09 July 2025: Articles 
Selective IgA Deficiency Complicated with Pernicious Anemia Diagnosed After Febrile Non-Hemolytic Transfusion Reaction
Rare disease
Yuta YoshinoDOI: 10.12659/AJCR.947678
Am J Case Rep 2025; 26:e947678






Abstract
BACKGROUND: Selective immunoglobulin A deficiency (SIgAD) is the most common primary immunodeficiency. However, most people with SIgAD are asymptomatic, and it is typically diagnosed during screening for blood donations or unexpected transfusion reactions. Screening programs for IgA deficiency have not yet been established, and the exact etiology of IgA deficiency remains unclear.
CASE REPORT: We report a case of SIgAD in a man who was diagnosed after a febrile non-hemolytic transfusion reaction (FNHTR) during erythrocyte transfusion for severe anemia. A 70-year-old man with a history of surgery for gastric carcinoid and sigmoid colon cancer presented to our hospital with persistent fatigue and general malaise for 2 months. A blood test revealed severe anemia with hyperbilirubinemia at the first visit to our hospital, and an erythrocyte transfusion was performed. A fever of 39.4°C with shivering was observed 30 min after the start of the transfusion. On day 20 after discharge, the serum IgA level was <3 µg/dL, indicating a high probability of IgA deficiency. He also tested positive for serum anti-IgA antibodies, leading to a diagnosis of SIgAD.
CONCLUSIONS: The cause of transfusion reaction should be immediately investigated, and the physician needs to learn about the epidemiology of transfusion reaction. Once the cause of transfusion reaction is identified, appropriate instruction should be provided for the patient to avoid transfusion reactions, and patients with SIgAD may benefit from wearing a medical alert bracelet.
Keywords: Anemia, Pernicious, IgA Deficiency, Transfusion reaction, Humans, Male, Aged, Erythrocyte Transfusion, Fever
Introduction
Selective immunoglobulin A deficiency (SIgAD) is the most frequent primary immunodeficiency [1], with an estimated prevalence of approximately 1: 150–1: 3000 [2]. In Japan, the incidence of SIgAD ranges from 1: 14840 to 1: 18500, which is lower than that observed worldwide [3]. SIgAD differs from other immunodeficiencies in that more than 50% of patients with SIgAD do not present with clinical symptoms and remain undiagnosed [4]. In most SIgAD cases, low levels of serum IgA are observed in asymptomatic individuals during screening for blood donations [5]. SIgAD is defined as a serum IgA level <7 mg/dL in patients aged >4 years with normal levels of serum IgG and IgM. In addition, patients with SIgAD have a normal vaccine response, excluding secondary causes of hypogammaglobulinemia and T-cell deficiency [6].
Although the pathogenesis of IgA deficiency remains unclear, it has been hypothesized that a defect occurs during the differentiation of B cells into IgA-secreting plasma cells [7]. IgA plays an important role in mucosal immunity; however, its deficiency does not lead to frequent and severe infections. The diagnosis of IgA deficiency is based on serum IgA levels and not on mucosal levels of secretory IgA. Therefore, individuals diagnosed with SIgAD may have sufficient amounts of IgA to protect their mucosal systems [8]. Furthermore, IgA-deficient cases might show increased production of secretory IgM as a compensatory mechanism [9]. However, it is unclear whether IgM can completely replace IgA. Fadlallah et al [10] found that IgM cannot efficiently bind all bacteria targeted by IgA in the intestinal tract. Although IgM cannot fully complement the function of IgA, it is suggested that IgM can maintain intestinal homeostasis by maintaining intestinal bacterial diversity.
Screening programs for IgA deficiency have not yet been established, and the exact etiology of IgA deficiency remains unclear [11]. Herein, we report a case of SIgAD in a man who was diagnosed following a febrile non-hemolytic transfusion reaction (FNHTR) during erythrocyte transfusion for severe anemia. After hospital admission, the cause of severe anemia was found to be pernicious anemia.
