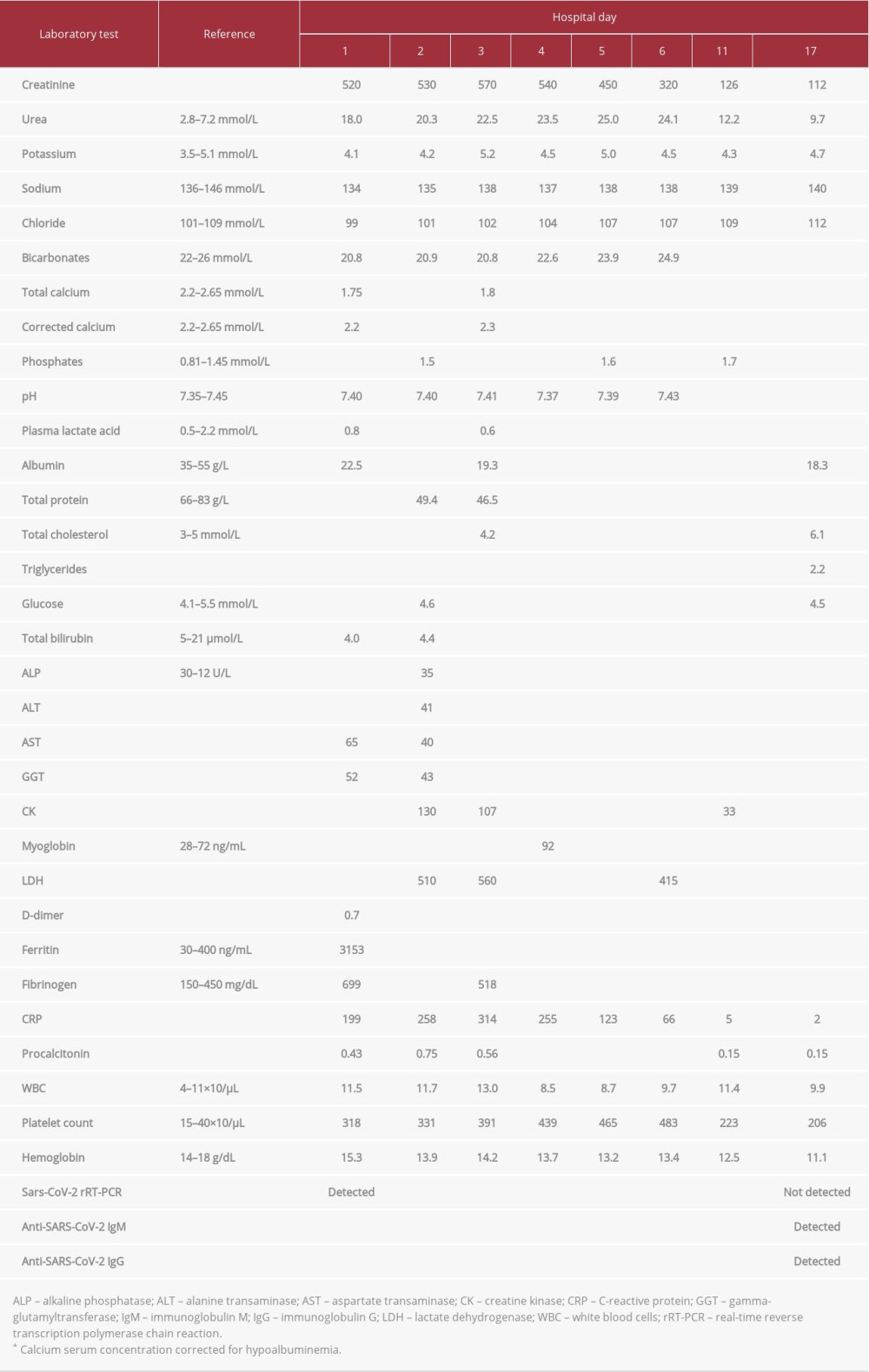 Table 1.. Summary of blood laboratory evaluations and relevant trends during hospitalization.
