02 July 2024: Articles 
A 68-Year-Old Man with Depression and Acute Renal Failure Due to Rhabdomyolysis Associated with Alcohol Intoxication While Taking Low-Dose Escitalopram: A Case Report
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Unexpected drug reaction
Daniela Cana RuiuDOI: 10.12659/AJCR.943422
Am J Case Rep 2024; 25:e943422






Abstract
BACKGROUND: Rhabdomyolysis, an uncommon but recognized adverse effect of selective serotonin reuptake inhibitor (SSRI) antidepressants, can precipitate acute renal injury (AKI), especially when combined with risk factors such as alcohol consumption. This report describes a 68-year-old man with acute renal failure due to rhabdomyolysis associated with alcohol intoxication while taking low-dose escitalopram, an SSRI antidepressant.
CASE REPORT: The patient, with a history of bipolar affective disorder managed with escitalopram, presented with symptoms of general malaise, diarrhea, myalgias, and transient loss of consciousness following substantial ethanol consumption. Laboratory tests indicated severe rhabdomyolysis with a creatine kinase level of 37 672 U/L and myoglobin level >5710 ng/ml, leading to an AKI diagnosis. The discontinuation of escitalopram, along with hydration and renal replacement therapy, facilitated renal recovery. However, the reintroduction of escitalopram resulted in the recurrence of rhabdomyolysis, suggesting a probable causal link, confirmed using the Naranjo Adverse Drug Reaction Probability Scale.
CONCLUSIONS: This report highlights the importance of identifying the medication history in patients presenting with acute renal failure and rhabdomyolysis and the association with SSRIs, which can be exacerbated by alcohol. This case underscores the importance of vigilant medication history assessment in patients presenting with AKI and rhabdomyolysis, particularly concerning the use of SSRIs like escitalopram, which can pose heightened risks in the context of alcohol use. It highlights the need for clinical caution in managing patients on long-term SSRI therapy, especially when reintroducing such medications after an episode of rhabdomyolysis.
Keywords: rhabdomyolysis, Acute Kidney Injury, escitalopram, olanzapine, case reports, Aged, Humans, Male, Alcoholic Intoxication, selective serotonin reuptake inhibitors
Introduction
Rhabdomyolysis is a clinical entity of significant complexity, requiring both a nuanced and expedient approach for early clinical and etiological diagnosis, as well as the prompt initiation of therapeutic measures [1]. These considerations are crucial, as they directly influence the prognosis and clinical trajectory of the patient. Within this syndrome, the lysis or dissolution of striated muscle is a central pathological event [2]. This breakdown leads to the leakage of large quantities of potentially toxic intracellular contents into the plasma and extra-cellular space [3,4]. Among these contents are molecules such as creatine kinase (CK), myoglobin, and a spectrum of electrolytes [1,5]. The clinical presentation of rhabdomyolysis is notably variable and cases can range from an asymptomatic condition [6] marked only by elevated levels of CK to severe [7], life-threatening scenarios featuring electrolyte imbalances, acute kidney injury (AKI), and disseminated intravascular coagulation [8,9]. The scope of this variability underlines the importance of timely diagnosis and treatment, making it an area ripe for clinical research and investigation. Various etiological factors contribute to rhabdomyolysis [10]. These include physical injury or trauma [11], severe burn injuries [12], electrocution [13], and high-intensity exercise [14]. Additionally, metabolic and endocrine disorders [5,15] such as hyperaldosteronism and hypothyroidism can also trigger this syndrome. Furthermore, a toxic etiology arising from medications like statins [16], antidepressants [17], and antivirals [18] is also well-documented, as are cases stemming from substance use disorders involving heroin, cocaine [19,20], and alcohol [4,21]. Cases have even been reported following prolonged periods of inactivity [22], such as in individuals who have fallen and remained immobile for an extended duration. Genetic predispositions, including McArdle disease and Duchenne muscular dystrophy, are other contributing factors and must be discussed when the patient has a family history of rhabdomyolysis [23,24]. Among these varied groups, substance abusers are particularly at risk for developing AKI due to non-traumatic rhabdomyolysis [25]. The role of myoglobin is pivotal in the pathophysiology of rhabdomyolysis-induced renal injury [26]. Once myoglobin enters the circulatory system following muscle injury, it is subject to glomerular filtration [27], which can lead to a cascade of adverse renal effects, such as tubular obstruction, renal inflammation, vasoconstriction, and, ultimately, severe renal dysfunction [28,29].