Case Report
A 70-year-old man with a history of surgery for gastric carcinoid and sigmoid colon cancer presented to our hospital with persistent fatigue and general malaise for 2 months. Three days before visiting the hospital, he visited a local gastroenterologist for persistent loss of appetite and a sore tongue. Although he had no taste disorder, his blood test results indicated severe anemia with hemoglobin level of 5.2 g/dL. A local gastroenterologist performed esophagogastroduodenoscopy (EGD) in the clinic. As no peptic ulcers or gastric neoplasms were observed, a further search for the cause of the anemia was necessary. The patient was referred to the Department of Internal Medicine of our hospital. At presentation, the Glasgow Coma Scale (GCS) score was 15/15. His vital signs were: body temperature 37.1°C, blood pressure 100/62 mmHg, heart rate 79/min, respiratory rate 18/min, and SpO2 96%. Physical examination revealed jaundiced skin and no palpable enlarged lymph nodes on the body surface. The surface of the tongue was not dry, and no papillary atrophy was observed. A blood test revealed macrocytic anemia (hemoglobin 5.0 g/dL, reticulocyte count 3.21×104/μL, and mean corpuscular volume 113.5 fL) with hyperbilirubinemia. The total bilirubin level was 2.2 mg/dL, with a direct bilirubin level of 0.8 mg/dL. Other results of blood tests presented a blood platelet count of 5.8×104/μL and lactate dehydrogenase levels of 3220 U/L, suggesting the presence of hematopoiesis disorder and/or hemolysis (Table 1). The direct Coombs test was negative, and erythrocyte transfusion was performed after confirming cross-matching with irregular antibodies. A fever of 39.4°C with shivering was observed 30 min after the start of the transfusion. The transfusion was stopped immediately. After sampling blood cultures, 1 g of meropenem was administered empirically, and the patient was admitted to the hospital.
Fever during erythrocyte transfusion was considered FNHTR because it developed in the middle of the transfusion rather than immediately after the transfusion began. Although this symptom appeared to be due to an allergic reaction following transfusion, the definite cause remained unclear. Plasma proteins and antibodies that could cause transfusion reactions were analyzed with the blood samples that had been taken before the transfusion. Sepsis was a possible cause; however, as blood cultures were negative on the third day of admission and the fever resolved, antimicrobial treatment was discontinued on the fourth day of admission.
The severe anemia was investigated as hemolytic anemia secondary to pernicious anemia or thrombotic microangiopathy (TMA). Hypersegmentation of polymorphonuclear leukocytes and erythrocyte fragmentation were observed in peripheral blood smears. However, no platelet aggregation was observed. Additional blood tests revealed low levels of haptoglobin, suggesting hemolysis, with normal disintegrin-like and metalloproteinase with thrombospondin type 1 motifs 13 activity and normal levels of complement C3 and C4. In addition, antinuclear and anticardiolipin antibody test results were negative. Whole-body contrast-enhanced computed tomography did not reveal abnormally enlarged lymph nodes or internal malignancies. TMA was ruled out, and vitamin B12 deficiency was subsequently recognized as the cause of macrocytic anemia (Table 2).
Another EGD performed at our hospital revealed atrophic gastritis consistent with autoimmune gastritis, with more significant mucosal atrophy in the upper stomach and the fornix than in the pyloric region (Figure 1). Pathological examinations of the biopsy samples obtained from the pyloric region revealed partial intestinal metaplasia, and no loss of pyloric glands was observed (Figure 2A). Fundic glands were not observed in a biopsy of the upper stomach, indicating strong atrophy (Figure 2B). Immunohistochemically, an increase in chromogranin A-positive cells, an indicator of enterochromaffin-like cells, was observed from the upper stomach to the fornix and pyloric regions (Figure 3A, 3B). A biopsy of the pyloric region revealed hyperplasia of gastrin-positive cells, whereas a loss of gastrin-positive cells was observed from the upper stomach to the fornix (Figure 4A, 4B). Although anti-parietal cell antibodies (APCA) and anti-intrinsic factor antibodies (AIFA) were negative, the pathological manifestations led to a diagnosis of pernicious anemia.
Intravenous vitamin B12 at 500 μg/dose was initiated on day 1 of admission and administered every other day throughout the hospitalization. No additional transfusions were performed during hospitalization because IgA deficiency was suspected based on serum IgA levels being below the sensitivity range of the assay. The hemoglobin level increased to 7.4 g/dL following intravenous vitamin B12 administration, and the patient was discharged on hospital day 11. Weekly intramuscular vitamin B12 administration was provided for the first month after leaving the hospital. Increases in reticulocyte and platelet counts, along with an improvement in pernicious anemia, were observed (Table 3). The clinical course following vitamin B12 administration could be explained by pseudo-TMA caused by pernicious anemia.
