29 March 2025: Articles 
High Creatine Kinase Levels in Viral Myositis: A Case of Rhabdomyolysis-Induced Renal Failure
Unusual clinical course, Challenging differential diagnosis, Management of emergency care
Sujatha BaddamDOI: 10.12659/AJCR.946551
Am J Case Rep 2025; 26:e946551






Abstract
BACKGROUND: Viral infections can cause a spectrum of muscle involvement, from mild myalgia to severe conditions like rhabdomyolysis. While benign muscle pain is common, viral myositis complicated by rhabdomyolysis and acute kidney injury is an uncommon but serious occurrence. If not promptly recognized and treated, these complications can result in significant morbidity and even mortality. Timely diagnosis and intervention are crucial to mitigating the risks.
CASE REPORT: We present the case of a 47-year-old man with a history of recent flu-like symptoms, who developed generalized muscle pain and weakness. Upon further evaluation, he was diagnosed with acute viral myositis. His condition was complicated by severe rhabdomyolysis, as evidenced by a markedly elevated creatine phosphokinase (CPK) level of 880 300 U/L, which subsequently led to acute kidney injury. Despite immediate intervention with aggressive intravenous fluid resuscitation, he required emergency hemodialysis secondary to electrolyte imbalances. Over the course of several weeks, he required ongoing dialysis, but with continued treatment his renal function gradually improved, and dialysis was discontinued after 1 month.
CONCLUSIONS: This case highlights the importance of early recognition and treatment of viral myositis complicated by rhabdomyolysis and acute renal failure. Aggressive management, including fluid resuscitation and hemodialysis, is crucial in preventing life-threatening complications.
Keywords: creatine kinase, Myoglobinuria, myositis, Renal Dialysis, renal insufficiency, rhabdomyolysis, Humans, Male, Middle Aged, Acute Kidney Injury
Introduction
Viral myositis is a rare complication of viral infections, typically involving benign myalgia. However, in severe cases, viral myositis can progress to rhabdomyolysis, leading to acute kidney injury (AKI), electrolyte disturbances, and potentially life-threatening complications [1,2]. Acute viral myositis is most often associated with viruses such as influenza A and B, and while it is uncommon, the progression to rhabdomyolysis is even rarer [1–3]. Diagnosing viral myositis is challenging due to the absence of serological confirmation of viral agents, a highly variable differential diagnosis for the causes of rhabdomyolysis, and the lack of specific diagnostic indicators for virus-induced myositis in muscle biopsy. Patients affected by viral myositis may initially exhibit constitutional symptoms such as fatigue, fever, and malaise, which are associated with the systemic release of cytokines induced by the viral infection [3]. The hallmark of rhabdomyolysis is an elevated creatine phosphokinase (CPK) level, often exceeding 5 times the upper limit of normal. CPK levels are the most reliable objective indicator of rhabdomyolysis [4,5].
Patients with CPK levels of more than 40 000 IU/L have an increased risk of acute kidney injury. The most reliable predictors for the onset of acute kidney injury include hydration status, elevated initial serum creatinine, decreased serum bicarbonate and calcium levels, and elevated serum phosphate. Additionally, hypoalbuminemia and increased blood urea nitrogen have been linked to the development of acute kidney injury [5]. A large meta-analysis demonstrated a significant correlation between serum CPK levels and the likelihood of rhabdomyolysis-induced AKI, especially in traumatic cases [6]. The present case report illustrates the extreme severity of viral myositis, resulting in a CPK level of 880 300 U/L, one of the highest ever reported in the literature. We present the case of a patient with viral myositis complicated by rhabdomyolysis and acute kidney injury who required short-term dialysis, with subsequent recovery in kidney function. Early diagnosis and management are essential in such cases to prevent irreversible renal damage and other complications.