This report describes a 68-year-old man with AKI due to rhabdomyolysis associated with alcohol intoxication while taking low-dose escitalopram, a selective serotonin reuptake inhibitor (SSRI). This case is unique in that it involved the development of rhabdomyolysis subsequent to the administration of a psychiatric medication prescribed in small doses for several years. This emphasizes the importance of dynamic monitoring of renal function in this category of patients to identify a possible renal disorder.
Case Report
PATIENT INFORMATION:
A 68-year-old man was admitted to the Emergency Department presenting with a deteriorating general condition that had persisted for 2 days. Prior to admission, the patient had consumed a substantial amount of ethanol, experienced diarrhea, myalgias, and a transient loss of consciousness.
His family history included a father with hepatic neoplasm and a mother with colonic neoplasm. Notably, the patient had a long-standing history of bipolar affective disorder and had been on a consistent psychiatric medication regimen of Zyprexa (10 mg/day), Cipralex (10 mg/day), and Orfiril (1 g/day) for over 5 years. No other pathologies or treatments were noted. Psychosocial history revealed occasional ethanol use, with no history of smoking.
CLINICAL FINDINGS:
The clinical examination revealed a moderately altered general condition, overweight, with dehydration syndrome, diffusely hypotonic and painful muscles, hypokinesia, tremor of the extremities, mild polyarthralgia, no adenopathies, no changes in respiratory status, moderately elevated blood pressure values (systolic arterial blood pressure max 170 mmHg), tachycardia (98/min), diffuse sensitive abdomen with accelerated intestinal transit, and oliguria.
DIAGNOSTIC ASSESSMENT:
Laboratory tests indicated elevated CK at 37 672 U/L (normal range: <308 U/L), high lactic dehydrogenase at 1025 U/L (normal range: 135–225 U/L), and serum myoglobin at 5710 ng/ml (normal range: 23–72 ng/ml). These findings, along with hyperkalemia, hyperuricemia, proteinuria, and hematuria without bacteriuria, were suggestive of AKI secondary to toxic rhabdomyolysis, potentially exacerbated by medication and ethanol use. Imaging studies, including lung X-ray and abdominal and pelvic tomography, showed a right renal angiolipoma and pulmonary fibrosis, but no other significant changes. Primary diagnoses included AKI due to toxic rhabdomyolysis, bipolar affective disorder, hepatic cytolysis, acute enterocolitis, severe hyperuricemia, pulmonary fibrosis, and possible secondary arterial hypertension. The initial biological parameters are presented in Tables 1–3.
THERAPEUTIC INTERVENTIONS:
The patient was administered alkalinizing agents, isotonic saline for plasma volume restoration, and glucose solutions. Anti-inflammatory treatment began with solumedrol (250 mg/day) for 3 days and continued with prednisone (10 mg/day), tapered by 2.5 mg every 3–4 days. Additional medications included hypouricemics, analgesics, anticoagulants (low-molecular-weight heparin, fragmin 5000 IU/day), broad-spectrum antibiotics, and antihypertensives (ramipril 5 mg/day, nifedipine 20 mg/day). Psychiatric medications were discontinued upon hospital admission (day 1). Due to the oliguria, severe uremia, and electrolyte imbalances, renal replacement therapy was initiated (day 2). The patient underwent 1 hemodialysis session/day for 2 days, followed by 1 hemodiafiltration session/day for 4 days, to remove heavy molecules like myoglobin.
FOLLOW-UP AND OUTCOMES:
As a result of stopping the psychiatric medication (day 1) and applying therapeutic measures, the patient showed substantial clinical improvement, with stabilization of hemodynamic, respiratory, and psychiatric parameters. Reintroduction of olanzapine 10 mg/day (day 5) was successful (the values of creatinine and CK were in continuous remission). Renal function normalized, as did enzyme levels such as lactic dehydrogenase (LDH), CK, aspartate aminotransferase (ASAT), and alanine aminotransferase (ALAT), indicating remission from rhabdomyolysis (day 10). However, subsequent re-administration of escitalopram 10 mg/day (day 11) led to the recurrence of rhabdomyolysis (a new increase in creatinine and CK level), necessitating its discontinuation (day 16) (Figures 1, 2). With the purpose of standardized assessment of causality for adverse drug reactions, the Naranjo Adverse Drug Reaction Probability Scale (Naranjo Scale) was used, according to which the reaction was considered probable as a result of a score of 5–8 (Table 4, Figure 3).