On day 20 after discharge, the results of outsourced testing were reported. The serum IgA level was < 3 μg/dL, indicating a high probability of IgA deficiency, and he tested positive for serum anti-IgA antibodies of isotype IgG, leading to a diagnosis of SIgAD. He was subsequently informed of having SIgAD and the high risk of transfusion reactions due to erythrocyte transfusion. He was advised to wear a medical alert bracelet to avoid the risk of transfusion reactions, but chose not to. Vitamin B12 intramuscular infusion for pernicious anemia was given every 3 months and his hemoglobin levels returned to within the normal range.
Discussion
SIgAD was diagnosed following FNHTR caused by an erythrocyte transfusion in a patient with severe anemia of unknown etiology. One of the most important complications of SIgAD is its well-known clinical association with autoimmune diseases, such as celiac disease and rheumatoid arthritis [12]. Inflammatory bowel diseases, primarily ulcerative colitis, are also reportedly associated with SIgAD [13]. Although no autoantibodies were detected in our patient, severe anemia due to vitamin B12 deficiency was diagnosed as pernicious anemia upon histopathological examination of the stomach. Pernicious anemia is a rare complication of SIgAD. However, systematic reviews [14,15] have indicated a relationship between pernicious anemia and SIgAD. In the present case, it was difficult to explain the association between SIgAD and pernicious anemia because APCA and AIFA were not detected. It may be helpful to make a histopathological diagnosis of pernicious anemia in SIgAD cases with vitamin B12 deficiency even if autoantibodies are serologically negative.
Transfusion reactions can occur in any patient. Acute hemolytic transfusion reaction (AHTR) can develop with fever and shivering during transfusion. Transfusion should be interrupted immediately following a fever on transfusion [16]. The most commonly reported cause of AHTR is major ABO mismatch of red blood cells due to human error, causing intravascular hemolysis [17]. Although the incidence of AHTR has now decreased due to blood product control systems, the fatality rate of AHRT remains high [18]. Once transfusion reaction has developed, the transfusion should be discontinued to search for the cause of transfusion reaction. At first, the possibility of a hemolytic transfusion reaction is explored. Then febrile diseases such as sepsis, which can be severe, are investigated. Once those are ruled out, the diagnosis of FNHTR is considered.
Transfusion reactions can develop in patients deficient in plasma proteins, such as IgA or haptoglobin, who produce antibodies to these proteins. In SIgAD cases, more severe transfusion reactions can develop in the presence of IgE-type anti-IgA antibodies [19]. Patients with SIgAD are recommended to undergo screening for anti-IgA antibodies before blood transfusions to assess the risk of blood product-induced antigen-antibody reaction [20]. If anti-IgA antibodies are present, IgA-free blood products from patients with IgA deficiency or serum washed with saline should be selected. Patients with SIgAD are recommended to wear medical alert bracelets to prevent secondary febrile non-hemolytic reactions to blood transfusions [21].
Conclusions
If systemic signs such as fever or shivering are present during or after blood transfusion, their relevance to transfusion should be considered. The cause of transfusion reaction should be immediately investigated, and the physician needs to learn about the epidemiology of transfusion reaction. Once the cause of transfusion reaction is identified, appropriate medical instruction should be provided for the patient to avoid transfusion reactions. Especially for patients with SIgAD, the benefits of wearing a medical alert bracelet should be stressed.