Table 1.. Summary of blood laboratory evaluations and relevant trends during hospitalization.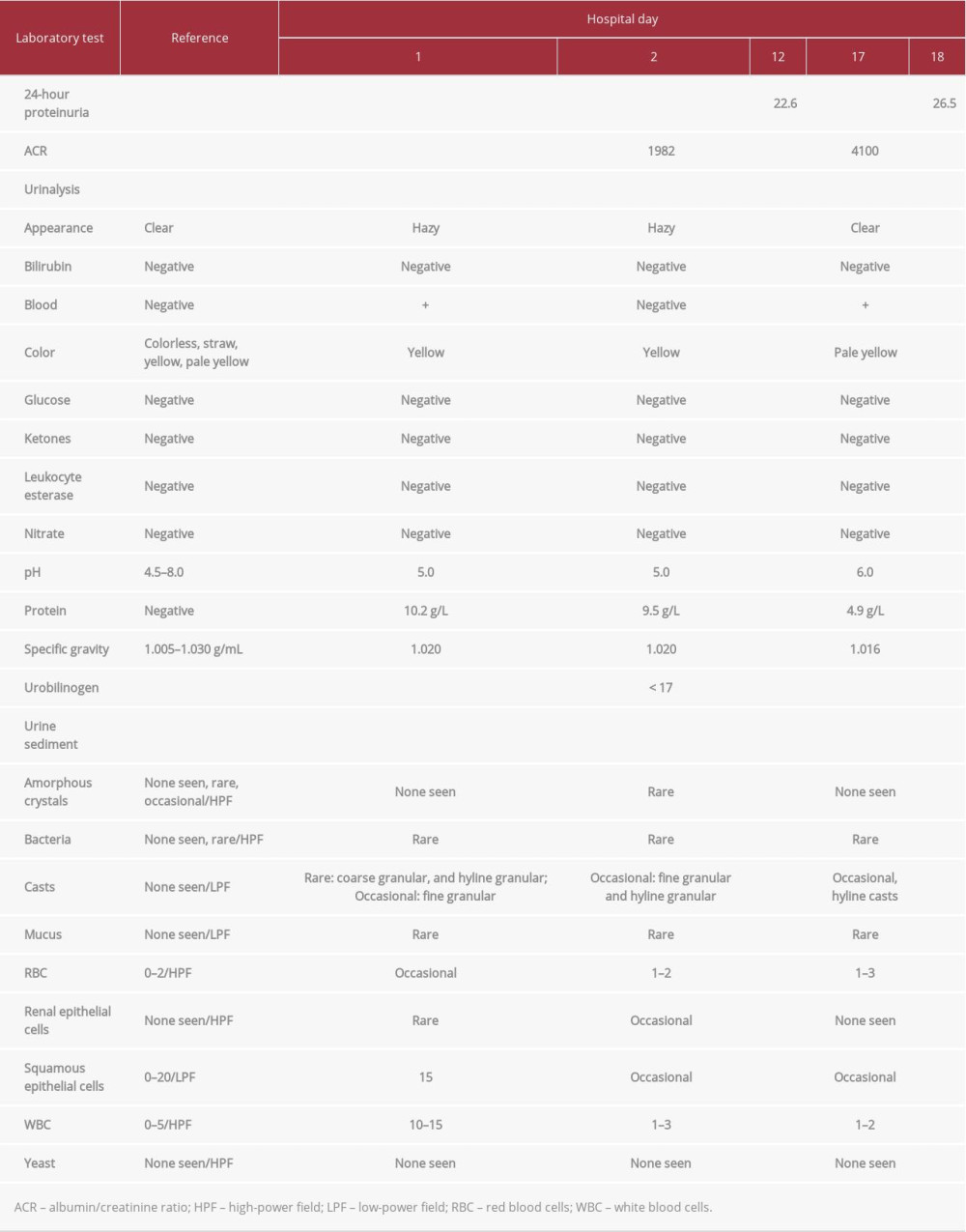 Table 2.. Summary of urine laboratory evaluations during hospitalization.