Later complications included
Discussion
This case report illustrates the intricate relationship between the use of escitalopram, a SSRI, and the development of AKI due to rhabdomyolysis. Notably, the resurgence of symptoms upon the reintroduction of escitalopram provided a unique insight into the drug’s potential role as a precipitant for rhabdomyolysis in susceptible individuals. The pronounced elevations in CK and myoglobin, which were significantly above their normal ranges, played a crucial role in guiding clinical management. These findings echo those documented in the literature, where SSRIs have occasionally been implicated in similar cases [1,30].
Upon the initial discontinuation of escitalopram and the commencement of supportive hydration and renal replacement therapies, the patient’s clinical status improved markedly. This improvement, however, was reversed with the reintroduction of escitalopram. This temporal association highlights escitalopram’s role as a potential trigger for rhabdomyolysis, corroborated by reports in the literature in which reintroduction of SSRIs precipitated similar outcomes [31,32].
While concurrent factors such as alcohol consumption and dehydration are recognized contributors to the development of rhabdomyolysis, the present case specifically underscores the significant impact of escitalopram. This aligns with our analysis that prioritizes the examination of escitalopram’s role over less pertinent differential diagnoses such as pre-renal conditions and acute tubular necrosis (ATN), all of which were thoroughly evaluated and ruled out through detailed diagnostic assessments [33,34]. This rigorous approach reaffirms the necessity for vigilance when reintroducing medications known to potentially exacerbate underlying pathologies, especially in patients with a history of rhabdomyolysis.
The implications of this case are significant, highlighting the critical need for cautious medication management in patients with complex medical histories involving multiple medications and comorbid conditions. It also emphasizes the importance of ongoing research into the mechanistic pathways through which SSRIs like escitalopram can induce muscle breakdown and renal injury. This is particularly crucial when considering potential interactions with substances like alcohol, which can amplify the risks associated with SSRIs [31,32].
Despite the valuable insights provided by this case report, it is imperative to consider several limitations. The analysis is based on a single case, which may not be representative of broader patient populations. The unique circumstances and individual patient characteristics limit the generalizability of the results. The patient’s history of alcohol use and the presence of multiple comorbidities – bipolar affective disorder, hepatic cytolysis, and acute enterocolitis – introduce potential confounders that can significantly influence the development and severity of rhabdomyolysis.
Moreover, the patient was on a regimen of multiple medications, including Zyprexa and Orfiril, alongside escitalopram, complicating the potential interactions that might impact renal function and muscle health. The differential diagnosis was further complicated by the multifaceted etiology of rhabdomyolysis, attributable to a range of factors beyond medication use, such as physical trauma, infections, and metabolic disorders.
The subjective nature of the Naranjo Adverse Drug Reaction Probability Scale, although providing a structured approach to evaluating the likelihood of drug-induced adverse reactions, may not capture all nuances of the case. The lack of longitudinal follow-up data and the ethical constraints preventing a definitive re-challenge with escitalopram to confirm its role in causing rhabdomyolysis also limit the direct causality assessment.
These considerations underscore the need for cautious interpretation of the findings and advocate for further research, including larger observational studies, randomized controlled trials, and pharmacogenetic investigations, to elucidate the relationship between SSRIs like escitalopram and the risk of rhabdomyolysis.
Conclusions
This case report has highlighted the vital importance of detailed medication history assessment in patients who present with acute renal failure and rhabdomyolysis, specifically highlighting the potential exacerbating role of SSRIs such as escitalopram, especially when combined with alcohol consumption. The findings underscore the necessity for rigorous and ongoing renal function monitoring for individuals undergoing long-term treatment with psychiatric medications, regardless of dosage levels. Moreover, this case sheds light on the diagnostic complexities encountered with drug-induced rhabdomyolysis in scenarios of multiple comorbidities and extensive polypharmacy. The application of the Naranjo Adverse Drug Reaction Probability Scale in this case provided a structured approach to evaluating escitalopram’s role as a causative factor, reinforcing the need for careful consideration when reintroducing this medication after an episode of rhabdomyolysis. The compelling narrative of this case, which supports the hypothesis of escitalopram’s significant contribution to the patient’s condition, also calls for caution in extrapolating these findings to all psychiatric medications or broader patient populations. It is clinically advisable to perform regular assessments of renal function in patients on long-term therapy with escitalopram, particularly for those with additional risk factors. Any sudden changes in renal markers should trigger a thorough investigation for potential underlying causes, including rhabdomyolysis. Additionally, the reintroduction of escitalopram after rhabdomyolysis requires careful consideration, and exploring alternative therapeutic strategies may be warranted. Future research should aim to elucidate the mechanisms by which psychiatric medications like escitalopram interact with other drugs and medical conditions to induce rhabdomyolysis. Studies into pharmacogenetics may provide valuable insights into individual susceptibility to this adverse effect. Longitudinal studies monitoring renal function in patients receiving chronic escitalopram treatment could yield important data on the prevalence and risk factors associated with this rare but important complication. Developing predictive models or algorithms for early identification of patients at risk could significantly enhance clinical outcomes and patient safety.