Case Report
A 47-year-old African American man with no significant past medical history presented to the Emergency Department (ED) with a 5-day history of flu-like symptoms, generalized muscle aches, and anorexia. Two days earlier, he had visited a local urgent care clinic, where he was diagnosed with an upper respiratory tract infection and prescribed doxycycline after receiving a dose of ketorolac. Despite taking acetaminophen and ibuprofen for symptom relief, his symptoms worsened, and he developed decreased urine output, prompting his visit to the ED. He denied vomiting, diarrhea, shortness of breath, trauma, intense exercise, recreational drug use, or alcohol use. His home medications included doxycycline, acetaminophen, and ibuprofen as needed. On examination, his vital signs were stable, with a blood pressure of 110/70 mmHg, heart rate of 89 beats/min, respiratory rate of 24/min, and temperature of 37.4°C. Physical examination revealed an ill-appearing man, not in apparent distress, with generalized muscle tenderness to palpation but no focal neurological deficits. His lungs were clear to auscultation. Heart sounds were normal. The abdomen was soft and non-tender with normal bowel sounds. No lower-extremity edema was noted.
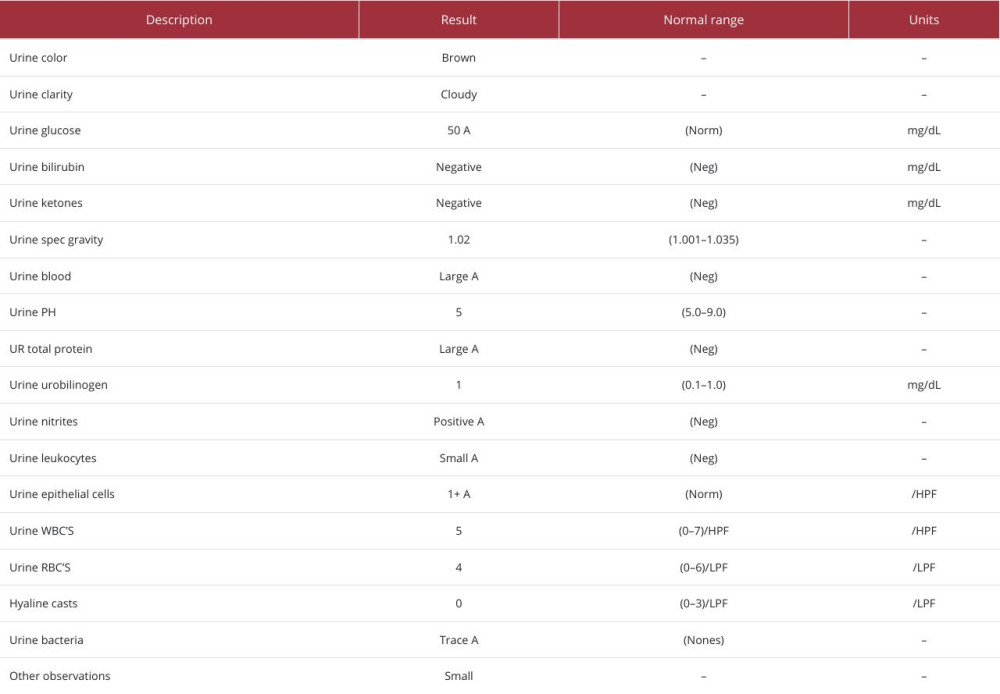
Initial laboratory investigations revealed severe electrolyte disturbances, including sodium 125 mmol/L, potassium 6.1 mmol/L, calcium 5.4 mg/dL, phosphorus 10.6 mg/dL, blood urea nitrogen 49 mg/dL, and creatinine 5.6 mg/dL. Liver function tests showed elevated aspartate aminotransferase at 2229 U/L and alanine aminotransferase at 605 U/L (Table 1). The patient’s CPK level was 872 100 U/L, with lactate dehydrogenase at 14 020 U/L. Urinalysis revealed large amounts of blood but only 4 red blood cells, consistent with myoglobinuria (Table 2). Chest X-ray results were normal, and electrocardiography showed normal sinus rhythm without peak T waves. The patient was diagnosed with acute kidney injury secondary to rhabdomyolysis-induced pigment nephropathy. He was given 3 L of normal saline intravenous fluids and started on maintenance fluids normal saline at 200 ml/h with the goal of maintaining a urinary flow of 200–300 mL/h. He underwent emergency hemodialysis immediately after admission due to severe acidosis and electrolyte imbalances. Despite these interventions, his CPK levels peaked at 880 300 U/L the following day.