Figures
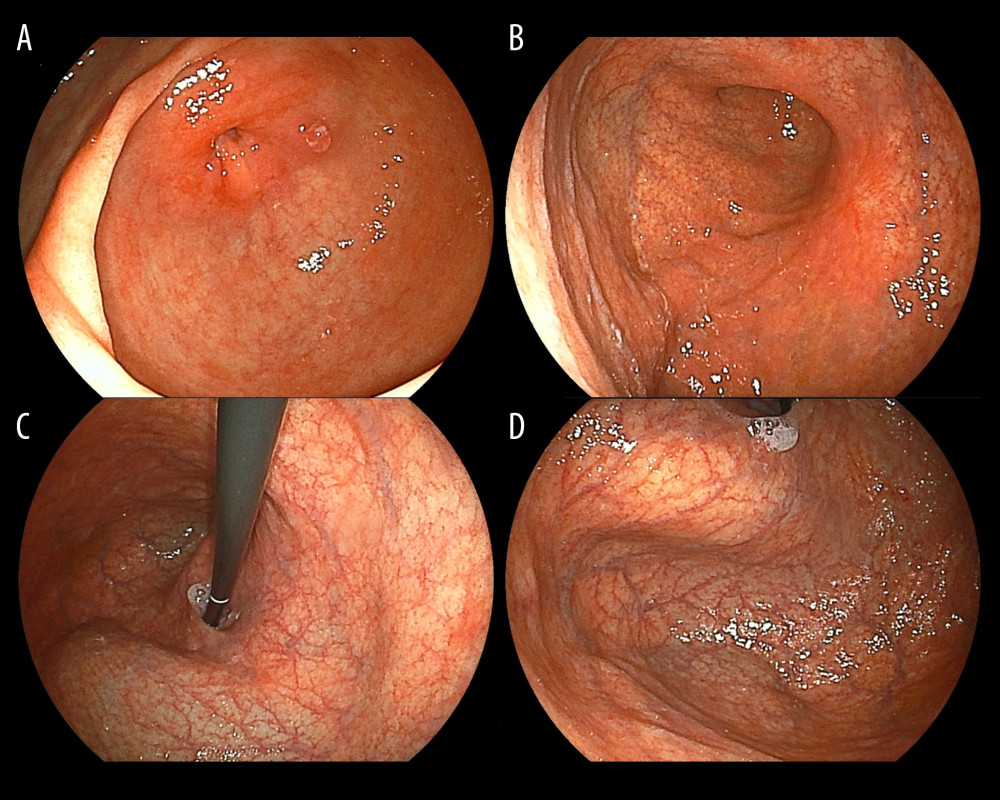 Figure 1. Images obtained using esophagogastroduodenoscopy. (A) Atrophic gastritis is not evident in the pyloric antrum. (B) A gastric ulcer scar was found on the posterior wall of the lower body of the stomach. (C, D) Severe atrophic gastritis was revealed in the upper stomach and the fornix.
Figure 1. Images obtained using esophagogastroduodenoscopy. (A) Atrophic gastritis is not evident in the pyloric antrum. (B) A gastric ulcer scar was found on the posterior wall of the lower body of the stomach. (C, D) Severe atrophic gastritis was revealed in the upper stomach and the fornix. 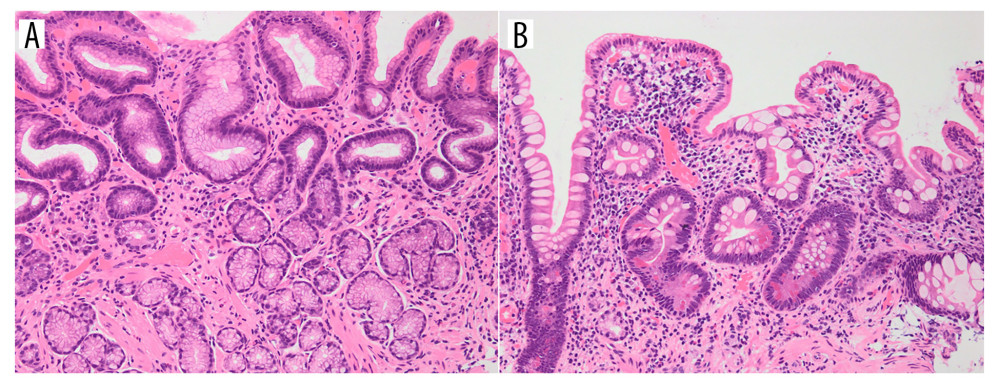 Figure 2. Histopathologic findings of biopsy samples obtained from the stomach. (A) Partial intestinal metaplasia and normal pyloric glands are observed in a biopsy sample obtained from the pyloric region (×400). (B) Hematoxylin and eosin staining of a biopsy sample from the fornix confirmed severe atrophy and loss of gastric fundic glands (×400).