Tables
Table 1.. Biological parameters: hematological parameters, kidney and liver function.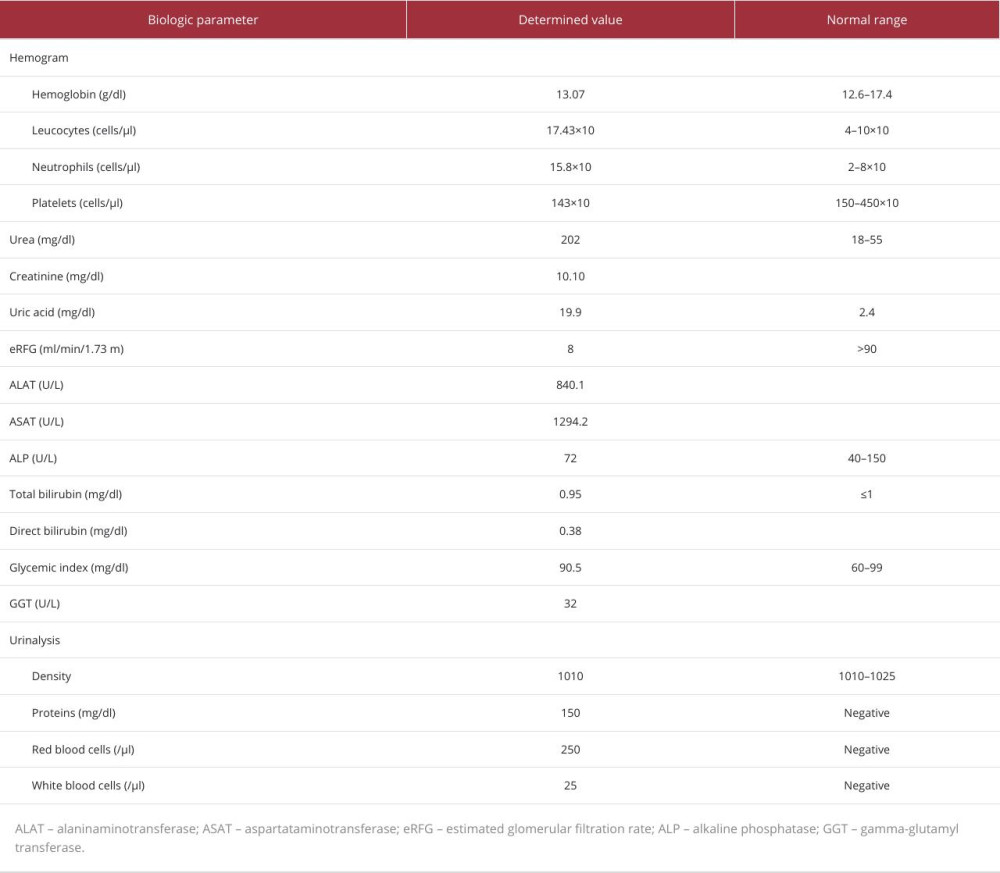 Table 2.. Biological parameters: acid-base and electrolyte balance, coagulation, infectious etiology.