Table 2.. Summary of urine laboratory evaluations during hospitalization.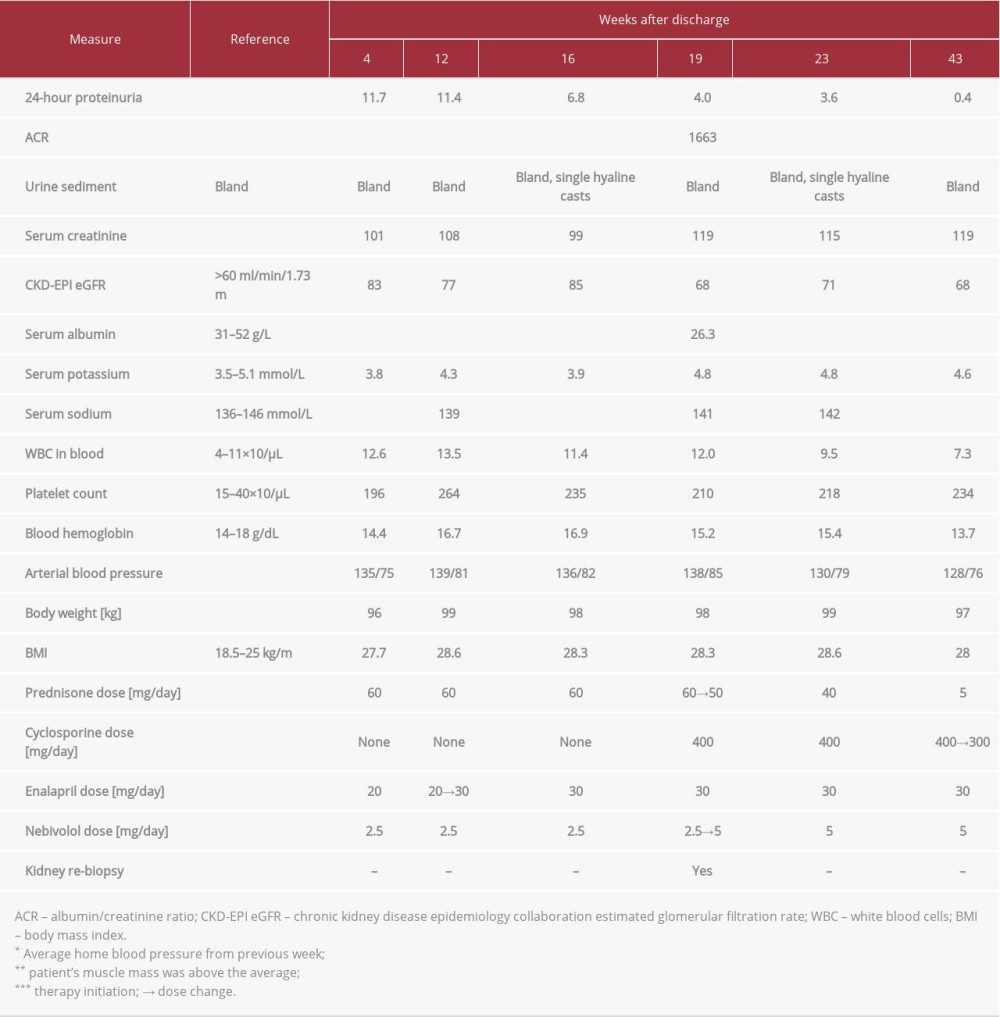 Table 3.. Summary of relevant parameters and main treatment during follow-up.Table 1.. Summary of blood laboratory evaluations and relevant trends during hospitalization.Table 2.. Summary of urine laboratory evaluations during hospitalization.Table 3.. Summary of relevant parameters and main treatment during follow-up.
Table 3.. Summary of relevant parameters and main treatment during follow-up.Table 1.. Summary of blood laboratory evaluations and relevant trends during hospitalization.Table 2.. Summary of urine laboratory evaluations during hospitalization.Table 3.. Summary of relevant parameters and main treatment during follow-up. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952507
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952041
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953137
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953095
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,827
22,760,827
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,468
176,468
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,758
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,804
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133