Figure 2. Histopathologic findings of biopsy samples obtained from the stomach. (A) Partial intestinal metaplasia and normal pyloric glands are observed in a biopsy sample obtained from the pyloric region (×400). (B) Hematoxylin and eosin staining of a biopsy sample from the fornix confirmed severe atrophy and loss of gastric fundic glands (×400). 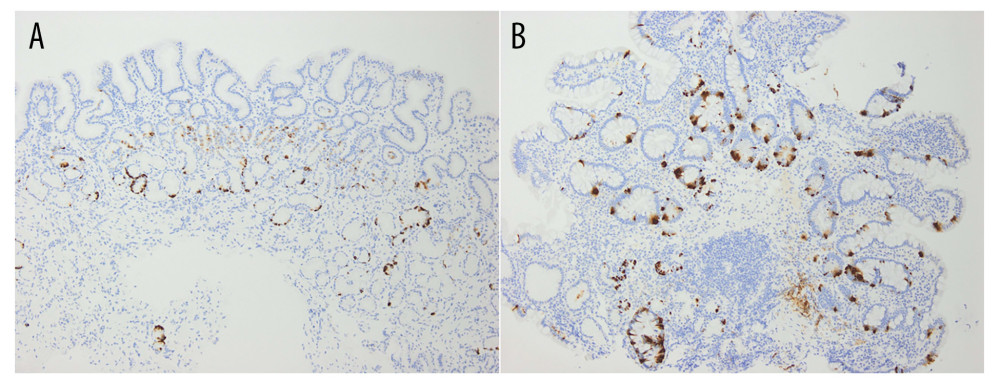 Figure 3. Results of the immunohistochemical staining for detecting chromogranin A. (A) A biopsy sample obtained from the pyloric region reveals an increase in chromogranin A-positive cells (×40). (B) Similarly, chromogranin A-positive cells are observed in the fornix (×40).
Figure 3. Results of the immunohistochemical staining for detecting chromogranin A. (A) A biopsy sample obtained from the pyloric region reveals an increase in chromogranin A-positive cells (×40). (B) Similarly, chromogranin A-positive cells are observed in the fornix (×40). 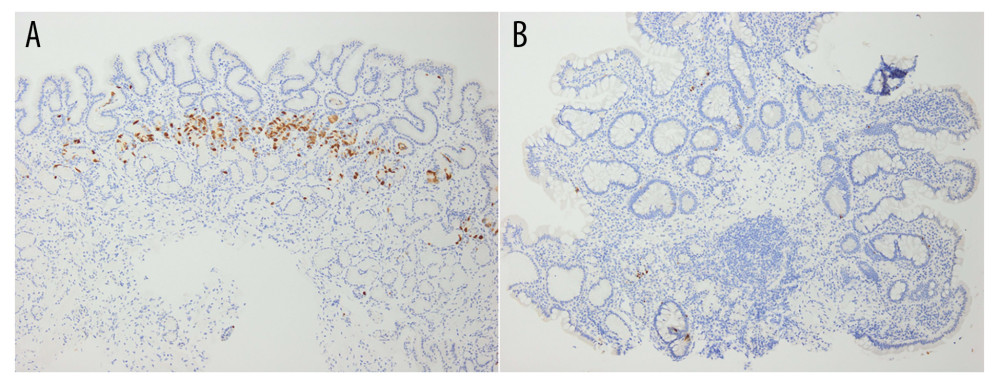 Figure 4. Results of the immunohistochemical staining for detecting gastrin. (A) Hyperplasia of gastrin-positive cells is observed in a biopsy sample obtained from the pyloric region (×40). (B) A loss of gastrin-positive cells is observed in the fornix (×40).
Figure 4. Results of the immunohistochemical staining for detecting gastrin. (A) Hyperplasia of gastrin-positive cells is observed in a biopsy sample obtained from the pyloric region (×40). (B) A loss of gastrin-positive cells is observed in the fornix (×40). References
1. Vo Ngoc DTL, Krist L, van Overveld FJ, The long and winding road to IgA deficiency: Causes and consequences: Expert Rev Clin Immunol, 2017; 13; 371-82
2. Morawska I, Kurkowska S, Bębnowska D, The epidemiology and clinical presentations of atopic diseases in selective IgA deficiency: J Clin Med, 2021; 10; 3809
3. Kanoh T, Mizumoto T, Yasuda N, Selective IgA deficiency in Japanese blood donors: Frequency and statistical analysis: Vox Sang, 1986; 50; 81-86
4. Abolhassani H, Aghamohammadi A, Hammarström L, Monogenic mutations associated with IgA deficiency: Expert Rev Clin Immunol, 2016; 12; 1321-35
5. Saghafi S, Pourpak Z, Aghamohammadi A, Selective immunoglobulin A deficiency in Iranian blood donors: Prevalence, laboratory and clinical findings: Iran J Allergy Asthma Immunol, 2008; 7; 157-62
6. Bonilla FA, Khan DA, Ballas ZK, Practice parameter for the diagnosis and management of primary immunodeficiency: J Allergy Clin Immunol, 2015; 136; 1186-205e1
7. Cunningham-Rundles C, Physiology of IgA and IgA deficiency: J Clin Immunol, 2001; 21; 303-9
8. Brandtzaeg P, Karlsson G, Hansson G, The clinical condition of IgA-deficient patients is related to the proportion of IgD- and IgM-producing cells in their nasal mucosa: Clin Exp Immunol, 1987; 67; 626-36
9. Klemola T, Immunohistochemical findings in the intestine of IgA-deficient persons: Number of intraepithelial T lymphocytes is increased: J Pediatr Gastroenterol Nutr, 1988; 7; 537-43
10. Fadlallah J, El Kafsi H, Sterlin D, Microbial ecology perturbation in human IgA deficiency: Science Translational Medicine, 2018; 10(439); eaan1217
11. Yazdani R, Azizi G, Abolhassani H, Selective IgA deficiency: Epidemiology, pathogenesis, clinical phenotype, diagnosis, prognosis and management: Scand J Immunol, 2017; 85; 3-12