Table 2.. Biological parameters: acid-base and electrolyte balance, coagulation, infectious etiology.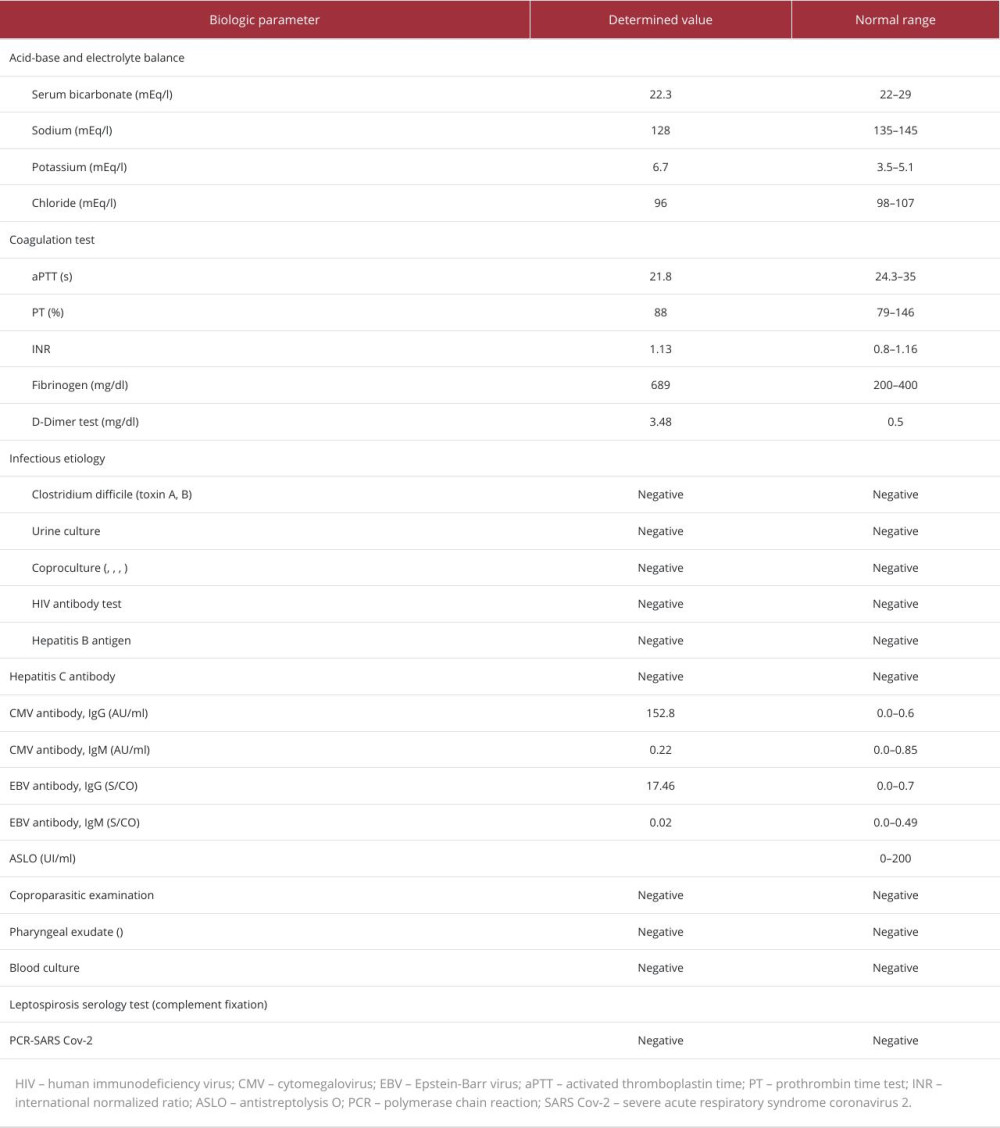 Table 3.. Biological parameters: immunological, inflammation and tumoral status.