A comprehensive diagnostic workup was performed to determine the cause of the patient’s rhabdomyolysis. A viral diatherix panel was negative (Table 3), and screenings for HIV, hepatitis, cytomegalovirus, Epstein-Barr virus, and mycoplasma were all negative. Thyroid-stimulating hormone and free thyroxine were within normal limits. Rheumatologic tests, including antinuclear antibody, double-stranded DNA, anti-Jo-1, anti-Mi-2, perinuclear antineutrophil cytoplasmic antibody (p-ANCA), and cytoplasmic antineutrophil cytoplasmic antibody (c-ANCA), were negative. Complement levels (C3 and C4) were normal. The MyoMarker panel was negative (Table 4). A urine drug screen was also negative. Urine and blood cultures were negative. A computed tomography (CT) scan of the abdomen and pelvis without contrast revealed a right hepatic and renal cyst, with no evidence of urolithiasis or obstructive uropathy (Figure 1). An abdominal ultrasound showed a possible hepatic hemangioma and diffuse increased echogenicity in the kidney (Figure 2). Electromyography (EMG) revealed no evidence of myopathy, and magnetic resonance imaging (MRI) of the brain was negative for any abnormality. Based on the exclusion of other causes, a final diagnosis of viral myositis complicated by rhabdomyolysis and pigment nephropathy was made.
In the ED, the patient was treated with intravenous fluids for aggressive fluid resuscitation and received treatment for hyperkalemia, including calcium gluconate, insulin with D50, and sodium zirconium cyclosilicate. He also received 150 m eq of sodium bicarbonate on admission, followed by 50 mmol of sodium bicarbonate for each subsequent 2–3 L of intravenous solution. Target fluid resuscitation was not achieved as he remained oliguric (urine output of less than 400 ml) for 4 days. Subsequently his urine output improved and the Foley catheter was removed on day 5 of admission, hence accurate urine output measurements were not available after removal of the Foley catheter. He was placed on continuous veno-venous hemofiltration (CVVH) with next-stage system on, with 8 L of therapy fluid rate per hour with a blood flow of 320 ml/min with no ultrafiltration for 4 days. On day 5, CRRT was stopped, and hemodialysis was resumed 3 days per week, starting on day 6. His CPK levels gradually declined (Figure 3), and he began to produce urine again. He was discharged home on day 12 with outpatient dialysis and follow-up with Nephrology. At the time of discharge, his CPK level had decreased to 2295 U/L, and his renal function continued to improve. He was advised to avoid nephrotoxic agents. One month later, he was able to discontinue hemodialysis, with his creatinine level stabilizing at 1.5 mg/dL after stopping dialysis. At the time of his first follow-up, he had returned to daily activities. He was advised to manage his AKI with lifestyle modifications while avoiding nephrotoxic agents to prevent further renal complications. Regular follow-ups with Nephrology were conducted to monitor renal function and track the progression of kidney function. Over the 2-year follow-up period, his renal function remained stable with CKD, and no additional complications were reported.
Discussion
We report a case of acute viral myositis complicated by rhabdomyolysis, electrolyte abnormalities, and acute renal failure requiring at least 4 weeks of hemodialysis. Our patient presented with a CPK level of 880 300 U/L, which is the highest CPK level reported in the medical literature secondary to acute viral myositis in an otherwise healthy young male. A thorough literature review was conducted to identify the highest CPK levels reported in patients with acute viral myositis.
Viral infections can cause diffuse muscle involvement, such as acute viral myositis, rhabdomyolysis, and inflammatory myositis. Common viruses associated with acute viral myositis include influenza A and B [1,2]. The exact mechanism of muscle necrosis in acute viral myositis is unknown, but it is presumed to involve direct invasion of muscle tissue by the viral agent or myotoxic cytokine release in response to the virus [2]. Although rare, acute viral myositis complicated by rhabdomyolysis has been reported with various viruses [3]. Viral symptoms may precede the onset of rhabdomyolysis by 1 to 14 days. Rhabdomyolysis is a syndrome involving skeletal muscle breakdown, resulting in the release of myoglobin into the systemic circulation. The classic triad of rhabdomyolysis consists of muscle pain, weakness, and red urine [4,5].