12. Abolhassani H, Gharib B, Shahinpour S, Autoimmunity in patients with selective IgA deficiency: J Investig Allergol Clin Immunol, 2015; 25; 112-19
13. Aghamohammadi A, Cheraghi T, Gharagozlou M, IgA deficiency: Correlation between clinical and immunological phenotypes: J Clin Immunol, 2009; 29; 130-36
14. Swain S, Selmi C, Gershwin ME, The clinical implications of selective IgA deficiency: J Transl Autoimmun, 2019; 2; 100025
15. Vosughimotlagh A, Rasouli SE, Rafiemanesh H, Clinical manifestation for immunoglobulin A deficiency: A systematic review and meta-analysis: Allergy Asthma Clin Immunol, 2023; 19; 75
16. Gilliss BM, Looney MR, Gropper MA, Reducing noninfectious risks of blood transfusion: Anesthesiology, 2011; 115; 635-49
17. Sharma S, Sharma P, Tyler LN, Transfusion of blood and blood products: Indications and com plications: Am Fam Physician, 2011; 83; 719-24
18. Leo A, Pedal I, Diagnostic approaches to acute transfusion reactions: Forensic Sci Med Pathol, 2010; 6; 135-45
19. Sandler SG, Mallory D, Malamut D, IgA anaphylactic transfusion reactions: Transfus Med Rev, 1995; 9; 1-8
20. Yel L, Selective IgA deficiency: J Clin Immunol, 2010; 30; 10-16
21. Sandler SG, How I manage patients suspected of having had an IgA anaphylactic transfusion reaction: Transfusion, 2006; 46; 10-13
Figures
Figure 1. Images obtained using esophagogastroduodenoscopy. (A) Atrophic gastritis is not evident in the pyloric antrum. (B) A gastric ulcer scar was found on the posterior wall of the lower body of the stomach. (C, D) Severe atrophic gastritis was revealed in the upper stomach and the fornix.Figure 2. Histopathologic findings of biopsy samples obtained from the stomach. (A) Partial intestinal metaplasia and normal pyloric glands are observed in a biopsy sample obtained from the pyloric region (×400). (B) Hematoxylin and eosin staining of a biopsy sample from the fornix confirmed severe atrophy and loss of gastric fundic glands (×400).Figure 3. Results of the immunohistochemical staining for detecting chromogranin A. (A) A biopsy sample obtained from the pyloric region reveals an increase in chromogranin A-positive cells (×40). (B) Similarly, chromogranin A-positive cells are observed in the fornix (×40).Figure 4. Results of the immunohistochemical staining for detecting gastrin. (A) Hyperplasia of gastrin-positive cells is observed in a biopsy sample obtained from the pyloric region (×40). (B) A loss of gastrin-positive cells is observed in the fornix (×40). Tables
 Table 1. Hematological and biochemical test results.
Table 1. Hematological and biochemical test results. Table 2. Additional biochemical test.
Table 2. Additional biochemical test. Table 3. Timeline with recovery from cytopenia and key laboratory findings.Table 1. Hematological and biochemical test results.Table 2. Additional biochemical test.Table 3. Timeline with recovery from cytopenia and key laboratory findings.
Table 3. Timeline with recovery from cytopenia and key laboratory findings.Table 1. Hematological and biochemical test results.Table 2. Additional biochemical test.Table 3. Timeline with recovery from cytopenia and key laboratory findings. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133