Table 3.. Biological parameters: immunological, inflammation and tumoral status.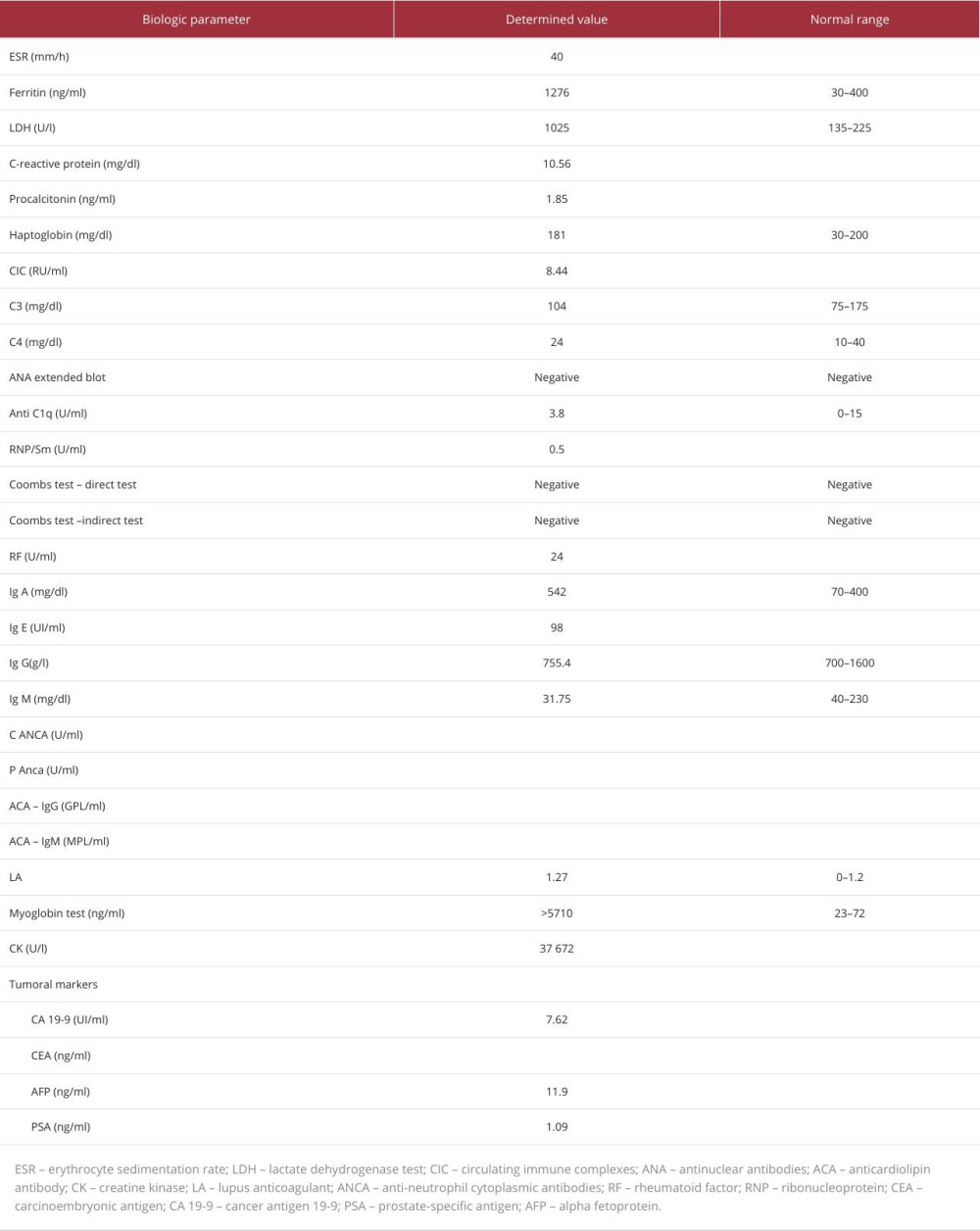 Table 4.. Naranjo Adverse Drug Reaction Probability Scale.