The diagnosis of viral myositis as a cause of rhabdomyolysis is based on clinical suspicion. Diagnostic evaluation for rhabdomyolysis includes measuring CPK levels and urinalysis (with dipstick and microscopic evaluation). The hallmark of rhabdomyolysis is the elevation of CPK and other muscle enzymes. Serum CPK levels are typically 5 times the upper limit of normal but can range from approximately 1500 to 100 000 IU/L [5]. Rhabdomyolysis is associated with hyperkalemia, hypocalcemia, hyperuricemia, and hyperphosphatemia. Hyperkalemia and hyperphosphatemia result from the release of potassium and phosphorus from damaged muscle cells. Muscle biopsy is not indicated in acute viral myositis as there are no specific findings. The differential diagnosis for rhabdomyolysis is also extremely variable. In adults, the most common causes are exertion, crush injury, alcohol and drug abuse, viruses, and statin use [5,7].
The mortality rate of rhabdomyolysis increases with increasing severity of the illness. One study reported 7.1% overall mortality in rhabdomyolysis, which increased to 22.5% in patients with renal failure and 40% in those that require renal replacement therapy [8]. Early intervention in cases of viral myositis complicated by rhabdomyolysis and acute renal failure is critical to improving patient outcomes. Prompt recognition of symptoms and initiation of treatment can significantly reduce the risk of severe complications, such as irreversible kidney damage or life-threatening electrolyte imbalances. Timely fluid resuscitation is essential in preventing acute kidney injury from progressing to chronic kidney disease [9]. In rhabdomyolysis, the release of myoglobin into the bloodstream can lead to tubular obstruction and direct toxic effects on the renal epithelium. Early and aggressive intravenous hydration helps to dilute the myoglobin concentration, promoting its clearance from the kidneys and reducing the likelihood of long-term renal impairment [5,10]. Early intervention can also mitigate other complications associated with rhabdomyolysis, such as hyperkalemia, which can lead to fatal cardiac arrhythmias if untreated. By promptly addressing electrolyte imbalances and providing appropriate supportive care, clinicians can prevent the escalation of these complications and improve overall survival rates. Patients who receive early treatment are more likely to experience a faster recovery, potentially leading to a shorter hospital stay and reduced need for prolonged interventions such as hemodialysis. This not only benefits the patient but also reduces the burden on healthcare resources.
One of the key limitations of this study is the lack of a definitive diagnosis, as our patient presented 5 days after the onset of symptoms. Unfortunately, viral testing was not performed during the patient’s initial visit to the urgent care clinic, which hindered the ability to identify the exact causative agent early in the course of the illness. This delay in testing limited our diagnostic precision and highlights the importance of early and thorough viral screening in similar cases. A person usually tests positive for influenza within 4 days of the first symptoms. Clinical evaluation and corroborative evidence from all the ancillary tests are needed for a definitive diagnosis. However, suspicion of viral etiology increases when muscle symptoms (weakness) develop acutely or sub-acutely after an antecedent respiratory or gastrointestinal infection. The idiopathic/ idiosyncratic cause of rhabdomyolysis in this case can be a differential diagnosis of viral myositis. Ibuprofen has been reported in the literature to provoke rhabdomyolysis in patients with carnitine palmitoyl transferase II deficiency (CPT II). CPT II deficiency is considered a common cause of metabolic myopathies and is caused by mutations in the gene encoding for this enzyme involved in fatty acid oxidation [11]. Since there was no evidence of myopathy on EMG, further genetic testing was not done. He also received a single dose of ketorolac and a total of 5–6 doses of 200 mg ibuprofen over the 5 days prior to admission. A large metanalysis demonstrated that mean non-steroidal anti-inflammatory drug exposure of 1–7 defined daily doses was associated with smaller hazard increases that were not significant [12]. No difference in the development of AKI was identified among participants who received at least 1 dose of ketorolac as compared to participants who did not receive any ketorolac [13]. Our patient was prescribed doxycycline at the urgent care clinic, but he did not take it. All other possible etiologies were excluded in our patient. Furthermore, muscle biopsy was not performed in this case, as viral myositis is often diagnosed based on clinical suspicion and elevated CPK levels. The clinical picture suggested a diagnosis of virus-induced rhabdomyolysis.