Table 4.. Naranjo Adverse Drug Reaction Probability Scale.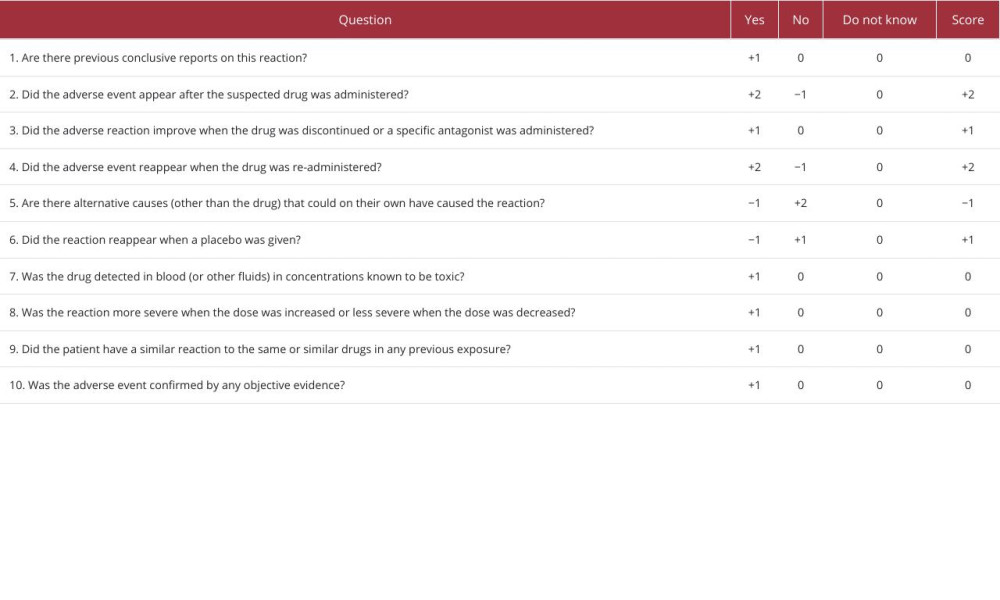
References:
1.. Eltayeb M, Sirag A, Alamin H, Elagib A, Management of rhabdomyolysis and acute renal failure following strenuous exercise in young adult: A case report: Open J Intern Med, 2023; 13(1); 23-31
2.. Gupta A, Thorson P, Penmatsa KR, Gupta P, Rhabdomyolysis: Revisited: Ulster Med J, 2021; 90(2); 61
3.. Al-Ismaili Z, Piccioni M, Zappitelli M, Rhabdomyolysis: Pathogenesis of renal injury and management: Pediatr Nephrol, 2011; 26; 1781-88
4.. Kodadek L, Carmichael SP, Seshadri A, Rhabdomyolysis: An American association for the surgery of trauma critical care committee clinical consensus document: Trauma Surg Acute Care Open, 2022; 7(1); e000836
5.. Sun L, Tang M, Peng M, Ritodrine-induced rhabdomyolysis and psychiatric symptoms: A case report and literature review: BMC Pregnancy Childbirth, 2023; 23(1); 1-7
6.. Sasaki R, Yunoki T, Nakano Y, A young female case of asymptomatic immune-mediated necrotizing myopathy: A potential diagnostic option of antibody testing for rhabdomyolysis: Neuromuscul Disord, 2023; 33(2); 183-86
7.. Cirillo E, Esposito C, Giardino G, Case report: Severe rhabdomyolysis and multiorgan failure after ChAdOx1 nCoV-19 vaccination: Front Immunol, 2022; 13; 845496
8.. Danaei B, Sharifi A, Mazloom H, Prevalence of compartment syndrome and disseminated intravascular coagulation following rhabdomyolysis; A systematic review and meta-analysis: Arch Acad Emerg Med, 2023; 11(1); e55
9.. Wang C, Yu B, Chen R, Association of D-dimer and acute kidney injury associated with rhabdomyolysis in patients with exertional heatstroke: An over 10-year intensive care survey: Ren Fail, 2021; 43(1); 1561-68
10.. Kruijt N, van den Bersselaar L, Kamsteeg E, The etiology of rhabdomyolysis: An interaction between genetic susceptibility and external triggers: Eur J Neurol, 2021; 28(2); 647-59
11.. Dantas GHM, de Alkmim Moreira Nunes R, Analysis of physiological markers and risk factors for the development of rhabdomyolysis in military personnel: A systematic review: Rev Environ Health, 2023; 38(4); 613-20
12.. Ko A, Song J, Golovko G, Higher risk of acute kidney injury and death with rhabdomyolysis in severely burned patients: Surgery, 2022; 171(5); 1412-16
13.. Romick J, Balogun R, Nye N, Evaluation and treatment of exertional heat illness, rhabdomyolysis, and hyponatremia: Endurance sports medicine: A clinical guide, 2023; 63-75, Springer
14.. Herrera-Olivares AM, Fernández-Luque JA, Combined HIIT and resistance training in very long-chain Acyl-CoA Dehydrogenase deficiency: A case report: Front Physiol, 2019; 10; 456034
15.. Díaz-López EJ, Villar-Taibo R, Rodriguez-Carnero G, Should we suspect primary aldosteronism in patients with hypokalaemic rhabdomyolysis? A systematic review: Front Endocrinol, 2023; 14; 1257078
16.. Safitri N, Alaina MF, Pitaloka DAE, Abdulah R, A narrative review of statin-induced rhabdomyolysis: Molecular mechanism, risk factors, and management: Drug Healthc Patient Saf, 2021; 13; 211-19
17.. Wang Y, Lin Y, Lin Q, Exploring the association between selective serotonin reuptake inhibitors and rhabdomyolysis risk based on the FDA pharmacovigilance database: Sci Rep, 2023; 13(1); 12257
18.. Qatomah A, Bukhari M, Cupler E, Acute reversible rhabdomyolysis during direct-acting antiviral hepatitis C virus treatment: A case report: J Med Case Rep, 2021; 15; 627
19.. Iftikhar MH, Dar AY, Haw A, Cocaine-induced rhabdomyolysis and compartment syndrome: BMJ Case Rep, 2022; 15(5); e249413
20.. Amanollahi A, Babeveynezhad T, Sedighi M, Incidence of rhabdomyolysis occurrence in psychoactive substances intoxication: A systematic review and meta-analysis: Sci Rep, 2023; 13(1); 17693
21.. Pigeaud L, de Veld L, van der Lely N, Elevated creatinine kinase levels amongst Dutch adolescents with acute alcohol intoxication: Eur J Pediatr, 2023; 182(3); 1371-75
22.. Isaacs AW, Myburgh KH, Macaluso F, Low-volume squat jump training improves functional performance independent of myofibre changes in inactive young male individuals: Healthcare (Basel), 2022; 10(7); 1217
23.. Harmelink M, Uncommon causes of rhabdomyolysis: Crit Care Clin, 2022; 38(2); 271-85
24.. Katz J, Labilloy A, Lee A, Recurrent, non-traumatic, non-exertional rhabdomyolysis after immunologic stimuli in a healthy adolescent female: A case report: BMC Pediatr, 2022; 22(1); 515
25.. Ahmad A, Zain MA, Ashfaq AA, A late presentation of substance-related rhabdomyolysis with normal serum creatine kinase levels and complicated with acute tubular necrosis: Cureus, 2019; 11(3); e4197
26.. Bajema IM, Rotmans JI, Histological manifestations of rhabdomyolysis in the kidney: Nephrol Dial Transplant, 2018; 33(12); 2113-14
27.. Nayak S, Jindal A, Myoglobinuria and acute kidney injury: J Integr Nephrol Androl, 2015; 2(2); 50
28.. Simpson JP, Taylor A, Sudhan N, Rhabdomyolysis and acute kidney injury: Creatine kinase as a prognostic marker and validation of the McMahon Score in a 10-year cohort: A retrospective observational evaluation: Eur J Anaesthesiol, 2016; 33(12); 906-12
29.. Ye Q, Gu C, Yan W, Meta-analysis of the pathogenesis and prognostic impact factors of rhabdomyolysis: Arch Clin Psychiatry, 2022; 49(4); 44-54
30.. Luckoor P, Salehi M, Kunadu A, Exceptionally high creatine kinase (CK) levels in multicausal and complicated rhabdomyolysis: A case report: Am J Case Rep, 2017; 18; 746
31.. Lewien A, Kranaster L, Hoyer C, Escitalopram-related rhabdomyolysis: J Clin Psychopharmacol, 2011; 31(2); 251-53
32.. Hart X, Heesen S, Schmitz C, Concentrations of escitalopram in blood of patients treated in a naturalistic setting: Focus on patients with alcohol and benzodiazepine use disorder: Eur Arch Psychiatry Clin Neurosci, 2023; 273(1); 75-83
33.. Sung DJ, Miyea L, Ji-Kang P, Hyun-Jung P, Combination of antidepressant and alcohol intake as a potential risk factor for rhabdomyolysis: Iran J Public Health, 2018; 47(9); 1423-24
34.. Tsai JP, Lee CJ, Subeq YM, Acute alcohol intoxication exacerbates rhabdomyolysis-induced acute renal failure in rats: Int J Med Sci, 2017; 14(7); 680
Figures
Tables
Table 1.. Biological parameters: hematological parameters, kidney and liver function.Table 2.. Biological parameters: acid-base and electrolyte balance, coagulation, infectious etiology.Table 3.. Biological parameters: immunological, inflammation and tumoral status.Table 4.. Naranjo Adverse Drug Reaction Probability Scale.Table 1.. Biological parameters: hematological parameters, kidney and liver function.Table 2.. Biological parameters: acid-base and electrolyte balance, coagulation, infectious etiology.Table 3.. Biological parameters: immunological, inflammation and tumoral status.Table 4.. Naranjo Adverse Drug Reaction Probability Scale. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133