In comparison to the existing literature, this case stands out due to the extraordinarily high CPK levels, as most viral myositis-related rhabdomyolysis cases present with lower CPK elevations. A review of similar cases found that most patients with viral-induced rhabdomyolysis presented with CPK levels ranging from 10 000 to 100 000 U/L, significantly lower than the levels observed in our patient. However, his extremely high CPK level raises the question of whether another mechanism was a contributor, but no other contributor was identified. This case serves as a reminder that clinicians must remain vigilant for severe cases even when viral infections appear benign initially. This case underscores the importance of maintaining a high index of suspicion for rhabdomyolysis in patients presenting with viral symptoms and muscle pain, especially when accompanied by signs of renal impairment. Clinicians should be vigilant in monitoring creatine kinase levels and renal function in such patients, even in the absence of classic symptoms like dark urine or severe muscle weakness. The prognosis of rhabdomyolysis varies depending on the underlying cause. However, even with AKI, most patients have favorable outcomes, with complete recovery of kidney function.
Conclusions
Viral myositis complicated by rhabdomyolysis and acute kidney injury is a rare but serious condition that requires prompt diagnosis and management. Early intervention, including fluid resuscitation and dialysis when needed, is essential in preventing long-term renal damage and other complications. The use of antibiotics is not advised in cases of viral myositis, as they do not enhance the patient’s clinical outcomes or prognosis. Moreover, unnecessary antibiotic use can increase the risk of nephrotoxicity, further complicating the patient’s condition. This case, involving an extraordinarily high CPK level, serves as a reminder for clinicians to maintain a high index of suspicion for rhabdomyolysis in patients presenting with viral infections and muscle pain, even in the absence of classic symptoms like dark urine or severe muscle weakness. Our case highlights the need to consider checking CPK levels in hospitalized patients with viral infection on admission, particularly in patients with muscle pain or weakness. With early diagnosis and management, there is a possibility of recovery of kidney function in AKI cases associated with viral myositis and rhabdomyolysis.
Figures



References:
1.. Narayanappa G, Nandeesh BN, Infective myositis: Brain Pathol, 2021; 31(3); e12950
2.. Crum-Cianflone NF, Bacterial, fungal, parasitic, and viral myositis: Clin Microbiol Rev, 2008; 21(3); 473-94
3.. Kietaibl AT, Fangmeyer-Binder M, Göndör G, Acute viral myositis: Profound rhabdomyolysis without acute kidney injury: Wien Klin Wochenschr, 2021; 133(15–16); 847-50
4.. Cervellin G, Comelli I, Benatti M, Non-traumatic rhabdomyolysis: Background, laboratory features, and acute clinical management: Clin Biochem, 2017; 50(12); 656-62
5.. Stanley M, Chippa V, Aeddula NR, Rhabdomyolysis.: StatPearls [Internet]., 2024, Treasure Island (FL), StatPearls Publishing 2023 Apr 16.
6.. Safari S, Yousefifard M, Hashemi B, The value of serum creatine kinase in predicting the risk of rhabdomyolysis-induced acute kidney injury: A systematic review and meta-analysis: Clin Exp Nephrol, 2016; 20(2); 153-61
7.. Bhai S, Dimachkie MM., Rhabdomyolysis: Clinical manifestations and diagnosis., 2024, Waltham (MA), UpToDate UpToDate [Internet]. Dashe JF, deputy editor.
8.. McMahon GM, Zeng X, Waikar SS, A risk prediction score for kidney failure or mortality in rhabdomyolysis: JAMA Intern Med, 2013; 173(19); 1821-28
9.. Rodríguez E, Soler MJ, Rap O, Risk factors for acute kidney injury in severe rhabdomyolysis.: PLoS One, 2013; 8(12); e82992
10.. Bosch X, Poch E, Grau JM, Rhabdomyolysis and acute kidney injury: N Engl J Med, 2009; 361(1); 62-72 [Erratum in: N Engl J Med. 2011;364(20):1982]
11.. Ivin N, Della Torre V, Sanders F, Youngman M, Rhabdomyolysis caused by carnitine palmitoyltransferase 2 deficiency: A case report and systematic review of the literature: J Intensive Care Soc, 2020; 21(2); 165-73
12.. Nelson DA, Marks ES, Deuster PA, Association of nonsteroidal anti-inflammatory drug prescriptions with kidney disease among active young and middle-aged adults: JAMA Netw Open, 2019; 2(2); e187896
13.. Baddam S, Aban I, Hilliard L, Acute kidney injury during a pediatric sickle cell vaso-occlusive pain crisis: Pediatr Nephrol, 2017; 32(8); 1451-56
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133